
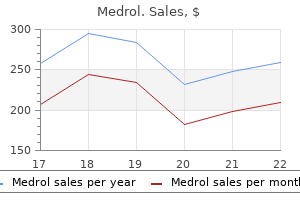
Discount 16mg medrol overnight delivery
Susceptible pregnant women exposed to varicella should be evaluated for use of varicella zoster immune globulin in the same way as the general population mouse for arthritic fingers purchase medrol 4mg free shipping. Disseminated coccidioidomycosis is associated with a very high mortality rate, and should be treated with amphotericin (17). Folic acid antagonists and sulpha drugs carry some risks for the fetus, but the alternative, pentamidine, is associated with higher risks for both mother and fetus. Active tuberculosis is treated with isoniazid and rifampin, which have a low risk of adverse fetal effects. Ethambutol is also used initially until sensitivities are available, and pyrazinamide is recommended by some authorities. Asthma Asthma is the commonest chronic medical illness to complicate pregnancy, affecting up to 7% of women of childbearing age. Pregnancy provides an opportunity to diagnose asthma, and to optimize the treatment of women already known to have asthma. Reversible bronchoconstriction is caused by smooth-muscle spasm in the airway walls and inflammation with swelling and excessive production of mucus. The clinical features include cough, breathlessness, wheezy breathing, and chest tightness. Symptoms demonstrate diurnal variation and are commonly worse at night and in the early morning. There may be clear provoking trigger factors, such as pollen, animal dander, dust, exercise, cold, emotion, and upper respiratory tract infections. Signs are often absent but during an acute attack there may be increased respiratory rate, inability to complete sentences, wheeze, use of accessory muscles, and tachycardia. Diagnosis is based on the recognition of a characteristic pattern of symptoms and signs in the absence of an alternative explanation. Women with only mild disease are unlikely to experience problems, whereas those with severe asthma are at greater risk of deterioration, particularly late in pregnancy. Women whose symptoms improve during the last trimester of pregnancy may experience postnatal deterioration. Acute asthma in labour is unlikely because of increased endogenous steroids at this time. Deterioration in disease control is commonly caused by reduction or even complete cessation of medication due to fears about its safety. For the majority of women, asthma has no adverse effect on pregnancy outcome, and women should be reassured accordingly. Severe, poorly controlled asthma, associated with chronic or intermittent maternal hypoxaemia, may adversely affect the fetus. Retrospective, uncontrolled or small studies have demonstrated associations between maternal asthma and pregnancy-induced hypertension/ pre-eclampsia, preterm births and preterm labour, low-birthweight infants, fetal growth restriction, and neonatal morbidity, including transient tachypnoea of the newborn, neonatal hypoglycaemia, neonatal seizures, and admission to the neonatal intensive care unit (18). In general, adverse effects on pregnancy outcome are small and related to the severity and control of the asthma. Most of the abovementioned associations are uncommon in clinical practice and women should be reassured that those with well-controlled asthma mostly have normal pregnancies with healthy babies. Poorly controlled severe asthma presents more of a risk to the pregnancy than the medication used to prevent or treat it. Women should be advised that their asthma is unlikely to adversely affect their pregnancy and maintaining good control of asthma throughout pregnancy is important. Emphasis in the management of asthma is on the prevention, rather than the treatment, of acute attacks. Management follows a stepwise approach and readers are directed to the British Thoracic Society/Scottish Intercollegiate Guidelines Network guideline on the management of asthma (19). Alternatively the dose of inhaled steroid can be increased to 2000 mcg/day (step 4). If these measures fail to achieve adequate control then continuous or frequent use of oral steroids becomes necessary. The lowest dose providing adequate control should be used, if necessary with steroid-sparing agents (step 5). The aim of treatment is to achieve virtual total freedom from symptoms, such that the lifestyle of the individual is not affected. This is inappropriate and pregnancy provides an ideal opportunity to educate women with asthma. Women should be advised to stop smoking and encouraged to avoid known trigger factors. They should receive explanation and reassurance regarding the importance and safety of regular medication in pregnancy (19). Home peak-flow monitoring and written personalized self-management plans should be encouraged. Use of a large-volume spacer may improve drug delivery and is recommended with high doses of inhaled steroid. The treatment of asthma in pregnancy is essentially no different from the treatment of asthma in non-pregnant women. The challenge in the management of pregnant women with asthma is to ensure adequate preconception or early pregnancy counselling so that women do not stop important anti-inflammatory inhaled therapy. Education and reassurance, ideally prior to pregnancy, concerning the safety of asthma medications during pregnancy are integral parts of management. Safety profile of medications used to treat asthma 2-agonists from the systemic circulation cross the placenta rapidly, but very little of a given inhaled dose reaches the lungs, and only a minute fraction of this reaches the systemic circulation. Studies show no difference in perinatal mortality, congenital malformations, birthweight, Apgar scores, or delivery complications when pregnant women with asthma treated with inhaled 2-agonists are compared with women with asthma not using 2-agonists and non-asthmatic controls. Long-acting -agonists should only be used concurrently with long-acting inhaled corticosteroids. They should not be discontinued or withheld in those who require them for good asthma control. Only minimal amounts of inhaled corticosteroid preparations are systemically absorbed. There is no evidence for an increased incidence of congenital malformations or adverse fetal effects attributable to the use of inhaled beclomethasone (Becotide) or budesonide (Pulmicort). Fluticasone propionate (Flixotide) is a longer-acting inhaled corticosteroid that may be used for those requiring high doses of inhaled steroids. The addition of systemic corticosteroids to control exacerbations of asthma is safe, and these must not be withheld if current medications are inadequate. Prednisolone is metabolized by the placenta, and very little (10%) active drug reaches the fetus. There is no evidence of an increased risk of miscarriage, stillbirth, other congenital malformations, or neonatal death attributable to maternal steroid therapy. There is a non-significant increase in the relative risk of preeclampsia in women with asthma treated with oral but not inhaled steroids. However, it is unclear whether this is an effect of steroids or asthma control and severity. Long-term, high-dose steroids may increase the risk of preterm rupture of the membranes. There are concerns regarding the potential adverse effects of steroid exposure in utero (such as from repeated high-dose intramuscular betamethasone or dexamethasone to induce fetal lung maturation) and neurodevelopmental problems in the child. It is unlikely that lower doses of prednisolone that do not cross the placenta as well as betamethasone or dexamethasone will have similar adverse effects. Oral steroids will increase the risk of infection, gestational diabetes, and cause deterioration in blood-glucose control in women with established diabetes in pregnancy. Blood glucose should be checked regularly; the hyperglycaemia is amenable to treatment with diet, metformin, and, if required, insulin, and is reversible on cessation or reduction of the steroid dose. The development of hyperglycaemia is not an indication to discontinue or decrease the dose of oral steroids, the requirement for which must be determined by the asthma. Oral steroids for medical disorders in the mother should not be withheld because of pregnancy. It is important to treat any gastroesophageal reflux as this can exacerbate asthma. No adverse fetal effects have been reported with the use of inhaled chromoglycates.
Buy medrol line
Episiotomy should be performed at the time of perineal distension by the fetal buttocks (27) arthritis neck pillow uk buy discount medrol 16mg. Delivery of the fetal legs and trunk the mother should be encouraged to push to deliver the buttocks and the legs spontaneously. The operator should avoid unnecessary intervention, but may help to flex the knee joint by slightly pressing at the popliteal fossa, and then delivering the flexed thigh by splinting the medial side of the thigh and sweeping it laterally. The operator may also guide the rotation of the buttocks to a sacral anterior position after both legs have been delivered. This may indicate that in women carrying breech presenting pregnancies, their fetuses may have less reserve to sustain stress during labour, or the maternal pelvic size may be less optimal for normal childbirth. By doing so, leverage is exerted upon the posterior shoulder, which may slide out over the vulval margin. The operator may then follow the posterior humerus to its elbow and sweep the arm out. Delivery of the fetal head the appearance of the fetal hairline outside the vulva indicates that the fetal head is now ready for delivery. Unlike vaginal cephalic delivery in which the fetal cranium has undergone moulding throughout labour as a gradual process, the vaginal delivery of the aftercoming head is potentially more difficult as the base of the skull (not moulded) would come out prior to the cranium. Hence, reducing the presenting diameter of the head by keeping it in a flexed position during the decent of the fetal head is crucial for a smooth delivery. Care should be taken to avoid blindly pressing the left fingers on the fetal eyeballs (just above the maxillas), or inserting the fingers into the fetal mouth and to pull the lower jaw. Suprapubic pressure by an assistant may help to facilitate the fetal head flexion. The fetal body is then elevated towards the maternal abdomen, so that the fetal head gradually rotates out of the perineum starting from the fetal mouth, nose, brow, and eventually the occiput. Forceps to aftercoming head Grasping the fetal head with a pair of forceps properly can ensure the head flexion during the descent process. After successful locking of the forceps, the fetal head is pulled out by the blades while the shanks and handles are swung upwards to deliver the fetal head in the flexed position. Once the buttocks are delivered, the mother is encouraged to push to deliver the fetal abdomen and the trunk gradually, with or without conjunctional use of gentle downward and rotational force of the operator. The operator should hold the fetal bony pelvis steadily, instead of holding its abdomen, which may result in rupture of the internal organs. Pulling on the legs to promote descent should also be avoided as it may cause hip dislocation or other fetal injury. The umbilical cord may be exposed from the vagina during this stage, and precautions must be taken to avoid any cord compression. Delivery of the fetal arms When the scapulas are visible outside the vulva, the next step is to deliver the arms, which are often extended, and the forearms may be even positioned behind the fetal neck (nuchal arm). Continuous downward traction would not help to deliver the arms but further extend it. Successful rotation would lead to the sliding of the anterior shoulder and humerus to the vulval level. Similar manipulation can be applied on the contralateral side to deliver the other shoulder and arm. If very rarely the rotation cannot facilitate the delivery of the anterior arm, the posterior arm can be approached and delivered first. Risks and complications of assisted vaginal breech delivery One of the major risks of vaginal breech delivery is fetal hypoxic injury, as the umbilical cord is vulnerable to compression or vasoconstriction once it is outside the cervix during the delivery process. Delayed delivery caused by nuchal arm or head entrapment increases the risk of hypoxia. Birth trauma such as fractures, nerve injury, and visceral injury can be caused by forceful traction or poor manipulation by inexperienced hands. A recent meta-analysis shows that although planned vaginal delivery is associated with a two to five times higher perinatal complication rate than planned caesarean delivery, its absolute mortality (0. Hence careful clinical assessment of patients, appropriate medical indication of the procedures, and proper training of the skills required are all essential to ensure safe application of these procedures. Planned vaginal birth or elective repeat caesarean: patient preference restricted cohort with nested randomised trial. Prevalence of levator ani muscle injury and health-related quality of life in primiparous Chinese women after instrumental delivery. Third- and fourth-degree perineal tears among primiparous women in England between 2000 and 2012: time trends and risk factors. The effect of a mediolateral episiotomy during operative vaginal delivery on the risk of developing obstetrical anal sphincter injuries. Anal sphincter damage after vaginal delivery: functional outcome and risk factors for fecal incontinence. Episiotomy characteristics and risks for obstetric anal sphincter injuries: a case-control study. Internal anal sphincter defect influences continence outcome following obstetric anal sphincter injury. Push, pull, squeeze, clamp: 100 years of changes in the management of the third stage of labour as described by ten teachers. The force applied to successfully turn a foetus during reattempts of external cephalic version is substantially reduced when performed under spinal analgesia. Randomized trial of anaesthetic interventions in external cephalic version for breech presentation. Outcome of labour after successful external cephalic version at term complicated by isolated transient fetal bradycardia. External cephalic version does not increase the risk of intrauterine death: a 17year experience and literature review. Intrapartum cesarean delivery after successful external cephalic version: a meta-analysis. Planned caesarean section versus planned vaginal birth for breech presentation at term: a randomized multicentre trial. While the term fetal death is most accurate, the word stillbirth is preferred by parents and the community (1, 2). For international comparisons, the World Health Organization recommends reporting of late gestation stillbirths (>28 weeks). The stillbirth rate is commonly expressed as the number of stillbirths per 1000 births. Different practices for inclusion of medical terminations of pregnancy also result in variations in reported stillbirth rates (3). Risk factors Two recently reported systematic reviews on risk factors for stillbirth (5, 7) are summarized here with the major factors presented in Table 34. These risk factors also make an important contribution to stillbirth globally (5). Women of 35 years or older have a 70% increased risk in stillbirth accounting for around 7% of stillbirths globally (7). Maternal overweight and obesity has become a global health problem, which also carries an increased risk of stillbirth (20% and 60% respectively). The contribution to stillbirth of maternal overweight and obesity globally is estimated at 10% (5) and may be twice that in some disadvantaged groups with higher rates of overweight and obesity (7). Maternal obesity also increases the risk of diabetes and hypertension, which further places women at increased risk of stillbirth. Despite modern obstetric care, pre-existing diabetes is associated with a threefold increase in stillbirth (7). The risk of stillbirth for women having their first child is around 40% higher than women who have had a previous birth. National, regional, and worldwide estimates of stillbirth rates in 2015, with trends from 2000: a systematic analysis. Facility and home stillbirth rates are differential, the direction of increased stillbirth rates is unpredictable because the values might be lower at home if high-risk cases are in facilities, or higher at home if very low access to care. Combining risk factors is also important and the stillbirth risk in older primiparous women.
Generic 4mg medrol with mastercard
If misdiagnosed or untreated arthritis joint pain relief order 4 mg medrol with amex, postpartum psychosis is one of the major risk factors for suicide after childbirth and in tragic but rare circumstances may also be linked with infanticide (Box 18. In a retrospective study on 116 women with postpartum psychosis, only 58% of women had a further pregnancy (61). Recurrence rates are around 50% for further postpartum episodes and between 50% and 70% for bipolar recurrences outside the puerperium (76, 77). Postpartum psychosis has a negative impact on the life of the woman, with one study reporting 18% of marriages ending after the severe postpartum episode (61). Bipolar disorder As we have discussed, over 50% of episodes of postpartum psychosis are the first episode of illness, but there is strong evidence of a specific relationship to bipolar disorder. Even if the woman is not planning a pregnancy, the prescription of psychotropic drugs should take account of the up-to-date data on teratogenic risk. Women planning a pregnancy or those in the perinatal period should be sensitively provided with relevant, understandable information on treatment and prevention options. An integrated health plan should be developed in collaboration with the woman and, if she agrees, her partner, family, or caregiver and a healthcare professional should be responsible for coordinating it. Regular monitoring of the symptoms is important and increasing contacts with the health services may be necessary. For severe psychiatric disorder, referral to a secondary mental health service should be considered. Similar to postpartum psychosis, there is a lack of randomized controlled trials on the treatment of postpartum bipolar depression. A naturalistic study on 34 women with postpartum bipolar depression initially misdiagnosed as unipolar showed that the discontinuation of antidepressants and the introduction of a mood-stabilizing therapy improved symptoms in 88% of cases (19). Psychological interventions and psychoeducation should always be considered, even if specific evidence for these approaches in the perinatal period is lacking (64). Schizophrenia Schizophrenia is a chronic, highly disabling, and severe mental disorder that affects about 1% of the general population. Symptoms usually start in early adulthood and are commonly grouped in three categories: positive (hallucinations, delusions, thought and movement disorders), negative (blunted expression of emotions, anhedonia, difficulty beginning and sustaining activities, reduced speaking), and cognitive (poor executive functioning and working memory, trouble focusing or paying attention). Although women with schizophrenia may have lower fertility, with the development of newer antipsychotic medications that impact less on prolactin levels, more women with this disorder are becoming mothers (64). The close relationship of episodes of illness following childbirth observed in bipolar disorder is not found for schizophrenia, a marked distinction between the two disorders (11, 44). There is a paucity of evidence on the management of schizophrenia in the perinatal period. Although women with schizophrenia may successfully parent, many do have difficulties. Indeed, studies have shown that the diagnosis of schizophrenia, together with that of personality disorders and substance abuse or dependence, are associated with an increased risk of involvement of social services (64). The loss of custody of a child represents a severe threat and a traumatic event (71) that can precipitate a crisis and a worsening clinical picture. According to the Eighth Report of the Confidential Enquiries into Maternal Deaths in the United Kingdom, 31% of mothers who committed suicide during pregnancy had been referred to social services (83). Although schizophrenia is associated with problems with the maternal role and a 25-fold increased risk of social service supervision compared to psychotic depression, women with schizophrenia are not necessarily unable to fulfil the maternal role (64). Among the factors that should be considered in assessing the potential for successful parenting are (valid also for other psychiatric disorder) (a) psychotic symptoms involving the baby or passivity experiences; (b) the Clinical presentation and epidemiology Over 70% of mothers with bipolar disorder have suffered at least one episode of mood disorder in the perinatal period, and over one in four have experienced an episode of postpartum psychosis (12). Although the emphasis for women with bipolar disorder has always been on psychotic/manic episodes, a large retrospective study on 1212 women with bipolar disorder found that non-psychotic depression is the most common mood episode in the perinatal period (12). It does appear, however, that there is a closer relationship between childbirth and episodes of mania and psychosis. Over 90% of manic/psychotic episodes occur within the first 4 weeks after childbirth, while one depressive episode in four has its onset later in the postpartum period, after the first month (12). The association between childbearing and bipolar disorder is specific for delivery and for manic/psychotic episodes. The risk of manic/psychotic episodes is significantly lower after miscarriage or termination than after delivery whereas depressive episodes are equally common following each of these pregnancy outcomes (60). The high risk of recurrence after delivery does not seem merely related to the discontinuation of medications during pregnancy, as recurrences are three times more frequent postpartum when lithium (a first-line treatment for bipolar disorder) is discontinued due to pregnancy than when the woman stops taking it for other reasons (70% vs 24%) (78). Treatment the pharmacological treatment of bipolar disorder during pregnancy often requires difficult decisions and needs to be evaluated in light of the high risk of recurrence and the negative impact that the illness may have on the fetus (4, 48, 64). The discontinuation of lithium during pregnancy, especially if abrupt, doubles the risk of a recurrence (79). There is a paucity of evidence on the impact of personality disorders in the perinatal period. According to a Scandinavian survey, the prevalence of personality disorders in pregnancy, assessed by self-report, is about 6% (85). Personality disorders often occur in comorbidity with other disorders and are associated with poor prognosis (8, 85). Significant constipation is a common side effect of all opioids, including replacement therapy, and should be enquired about and addressed by clinicians (89). Depression during pregnancy is associated with an increased risk of premature delivery, while evidence for birth weight is equivocal (90). Maternal perinatal depression has been associated with emotional dysregulation, impaired social skills, internalizing and externalizing disorders, attachment problems, and increased risk of depression during adolescence (90). It has been hypothesized that the mechanisms underpinning the association between depression in the offspring and maternal antenatal and postnatal depression are different (91). There is little or inconsistent evidence for an effect of perinatal depression on cognitive development (90). There is a paucity of studies investigating the effects of other mental disorders and evidence is often inconsistent. A study conducted on multiparae admitted to mother and baby units found that the risk of psychiatric disorders in adulthood was higher in offspring of puerperal episodes (34%) compared to their siblings from unaffected pregnancies (15%) (92). The study of the effect of alcohol and illicit substances during pregnancy on the fetus is complicated by the use of multiple substances, comorbidity with other psychiatric disorders, and the association with disadvantaged socioeconomic status. Teratogenic effects include intrauterine death, dysmorphism, growth restrictions, and behavioural changes (93). A Norwegian survey reported remission rates between 29% and 78%, depending on the specific eating disorder (88). Over half of women with a history of a prepregnancy eating disorder have a continuation or recurrence in the postpartum (8). The continued presence of eating disorder symptoms increases the risk of postpartum depression compared to women whose symptoms remit (8). Apart from binge-eating disorder, the incidence of other eating disorders in pregnancy is rare (8). Substance abuse and dependence the United States 2012 National Survey on Drug Use and Health estimated that 9. These estimates are roughly half the rates observed in nonpregnant women in the same age group (89). There are significant barriers to care for pregnant women with substance use disorders (89). Universal antenatal screening with validated questionnaires has been advocated and should be preferred to urine drug testing, that does not identify women with significant, but sporadic, use and may prevent women to seek prenatal care (89). Perinatal women with substance use disorders require intensive and multidisciplinary care. They often present comorbidity with other medical and psychiatric disorders and environmental stressors that need to be addressed. A harm reduction approach, aimed to extend periods of abstinence while recognizing the likelihood of relapse, should be adopted (89). Opioidcontaining pain medications are ten times more commonly used than heroin during pregnancy (89). Opioid replacement therapy has Conclusion Obstetricians will frequently be involved in the care of women with the new onset or recurrence of a psychiatric illness. There are significant barriers to care for women with psychiatric disorders in the perinatal period. Universal screening for the most prevalent disorders, depression and anxiety, but also for eating disorders and substance abuse has been advocated but remains controversial.
Buy medrol 4 mg low price
Women with chronic hypertension are at increased risk for adverse obstetrical outcomes including preterm birth arthritis upper spine cheap 4mg medrol with amex, intrauterine growth restriction, placental abruption, fetal death, and developing pre-eclampsia (30). In the preconception period, optimization of antihypertensive medication and cardiovascular health are the main goals. For women with long-standing chronic hypertension, preconceptional evaluation should include assessment of cardiac and renal involvement, including baseline heart and kidney function tests. Depending on the chronicity and severity of the disease, baseline investigations may include an electrocardiogram, echocardiogram, serum creatinine, glomerular filtration rate, blood Preconceptional evaluation of women with heart disease Women of reproductive age with existing heart disease require evaluation in the preconception period, with unique implications for treatment options. There are specific cases in which caesarean section is recommended, including severe pulmonary stenosis and ventricular function deterioration, and discussion of this should be considered in the preconceptional period (36). Preconceptional evaluation includes a baseline cardiovascular stress test and screening tests with electrocardiography and echocardiography in order to detect these modifiable risk factors. In cases where valvular surgery is indicated, preconceptional counselling is paramount regarding the timing of the surgery, as well as the resulting implications of treatment following the interventions of bioprosthetic versus mechanical valve replacement. In cases where valve replacement is indicated, there is no clear consensus on the recommendations, as the individual case should be discussed and managed by a cardiologist with specialties in management of pregnancy in conjunction with an obstetrician. Studies have shown increased risk of low birth weight, preterm delivery, and risk of antepartum haemorrhage (41, 42). The preconception period for women of reproductive age is paramount to optimize disease management, including discussion of nutritional requirements such as increased folic acid requirements of 1. A recent study showed that women who conceive in remission have a decreased risk of having active disease during pregnancy (46). Despite the improved outcomes from quiescent disease in preconception, unfortunately approximately one-third of women still relapse in pregnancy, with most relapses occurring in the first trimester. Optimization of therapy preconceptionally is also important to preserve fertility. This effect is related to both medication use as well as surgical intervention, and is a potentially reversible cause of infertility that should be addressed with couples in the preconception period (58, 59). Particular consideration should be taken regarding the management of epilepsy in relation to pregnancy, the effect of pregnancy on seizure frequency, the potential effects of epilepsy treatment on the fetus, the increased risks of obstetrical complications, and the preparation for the postpartum period. It is important to discuss some of the increased risk for obstetrical complications that women with epilepsy have. Historically, it was theorized that women with epilepsy are at increased risk of developing pre-eclampsia and eclampsia in pregnancy. However, recent studies have not shown evidence of an increased risk for development of pre-eclampsia, although these were insufficiently sensitive to rule out the increased risk (65). There is evidence to show that women with epilepsy have an increased risk of preterm labour, however recent studies demonstrate that smoking may be a confounder, as the risk is substantially higher in those women with epilepsy who also smoke (65). This is particularly important in discussions of preconceptional health, as the disease has an increased prevalence in women of childbearing age (68, 69). In the preconception period, it is advised that women discontinue disease-modifying agents, as some of these are known to be teratogenic (methotrexate, teriflunomide). Current evidence suggests that women discontinue disease-modifying agents in the preconception period from 1 to 6 months prior to conception, depending on the drug, and this decision should be discussed with a neurologist (73). Similarly, women are cautioned against using disease-modifying agents in the postpartum period if breastfeeding, and this schedule should be discussed with a neurologist. Preconceptional management strategies in women with thrombophilic disorders the discussion of thrombophilic disorders in preconceptional management is important, as it is one of the leading causes of maternal morbidity and mortality, despite being a rare complication in pregnancy with a prevalence of only 0. Although screening should be completed in the preconception period, there is no indication for thromboprophylaxis in the preconception period, unless the condition itself requires this treatment. The recommended thromboprophylaxis in the antepartum period may include daily low-molecular-weight heparin administration, with the risks and benefits of treatment discussed on an individual basis with each woman. Specific considerations that should be assessed at the initial preconception visit include general diet and weight, possible issues of smoking and/or substance use, obesity/diabetes, hypertension, possible cultural context, vaccination status, possible hepatitis C coinfection, and signs of immunosuppression including fevers and history of opportunistic infections. Careful physical examination should also include signs of immunosuppression, including signs of thrush, cachexia, genital ulcers, or vaginal discharge. Optimization of maternal health in the preconception period is paramount to a healthy pregnancy, and should include folic acid supplementation of 1 mg per day for at least 3 months preconceptionally, treatment of any active infections, evaluation of maternal psychosocial health, and counselling regarding smoking cessation, alcohol and drug use, and safe sex practices. Mode of delivery can be affected by viral load, and therefore should be discussed during the preconception period (82, 83). Previous fetal loss and future management considerations the rate of fetal loss in the United Kingdom historically is approximately 1 in every 200 deliveries, which is a devastating experience for mothers and families (87). There is controversial evidence regarding the relative risk of recurrence of stillbirth in lowrisk women with previous unexplained fetal loss, with some studies showing no increased risk, and others finding a 3. Identifiable causes of fetal loss can be broken down into categories of obstetrical complications, fetal complications, maternal complications, and unknown causes. Many of these are either difficult to diagnose in early pregnancy, or non-modifiable, making counselling around these obstetrical complications difficult for future expectations. Fetal complications mainly include karyotype abnormalities, with the most common being trisomy 18 and 21 (98). One of the fetal complications that poses a modifiable intervention to reduce the risk of congenital malformations leading to fetal loss includes ensuring adequate counselling regarding maternal folic acid fortification (99). Maternal causes include primarily pre-existing maternal disease, maternal trauma, and infection with syphilis, malaria, cytomegalovirus, and Coxsackie B virus as potential infections that contribute to fetal loss (93, 100). Counselling in this area should include discussion around vaccinations, including influenza vaccine, and to counsel women regarding foods to avoid including soft cheeses, and as well as some meats and seafood products (100). Maternal diabetes and hypertensive disorders are the two most common maternal complications that have identifiable and preventable risk factors (95). Counselling for couples with genetic abnormalities and inheritable conditions Detection of genetic abnormalities in the antenatal period can significantly affect the outcome of a pregnancy. Congenital abnormalities as a cause of death in the perinatal period have decreased dramatically from 1960 to 2013 (101, 102). This can be attributed, in part, to the higher rates of detection in the prenatal period, with medical advances in treatment options as well as subsequent selective termination. New advances in genetic screening tests have made preconceptional carrier testing possible through genetic testing across single genes and more recently multiple genetic mutations with genome sequencing. Typically, carrier testing is performed on the maternal genes, followed by paternal testing if any genes of interest are identified. This can be offered to couples at high risk for specific inheritance, or for those who wish to pursue this testing through the private sector. Although this is not the standard method of screening for chromosomal abnormalities, noninvasive testing is being used more commonly as a screening tool to diagnose several genetic conditions due to the high sensitivity and specificity that it offers. During a preconceptional evaluation of couples with genetic abnormalities, specific factors should be discussed in detail, including personal and family history of known or suspected inheritable diseases, consanguinity, advanced maternal and paternal age, potential teratogen exposure, ethnic background with an increased prevalence of disease, and recurrent pregnancy loss. If any of these factors are of concern, genetic counselling referral with a geneticist is indicated and should be done preconceptionally if possible. A detailed family history, including first-, second-, and third-degree relatives, is important to identify any unexplained perinatal or infant deaths, intellectual disability, or congenital abnormalities that could otherwise be missed. When an inheritable disease is identified, a couple should be informed regarding the likelihood of future offspring developing the condition, which may depend on the pattern of inheritance, including Mendelian versus di- or multigenic, as well as penetrance and variable expression. The burden of disease on both the inheriting individual as well as the family should be discussed, including the potential for requirement for chronic hospitalization or shortening of life span; cost of treatments; impact on future reproductive potential; and effects on physical and mental development, with special consideration of future ability to engage in activities of daily living independently. Alternative options to modify the impact of disease for couples with known inheritable disease include artificial insemination by donor, ovum transfer from surrogate, as well as adoption. Drugs to avoid preconceptionally Women of reproductive age can be taking medications for chronic diseases, may start new medications during pregnancy, or require over-the-counter medications during the preconception period or during pregnancy. We will discuss medications taken commonly during pregnancy separately from those taken for chronic illness. For these chronic illnesses, most prescription drug regimens should be optimized in the preconception period, and medication changes avoided during pregnancy, unless indicated.
Medrol 4 mg with visa
Mechanical ventilatory support should target tidal volumes of 6 mL/kg (predicted body weight) and plateau pressures less than 30 cmH2O arthritis medication celebrex buy 16mg medrol mastercard. The reduced chest wall compliance in pregnancy may require slightly higher airway pressures than in the non-pregnant patient. Non-conventional modes of ventilation have been used successfully in pregnancy as a rescue intervention, including extracorporeal membrane oxygenation (30). Delivery is sometimes, but not always, beneficial to the mother and should be considered on an individualized basis by the multidisciplinary team (31). Amniotic fluid embolism Although small amounts of amniotic fluid are likely to enter the circulation during uncomplicated pregnancy, occasionally the catastrophic syndrome of amniotic fluid embolism results. The onset is usually during labour and delivery or following uterine manipulation. Initial manifestations may be acute severe dyspnoea and hypoxaemia, following which seizures, cardiovascular collapse, or cardiac arrest may occur. The mechanism involves traumatic opening of uterine vessels, with constituents of the amniotic fluid producing the pathological effects. These constituents may include leukotrienes, arachidonic acid metabolites, and fetal squamous cells. The haemodynamic effects include acute pulmonary hypertension followed by left ventricular dysfunction (33). The diagnosis is usually by exclusion-several biomarkers have been evaluated, with poor sensitivity and specificity. Low levels of C1 esterase inhibitor may be a useful marker and may play a pathological role (34). Gastric acid aspiration Contributing factors for gastric acid aspiration include the effect of progesterone lowering the tone of the oesophageal sphincter, the increased intra-abdominal pressure due to the enlarged uterus, and use of the supine position for delivery. The majority of cases of aspiration occur in the delivery suite, and all pregnant women should be considered to have a full stomach. The clinical presentation is of a sudden onset of dyspnoea occurring during or within 6 hours of transfusion of plasma-containing blood products. The differential diagnosis includes circulatory overload, which should respond to diuresis. This is likely due to the fact that pyelonephritis is the most common cause of severe sepsis during pregnancy. Polycythaemia gives an indirect assessment of the degree of hypoxia and in itself is associated with an increased risk of thrombosis due to hyperviscosity. Women are often delivered preterm due to deterioration in respiratory function in the third trimester, and by caesarean section because of associated abnormalities of the bony pelvis and of abnormal presentations of the fetus. Women with nocturnal hypoxia/hypercapnia may require supplemental oxygen and non-invasive ventilation. Regional analgesia/anaesthesia where the block is high may be dangerous in a woman with limited respiratory reserve. In addition, some women have had Harrington rods inserted that may preclude regional anaesthesia. Elective caesarean section may occasionally be indicated for anaesthetic reasons in women in whom regional techniques are not possible and emergency general anaesthesia is deemed too risky because of airway concerns. Restrictive lung disease Restrictive lung disease appears reasonably well tolerated in pregnancy as the lungs have relatively more reserve than the heart (38). Whatever the underlying Interstitial lung disease Reduced diffusing capacity may cause difficulty in meeting the increased oxygen consumption requirements of pregnancy. Management of the acute presentation is usually with high-dose intravenous pulsed methyl prednisolone and management of the chronic disease is immunosuppression with steroids, azathioprine, cyclophosphamide, methotrexate, or biologicals such as rituximab. Immunosuppression, usually with prednisolone or azathioprine, should be continued in pregnancy. Mycophenolate mofetil, methotrexate, and rituximab are usually avoided in pregnancy but cyclophosphamide can be used in the second and third trimester for severe disease (41). Pneumothorax Most cases of pneumothorax in pregnancy occur in those with underlying lung pathology such as emphysema, Marfan syndrome, or bronchiectasis. Pneumothorax may rarely occur during the second stage of labour secondary to rupture of a bulla during prolonged Valsalva manoeuvres. Chest drains can be inserted in pregnancy and for resistant cases video-assisted thoracoscopic surgery and pleurodesis should not be withheld. Note bilateral airspace disease, bilateral chest tubes for barotrauma, elevated diaphragms, and lead shielding of abdomen. Treatment is usually supportive with oxygen, management of airflow obstruction, and treatment of pneumothorax if it occurs. Recently, genetic findings have suggested a benefit of mechanistic target of rapamycin inhibitors such as sirolimus. Sleep-disordered breathing Sleep-disordered breathing includes the spectrum of snoring, upper airway resistance syndrome, and obstructive sleep apnoea and hypopnoea syndrome. Maternal obesity together with the physiological changes of pregnancy discussed previously predispose to the development of sleep disordered breathing (42). Since nasal obstruction is a risk factor for snoring and sleep-disordered breathing in the general population, it is possible that the nasal hyperaemia and rhinitis of pregnancy increase the risk in pregnancy. Upper airway size at the oropharyngeal junction is also reduced in pregnancy and especially in pre-eclampsia. However, because women in the second half of pregnancy sleep in the lateral position and spend less time in rapid eye movement sleep they are less prone to apnoeic and hypopnoeic events. The risk is also lower because of the respiratory stimulatory effect of progesterone (43). Continuous positive airway pressure is the treatment of choice of sleep-disordered breathing in the general population and can be safely and effectively used in pregnancy. Continuous positive airway pressure has been associated with lower nocturnal blood pressure measurements in patients with preeclampsia (44). This is an autosomal dominant vascular dysplasia characterized by epistaxis, mucocutaneous telangiectasias, and arteriovenous malformations in the brain, lung, liver, gastrointestinal tract, or spine. The risks included bleeding leading to potentially catastrophic haemoptysis, infectious and ischaemic neurological manifestations due to paradoxical emboli, and high-output cardiac failure due to systemic arteriovenous shunting. Women should therefore deliver in facilities with interventional radiology support. Respiratory functions, buffer system, and electrolyte concentrations of blood during human pregnancy. Lymphangioleiomyomatosis Lymphangioleiomyomatosis is a rare lung disease most commonly affecting women of childbearing age, which occurs sporadically or associated with tuberous sclerosis complex. Pathological findings are interstitial proliferation of abnormal smooth muscle, which obstructs lymphatics and causes multiple thin-walled pulmonary cysts. Patients with lymphangioleiomyomatosis present with progressive dyspnoea, recurrent pneumothoraces, chylous collections, or haemoptysis. Elevated serum vascular endothelial growth factor-D levels have been demonstrated in this condition. Lymphangioleiomyomatosis is thought to be accelerated by oestrogen and is believed to progress during pregnancy. Critical illness due to 2009 A/ H1N1 influenza in pregnant and postpartum women: population based cohort study. Hospital readmission after delivery: evidence for an increased incidence of nonurogenital infection in the immediate postpartum period. Systematic review of the safety of regular preventive asthma medications during pregnancy. Acute respiratory distress syndrome in pregnancy and the puerperium: causes, courses, and outcomes. Amniotic fluid embolism incidence, risk factors and outcomes: a review and recommendations. Interventions at caesarean section for reducing the risk of aspiration pneumonitis.
Horse Gowan (Ox-Eye Daisy). Medrol.
- What is Ox-eye Daisy?
- Dosing considerations for Ox-eye Daisy.
- How does Ox-eye Daisy work?
- Are there safety concerns?
- Common cold, cough, bronchitis, fever, mouth and vocal cord swelling (inflammation), liver and gallbladder problems, loss of appetite, reducing spasms, increasing the amount of urine produced (diuretic), skin swelling (inflammation), wounds, and burns.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96106
Discount medrol 4mg on line
When given antenatally arthritis of fingers purchase medrol uk, particularly in the third trimester, it has been associated with premature closure of the patent ductus arteriosus. Anaesthesia provides total relief of pain, which is necessary for a surgical operation (2). Non-pharmacological methods Many factors can help reduce the need for pharmacological intervention. There is little research proving the effectiveness of these treatments though lots of women say that they found these techniques useful. A calm environment and the presence of a trusted companion throughout labour may reduce the need for pain relief. Adverse effects: toxicity is common and increases with duration of therapy; 20% of long-term users will experience side effects. It is inhaled using a mouthpiece during labour and provides rapid-onset pain relief of short duration during contractions. Its use in between contractions should be discouraged to prevent unwanted side effects. Adverse effects: in some patients, nitrous oxide can cause extreme dizziness accompanied by nausea and vomiting. Heavy use of nitrous oxide may cause signs of hypocapnia and hyperventilation including paraesthesia and muscle cramps. Midazolam is a water-soluble benzodiazepine with anxiolytic, amnestic, and hypnotic properties. When used in combination with opioids, it has a marked synergistic effect that increases the likelihood of life-threatening complications, such as hypoxaemia and apnoea. It is better to supplement inadequate pain relief with other anaesthetic techniques including conversion to a general anaesthetic as appropriate. Adverse effects: pethidine has significant anticholinergic effects including dry mouth and mydriasis. It can precipitate seizures in patients with a history of epileptogenic seizures and in those taking monoamine oxidase inhibitors. Codeine is often given as a combination with paracetamol in a preparation called co-codamol. Dihydrocodeine is structurally similar to codeine but is twice as potent and it can also be combined with paracetamol as co-dydramol. Subsequently, a significant reduction in its use in the peripartum period has been observed. Signs of opioid toxicity in mothers and neonates may include a reduced conscious level and respiratory depression. Remifentanil is an effective alternative to epidural analgesia in labour where epidural analgesia may be contraindicated. Mechanism of action: remifentanil is a potent opioid, which acts at the mu-receptor and is over a hundred times as potent as morphine. Most opioids are metabolized in the liver, but remifentanil is rapidly metabolized by esterase enzymes in the plasma and tissues resulting in a very short duration of action. This property is unique among opioids and prevents the accumulation of remifentanil over time, allowing it to be used for long periods during labour. Adverse effects: like all potent opioids, remifentanil can cause significant respiratory depression and a reduced conscious level. Remifentanil can also cause hypotension and bradycardia which can be treated with antimuscarinics such as atropine or glycopyrrolate. Remifentanil does cross the placenta, but is most probably rapidly metabolized by the fetus with minimal effect of the neonate. It crosses the placenta and can cause significant neonatal depression, with peak effect at 4 hours after maternal dose. It crosses the placenta and is contraindicated during labour (*of a live fetus) due to the risk of neonatal respiratory depression. It can be safely administered for pain relief in labour if the mother is not carrying a live fetus. Adverse effects: morphine causes a decrease in conscious levels and can cause respiratory depression. Indications Epidural analgesia is indicated primarily for pain relief in labour (7). It also has the advantage of providing pain relief for episiotomy and perineal suturing. Epidural anaesthesia can be used as an adjunct in the management of severe pre-eclampsia due to the vasoactive hypotensive effect of the sympathetic blockade resulting from epidural local anaesthetic administration. Epidural anaesthesia can also be performed de novo for operative intervention where spinal block may not be appropriate. Anaesthesia to the T4 dermatome level bilaterally is necessary to minimize the chances of the parturient experiencing pain during a caesarean section. Regional anaesthesia is, on the other hand, used to facilitate operative interventions in theatre. The clinical situation and the urgency of the situation often dictate which method of regional analgesia or anaesthesia is used. Effective epidural/spinal block can allow caesarean section, or the trial of operative vaginal birth in theatre with immediate conversion to a caesarean section if necessary (6). It lies anterior to the ligamentum flavum and posterior to the posterior longitudinal ligament. The innervation for the uterus is derived from T10 to L1 nerve Technique A soft plastic catheter is introduced into the epidural space using a specially designed needle called a Tuohy needle. Traditionally, the L3/4 interspace is chosen because the spinal cord ends at L1/2. The catheter is introduced through the Tuohy needle, which is then removed, leaving the catheter in place (8). Between 3 and 5 cm of catheter is left in the epidural space, through which a local anaesthetic solution can be administered. A low-dose concentration of local anaesthetic is delivered in combination with an opioid which improves the quality and duration of analgesia. The anaesthetic solution can be administered as intermittent boluses, continuous infusion, or patient-controlled boluses (patientcontrolled epidural analgesia). These drugs can cause significant neurological and cardiovascular compromise including cardiac arrest if administered in excessive doses or accidentally injected into blood vessels. Local anaesthetics exert their action by reversibly blocking the transmission of action potential in sensory, motor, and sympathetic nerve fibres. Local anaesthetic molecules inhibit the passage of sodium through voltage-sensitive ion channels in the neuronal membrane. In excessive doses, the molecules can bind to ion channels in other excitable tissues resulting in cardiovascular arrhythmias and cardiac arrest. Neurological side effects include an altered mental state, perioral tingling, and seizures. Neurological adverse effects tend to develop before cardiovascular complications become evident. Local anaesthetic toxicity is a medical emergency and should be treated according to nationally agreed protocols using advanced life support algorithms and intravenous lipid solution (9). The third national audit project of the Royal College of Anaesthetists reported an incidence of permanent harm of 0. This is usually the consequence of an inadvertent puncture of the dura with the Tuohy needle. The resultant headache is typically occipitofrontal, and may also involve neck pain. Many cases will respond to conservative management such as simple analgesics, adequate hydration, and increased caffeine intake. In cases where a severe headache persists, an autologous epidural blood patch may be required. Spinal anaesthesia Spinal block is typically used to facilitate operative interventions.
Order medrol in india
The minimum acceptable rate of progress for the active phase of the first stage of labour was defined by Friedman as 1 cm/hour in nulliparous women and 1 arthritis spine diet medrol 16mg free shipping. This standard has more recently been challenged with the suggestion that normal labour progresses somewhat slower. An abnormal first stage of labour can essentially be classified into the following three categories: 1. A prolonged latent phase-because the duration of the latent phase Abnormal labour It is essential that before labour can be defined as abnormal, the nature of normal labour is fully understood and accepted. Much of what defines an abnormal labour is derived from studying spontaneous labours that result in vaginal birth. Failure to achieve the time limits and milestones of these labours is what separates normal from abnormal. The definition also implies that abnormal labours are associated with a higher risk of maternal and fetal/neonatal adverse outcomes or an inability to achieve a spontaneous vaginal birth. Defining the abnormal first stage of labour Defining an abnormal latent phase of labour is problematic. It is known that the latent phase encompasses the progressive effacement and dilatation of the cervix. The latent phase ends with a fully effaced cervix, the dilatation at which this occurs being less important and also a matter of some controversy. Women presenting in spontaneous labour are more commonly already in the active phase of labour. This makes any attempt to define the normal duration of the latent phase purely speculative. Women who are in the delivery suite and diagnosed as being in the latent phase are likely to either have been misdiagnosed to be in labour or requiring induction of labour. Friedman defined the latent phase of labour as being prolonged if it lasted more than 20 hours in the nulliparous woman or 14 hours in the multiparous woman (16). These limits may reflect what was viewed as an acceptable length of time to subject a woman to the stresses of labour. Prolonged labours can also be emotionally traumatic for women and increase demands on staff and resources. It is for these reasons that in present-day obstetrics, labours are not usually allowed to continue for as long as initially suggested by Friedman. Primary dysfunctional labour-progress which is slower than the accepted rate of progress but which continues until full dilatation is achieved. Secondary arrest-a halt in progress in the active phase of labour prior to full cervical dilatation. Management of the prolonged first stage of labour the prolonged latent phase Women may be diagnosed to be in the latent phase of labour because they present with a show or prodromal or Braxton-Hicks contractions. Vaginal examination findings of a cervix that is not fully effaced would support this diagnosis. In the absence of a medical indication to expedite delivery, these women are best managed expectantly. If left alone, these women often return to the delivery suite in the active phase of labour at a later time. If an amniotomy is performed inadvertently or intentionally in these women, delivery becomes mandated. The next intervention is an oxytocin infusion to optimize uterine contractions in the hope that labour will progress beyond the latent phase and into the active phase of the first stage. If labour does not progress within the time limits which are acceptable, intervention by caesarean section becomes necessary. Reference was made earlier in this chapter to the 20-hour limit for nulliparous women and 14 hours for multiparous women proposed by Friedman and the fact that shorter durations would be the norm in modern obstetrics. The treatment for primary dysfunctional labour is to ensure efficient uterine contractions. This is achieved by performing an amniotomy, if the membranes are intact, or commencing an oxytocin infusion. The aim is to achieve five uterine contractions every 10 minutes but not more frequent than this. More than five contractions in 10 minutes is termed tachysystole and may induce fetal intolerance as manifested by abnormal fetal heart rate patterns. If this does not happen, there is still a place for expectant management as long as progressive cervical dilatation occurs. Fetal malposition the fetus in the occiput anterior presentation adopts a well-flexed attitude. This results in a vertex presentation where the presenting diameter, the suboccipitobregmatic diameter, is the smallest possible anteroposterior fetal cephalic diameter to negotiate the maternal pelvis. As a result, occipitoanterior positions are optimal for spontaneous vaginal birth unless an unusually large baby or unusually small maternal pelvis is present. The same is not true in malpositions such as an occipitoposterior or occipitotransverse position. In these situations, although there is no cephalopelvic disproportion in the absolute sense, the wider and therefore less optimal fetal diameters must negotiate the maternal pelvis. Often, optimizing uterine contractions may correct the malposition and allow the labour to progress. If this spontaneous flexion and rotation to an occiput anterior position does not occur, with persistent malposition and failure to progress with increasing moulding and caput, recourse to caesarean section may need to be considered. Secondary arrest Causes of an arrest in progress of cervical dilatation in the active phase can be classified as the three Ps. Passages-an adequately large pelvic cavity as a conduit for Defining the abnormal second stage of labour Reference is made in the previous section to the fact that there is no clear consensus on the acceptable duration of the second stage of labour. Traditionally, in the presence of regional anaesthesia, the cut offs are 3 hours and 2 hours in nulliparous women and multiparous women respectively. Confirming that efficient uterine activity is present is the first step in managing secondary arrest. An amniotomy (if membranes are intact) or an oxytocin infusion are the available interventions to correct inadequate uterine contractions. There is a case to consider an oxytocin infusion even in women who demonstrate regular uterine contractions as the strength of the contractions is not possible to assess clinically. This is particularly so in nulliparous women who more frequently require augmentation with oxytocin. Augmentation is also safer in nulliparous women whose risk of uterine rupture from this intervention is so low that they are often termed to be immune to it (19). Cephalopelvic disproportion As the name suggests, this cause of secondary arrest is due to a mismatch in fetal size and diameters of the pelvis. Occasionally, women with an acquired cause of a contracted pelvis such as a history of traumatic fractures of the pelvis may be encountered. In addition to poor cervical dilatation there may be signs of increasing caput and moulding. It is also clear that the practice of delayed pushing, which refers to allowing a period of time after full cervical dilatation during which the woman is not actively encouraged to bear down, will have a bearing on the duration of the second stage. Delayed pushing is shown to increase the likelihood of a spontaneous vaginal delivery (21). Another consideration is that, although a longer second stage may not have harmful fetal or maternal effects, it may not always be possible in practice as maternal exhaustion may set in. Ensure uterine contractions are optimal and consider oxytocin augmentation if appropriate-this step is best considered before the agreed limits of the second stage are reached. If delayed pushing is practised, an opportune time to start oxytocin augmentation is when active bearing-down efforts by the mother commence. In the presence of malposition, rotational operative vaginal delivery or manual rotation to the occiput anterior position followed by operative vaginal delivery may be possible. Manual rotation to the occiput anterior position by an experienced clinician appears to be effective (22) and is a promising intervention, especially in light of the decreasing use of rotational forceps for these deliveries. In deciding between operative vaginal delivery and caesarean section, careful consideration of the clinical situation including abdominal and vaginal examination findings, the fetal heart rate pattern, and maternal cooperation is essential. The experience of the obstetrician is also a key factor in choosing the appropriate mode of delivery. Cervicographs in the management of labour in primigravidae-the alert line for detecting abnormal labour.
Effective medrol 4mg
A number of factors appear to promote the development of adenomyosis including multiparity arthritis in dogs feet discount 16 mg medrol amex, spontaneous miscarriage, surgical termination of pregnancy, curettage, hysteroscopic resection of the endometrium, myomectomy, caesarean section, imaging features Ultrasonography the presence of adenomyosis is suggested by the presence of three or more of the following signs: 1. The heterogeneous appearance is due to the presence of heterotopic endometrial tissue and myometrial cell hypertrophy (36). An enlarged uterus with smooth regular contours and asymmetrical hypertrophy of the uterine walls, the posterior wall usually thicker than the anterior wall. Doppler sonography may show linear striations crossing the myometrium within the adenomyotic lesions (36). The corpus uteri is flexed backwards, the fundus of the uterus faces the posterior compartment, and the cervix is directed frontally towards the bladder. Medical treatment Oral progestogens such as dydrogesterone can be used to treat premenopausal menometrorrhagia. It causes endometrial atrophy due to its antioestrogen effect and therefore relieves irregular bleeding, dysmenorrhoea, and pain. It might need to be replaced earlier than the 5-year recommended interval due to tachyphylaxis (46). They can also be used for symptom relief for women who do not desire fertility immediately, but who want conservative treatment. They are generally administered for up to 6 months and rarely for up to a year, with add-back oestrogen/gestagen therapy to prevent menopausal symptoms (44). They are also used preoperatively to reduce uterine size prior to hysterectomy or to make resection of adenomyotic lesions easier (44). Surgical treatment the age of the patient and whether preservation of fertility is required are the two factors that determine the type of surgery: radical or conservative. Radical Radical treatment involves hysterectomy, either total or subtotal, based principally on the condition of the cervix, pouch of Douglas, and rectovaginal septum (44). The decision to remove the adnexa will depend on the presence of endometrioma, deep peritoneal endometriosis, and the age of the patient. This appears as a hypoechoic halo around the endometrium, whose thickening and integrity can be assessed under 3D ultrasound. Multiple leiomyoma: localized forms of adenomyosis are more difficult to diagnose as these can mimic fibroids. Colour and power Doppler can help to distinguish these two entities: in adenomyosis the vessels spread through the myometrium, whereas in fibroids they surround the lesion without penetrating it (36). Cystic glandular hypertrophy, frequently caused by medications such as tamoxifen, are more difficult to differentiate from the subendometrial cysts seen in adenomyosis. It demonstrates continuity of the subendometrial cystic spaces with the endometrial cavity, with the superficial sites remaining in continuity and the deep sites losing continuity. Surgery often results in fibrotic scars and suture material in surrounding healthy tissue, which can affect future fertility adversely. Moreover, conservative surgery is only effective in up to 50% of patients and there are no data on long-term follow-up (48). More recently, endomyometrial ablation, laparoscopic myometrial electrocoagulation, and excision have been tried as an alternative treatment options for patients with localized adenomyosis. Transcervical endometrial ablation or resection is only possible for patients with submucous or superficial localized adenomyosis (48). However, symptoms may be persistent after use of this approach when the depth of the lesion is greater than 2. Although laparoscopic electrosurgical excision can significantly relieve pain, with low rates of complications, a second procedure is often required (49). Uterine artery embolization this involves selective embolization of the uterine artery on each side with microarticulate non-calibrated polyvinyl alcohol or calibrated trisacryl alcohol with or without gelatin sponge. On the basis of limited evidence, there seems to be short-term clinical resolution of symptoms particularly menorrhagia, but not pain (50). The fundamental difference to other ablation techniques using coagulation necrosis such as radiofrequency, laser microwave, and cryotherapy is that it does not require the use of applicators to deliver the energy. The advantages are an absence of bleeding or risk of seeding metastasis, and the ability to treat poorly perfused tumours, large volume, or irregular tumours. However, the high energy levels used may affect tissues in the path of the beam, potentially resulting in inadvertent ablation of the endometrium or the endometrial blood vessels. However, high-quality randomized trials are necessary before its introduction into clinical practice. Conclusion Adenomyosis is a common benign condition that can cause menorrhagia, dysmenorrhoea, and dyspareunia. With ultrasound it can be difficult to differentiate a leiomyoma from adenomyosis. Conservative therapies such as local resection and high-energy ablation are promising, but require further rigorous evaluation. Uterine fibroids introduction Fibroids are the most common tumour in women of reproductive age (54, 55). Recent years have seen a demographic shift in childbirth trends, with many women delaying starting their families until they reach their third or fourth decade (56, 57). The repertoire of uterus-preserving treatments for symptomatic fibroids has increased in recent years. Despite the emergence of these new treatments for managing symptomatic uterine fibroids, in reality, when the uterus is to be preserved, myomectomy, especially the open abdominal approach, remains the treatment of choice of many gynaecologists. Thus reports, based on clinical diagnosis or diagnostic tests, underestimate the true incidence of fibroids, but nevertheless it is estimated that the lifetime risk of having fibroids for a woman over the age of 45 years is greater than 60% (68). It is highly likely that the prevalence of fibroids is underestimated: the incidence of histological analysis is more than double the clinical incidence, and the incidence increases with increasing age (70). Aetiology Despite considerable research, the aetiology of uterine fibroids is unknown. What is well established is that all the cells within a given fibroid originate from a single cell (the monoclonal origin of fibroids) (71, 72)-but what actually causes the transformation from a normal myometrial to a leiomyoma cell remains enigmatic. While it is evident that ovarian steroid hormones promote fibroid growth, there is no evidence for differences in circulating concentrations of these hormones between women with and without fibroids. Cytogenetic chromosomal alterations, including translocations, duplications, and deletions have also been found in up to 50% of fibroid tumours. Clearly, fibroids are not a single-gene disorder, and this might in part explain the heterogeneity in the phenotype of fibroids between individuals and also between different ethnic groups. Epidemiology There is a clear-cut racial disparity in age of onset and number and size of fibroids between black, white, and Asian women (76, 77). The reasons for the racial differences are not known, and while epidemiological factors linked to fibroids are thought to include reproductive factors, sex steroids, and lifestyle/environmental factors in addition to racial origin, the available information should be interpreted with caution. For example, the racial disparity is not reflected in hormonal concentrations or oestrogen receptor expression. The familial predisposition to fibroids is illustrated by a number of observations: female relatives of women with fibroids have a significantly increased risk of developing fibroids; twin pair studies indicate an increased risk of fibroids in monozygotic compared to dizygotic twins (78, 79); and there is a consistent pattern of clinical symptoms, operative findings, and tissue molecular features in families with a prevalence of uterine fibroids compared with those without this prevalence (77). Fibroids are associated with the polycystic ovary syndrome, hypertension, and obesity, while smoking in white (but not black) women appears to be protective (80). There are no dietary factors that have been proven to alter the risk of developing fibroids. Fibroids are commoner in nulliparous women, with the relative risk decreasing with increasing number of term pregnancies. Fibroids initially increase in size in the first trimester of pregnancy and then shrink in size over the next two trimesters. There is therefore an overall relative decrease in uterine fibroid volume during the course of pregnancy (81, 82). The effect of the oral contraceptive pill on the risk of fibroids is unclear, with some studies showing an increased risk, others a decrease, and yet others no association at all. However, it is likely that there is altered smooth muscle cell proliferation in association with disordered angiogenesis (83).
