
Purchase discount ramipril on line
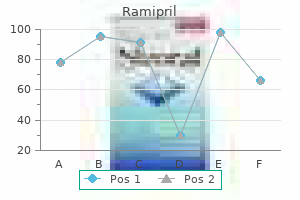
These illnesses have sometimes been referred to as typhoidal fevers blood pressure quit smoking cheap 5 mg ramipril amex, and are usually characterized as nonspecific systemic illnesses associated with fever that lasts longer than a week. Indeed, typhoid itself was named for its clinical similarity to typhus, caused by Rickettsia species. Typhus and typhoid are both characterized as febrile illnesses that may be prolonged and associated with encephalopathy or confusion, and if untreated, both diseases are associated with high mortality rates. In South and Southeast Asia, scrub typhus (Orientia tsutsugamushi) and murine typhus (Rickettsia typhi) are highly endemic, and are often mistaken for typhoid. Leptospirosis is also a common cause of nonspecific febrile illness in many typhoid-endemic areas, and is often underdiagnosed owing to lack or underuse of diagnostics. Similarly, individuals with brucellosis may present with nonspecific fever, malaise, and abdominal pain. Fever may be prolonged, and infection during brucellosis is often characterized by its chronicity. Manifestations include osteoarticular and genitourinary involvement, granulomatous hepatitis, uveitis, and, rarely, endocarditis. Most human infections are due to exposure to small rodents or lagomorphs (rabbits), and humans usually become infected through direct contact with infected animals or animal parts, or through the bite of an arthropod as a transmission vehicle. Persistent fever with nonspecific symptoms may also be seen with melioidosis, an infection caused by Burkholderia pseudomallei. Melioidosis may manifest in a number of ways, ranging from a chronic febrile illness to an acute septicemia,165 and it may include abscess formation (often in the spleen, liver, lungs, or muscles) or pneumonia. Melioidosis is associated with water and soil exposure and can affect anyone, although individuals with diabetes, immunosuppression, chronic renal disease, alcoholism, and cirrhosis are at particular risk. A typhoidal-like illness can also be seen with Q fever, caused by the intracellular bacterium Coxiella burnetii. Q fever is a zoonotic infection usually associated with exposure to sheep or cattle, and humans become infected through exposure to pseudospores from animal products, especially placental tissues. Individuals with Q fever may present with prolonged fever and a wide range of symptoms, including headache, pneumonia, hepatitis, and endocarditis. Rat-bite fever, caused by Streptobacillus moniliformis, may also cause a nonspecific febrile illness that may mimic enteric fever, especially when the route of infection is foodborne (Haverhill fever); arthritis and rash can occur. During the acute illness (Oroya fever), patients present with fever and hemolytic anemia. In survivors, disease can progress to verruga peruana, a chronic illness characterized by vascular, proliferative, nodular skin lesions. In addition, Bartonella quintana is the cause of trench fever, a relapsing febrile illness transmitted by body lice. Trench fever usually affects individuals who are displaced or severely impoverished; onset is usually acute with high fever, headache, and retro-orbital pain, bone pain of the shins, and myalgia. Louse-borne relapsing fever is a humanrestricted infection caused by Borrelia recurrentis and is associated with human body lice. Relapsing fevers are characterized by relapsing and recurrent episodes of fever associated with spirochetemia. Individuals with these infections may present with a prolonged febrile illness, headache, and abdominal pain. Additional Causes of Prolonged or Persistent Fever Most acute febrile illnesses resolve within 3 to 7 days. Individuals with typhoid or enteric fever may have fever that lasts for 1 to 4 weeks before resolution if left untreated. Clinicians assessing individuals with fever that lasts longer than 7 to 10 days need to consider a wide differential, both for infectious and noninfectious processes (see Chapter 56). Noninfectious causes that also need to be considered include lymphoma, malignancy, drug fever, Addison disease, and inflammatory conditions and connective tissue disorders. As described earlier, prolonged fever may also be associated with malaria, brucellosis, yersiniosis, tularemia, Q fever, melioidosis, endocarditis, tuberculosis, and endemic mycoses such as histoplasmosis. Recurrent or relapsing fever may be associated with trench fever and relapsing fever. Clinicians caring for individuals with prolonged fever in resource-limited or tropical areas or caring for individuals who have traveled to such regions need to consider these and other diagnoses. For instance, individuals with babesiosis, caused by an intraerythrocyte protozoal parasite transmitted by ticks, may also present with a nonspecific and prolonged febrile syndrome. Chronic and relapsing fever are also part of visceral leishmaniasis, a protozoal parasitic infection of the reticuloendothelial system. Individuals with visceral leishmaniasis often present with prolonged and ongoing fever, hepatosplenomegaly, pancytopenia, hypergammaglobulinemia, and absence of eosinophilia. Individuals with human African trypanosomiasis (sleeping sickness) can present with chronic and recurrent fever, weight loss, and lymphadenopathy before neurologic manifestations occur. Serologic tests and direct parasitic detection are usually used to confirm the diagnosis. Prolonged fever can also be associated with a number of viral syndromes, including Epstein-Barr virus (mononucleosis), characterized by prolonged fever, headache, weakness, and fatigue and may include pharyngitis, hepatosplenomegaly, and lymphadenopathy. Most individuals with typhoid or paratyphoid present with an acute febrile illness, and typhoid and paratyphoid fever are common causes of bacteremia in many resource-limited areas of the world. Most cases of typhoid fever reported in North America and Europe are related to international travel, predominantly to South Asia,16 and affected patients usually develop fever within 1 to 3 weeks of exposure or returning from travel. Because vaccines are 50% to 80% protective and do not protect against Salmonella Paratyphi A, previous immunization does not preclude the possibility of enteric fever, and previous immunization can lead to cross-reactive serologic assays. Diagnosis can be confirmed by identifying Salmonella Typhi or Salmonella Paratyphi in blood cultures, but this assay is only 30% to 70% sensitive. Leading other causes of acute febrile illness in individuals at risk of typhoid include urinary, reproductive tract, and respiratory or intestinal tract infections that can be evaluated with standard approaches. Of importance, the differential diagnosis also needs to include influenza, dengue, chikungunya, Zika, leptospirosis, rickettsiosis, bartonellosis, and malaria, among others. An incubation period of less than a week before onset of fever would be most consistent with a viral cause, such as influenza or dengue. International travelers are at particular risk of influenza, and the transmission season in the Southern Hemisphere is March through September, with year-round transmission as one approaches the equator. Most individuals with dengue will present within 3 to 7 days of returning from travel to Asia or the Caribbean. Thrombocytopenia and evidence of capillary fragility, such as a positive tourniquet test, would be supportive of consideration of dengue fever (see Chapter 153). Leptospirosis is caused by exposure to animal urine, and exposure usually occurs from contaminated freshwater sources. The febrile illness can be biphasic, with conjunctival suffusion, hematuria, proteinuria, renal dysfunction, and hepatitis suggestive of the diagnosis (see Chapter 239). Rapid microscopic examination of peripheral blood should assist with establishing whether a patient may have malaria or borreliosis (see Chapter 240). A careful examination of skin for evidence of eschars or spotted rashes can assist in establishing whether the patient may have a rickettsiosis (see Chapter 186). Microbiologic culturing of blood will assist in confirming infection with a number of bacterial pathogens, including Salmonella. Assessing an Individual With an Acute Febrile Illness in a Resource-Limited Area or After International Travel Chapter 100 Typhoid Fever, Paratyphoid Fever, and Typhoidal Fevers Individuals with mesenteric adenitis or ileocecitis often present with a history of fever and abdominal pain, often localizing to the right lower quadrant. The illness needs to be differentiated from appendicitis, intraabdominal abscess formation, and diverticulitis (Table 100. Ingestion of undercooked or uncooked pork and pork-related products, such as the small intestine of pigs (chitterlings), are particular risk factors. Noninfectious causes include Crohn disease and Fever and Mesenteric Adenitis or Ileocecitis 1378 ulcerative colitis. Infectious causes of ileocecitis include appendicitis, diverticular abscess formation, intestinal yersiniosis, tuberculosis, histoplasmosis, and amebiasis complicated by an inflammatory mass (an ameboma), intestinal schistosomiasis complicated by an inflammatory mass (a bilharzioma), an intestinal actinomycetoma that may include drainage fistula tracks, and intestinal angiostrongyliasis (see "Fever, Abdominal Pain, and Peripheral Eosinophilia"). The differential diagnosis for these individuals includes a number of entities (see Table 100. Fascioliasis caused by the liver fluke Fasciola hepatica may manifest as severe, right upper quadrant pain and high-level peripheral eosinophilia and fever. Individuals are often diagnosed incorrectly as having a pyogenic hepatic abscess and drug reaction. During the initial phase of infection, the flukes can migrate through hepatic parenchyma, causing severe right upper quadrant pain.
Diseases
- Willems De vries syndrome
- Cutis verticis gyrata
- Guillain Barr? syndrome
- Diarrhea chronic with villous atrophy
- Neurotoxicity syndromes
- Saethre Chotzen syndrome
- Benign paroxysmal positional vertigo
- Anomic aphasia
- Clubfoot
- Van Bogaert Hozay syndrome
Cheap ramipril 10 mg with amex
Superior vena cava obstruction secondary to mediastinal lymphadenopathy in a patient with cystic fibrosis arteria pudenda interna buy cheap ramipril 1.25 mg. Retroperitoneal iliac fossa abscess: a complication of suppurative iliac lymphadenitis. Clinical and pathologic diagnosis and different diagnosis of syphilis cervical lymphadenitis. Clinical features and complications of Coxiella burnetii infections from the French National Reference Center for Q fever. Mycotic cervical lymphadenitis following oral mucositis in children with leukemia. Candida albicans cervical lymphadenitis in patients who have acute myeloid leukemia. Cryptococcal lymphadenitis diagnosed by fine needle aspiration cytology: a review of 15 cases. A 38-year-old woman with necrotising cervical lymphadenitis due to Histoplasma capsulatum. Rothia aeria neck abscess in a patient with chronic granulomatous disease: case report and brief review of the literature. A novel bacterium associated with lymphadenitis in a patient with chronic granulomatous disease. Clinicopathological features of cryptococcal lymphadenitis and a review of literature. Mycobacterial cervicofacial lymphadenitis in human immunodeficiency virusinfected individuals after antiretroviral therapy initiation. Pathogenesis and prevention of immune reconstitution disease during antiretroviral therapy. Immune reconstitution and "unmasking" of tuberculosis during antiretroviral therapy. Cryptococcal lymphadenitis and immune reconstitution inflammatory syndrome: current considerations. Corynebacterium pseudotuberculosis necrotizing lymphadenitis in a twelve-year-old patient. Lymphadenitis due to nontuberculous mycobacteria in children: presentation and response to therapy. Non-tuberculous mycobacteria in children: muddying the waters of tuberculosis diagnosis. A case of obstructive jaundice caused by tuberculous lymphadenitis: a literature review. Surgical excision versus antibiotic treatment for nontuberculous mycobacterial cervicofacial lymphadenitis in children: a multicenter, randomized, controlled trial. Human lymphadenitis due to Corynebacterium pseudotuberculosis: report of ten cases from Australia and review. Cat-scratch disease during anti-tumor necrosis factor-alpha therapy: case report and review of the literature. Mediastinal lymphadenopathy without cervical lymphadenopathy in a case of Kikuchi-Fujimoto disease. Interferon-gamma release assays for the diagnosis of latent tuberculosis infection: an updated review. Diagnosis, treatment, and long-term management of Kawasaki disease: a statement for health professionals from the Committee on Rheumatic Fever, Endocarditis, and Kawasaki Disease, Council on Cardiovascular Disease in the Young, American Heart Association. Diagnosis, treatment, and long-term management of Kawasaki disease: a scientific statement for health professionals from the American Heart Association. Lymph-node-first presentation of Kawasaki disease compared with bacterial cervical adenitis and typical Kawasaki disease. An uncommon presentation of Kikuchi-Fujimoto disease: a case report with literature review. Kikuchi-Fujimoto disease: retrospective study of 91 cases and review of the literature. Clinical characteristics of severe histiocytic necrotizing lymphadenitis (Kikuchi-Fujimoto disease) in children. Diagnosing Kikuchi disease on fine needle aspiration biopsy: a retrospective study of 44 cases diagnosed by cytology and 8 by histopathology. Consensus recommendations for the diagnosis and clinical management of Rosai-Dorfman-Destombes disease. Benign non-infectious causes of lymphadenopathy: a review of cytomorphology and differential diagnosis. Isolated leishmanial lymphadenopathy-a rare type of leishmaniasis in India: a case report. Silicone lymphadenopathy in a long distance runner: complication of a Silastic prosthesis. Symptomatic primary infection due to human immunodeficiency virus type 1: review of 31 cases. Discovery of human immunodeficiency virus infection by immunohistochemistry on lymph node biopsies from patients with unexplained follicular hyperplasia. First-generation fluoroquinolone use and subsequent emergence of multiple drug-resistant bacteria in the intensive care unit. Bancroftian lymphangitis in north-eastern Brazil: a histopathological study of 17 cases. Granulomatous lymphangitis of the scrotum and penis: report of a case and review of the literature of genital swelling with sarcoidal granulomatous inflammation. Mycobacterium marinum: ubiquitous agent of waterborne granulomatous skin infections. Case of Mycobacterium marinum infection with unusual patterns of susceptibility to commonly used antibiotics. J Gastrointestinal Infections and Food Poisoning 96 Syndromes of Enteric Infection Regina C. Enteric pathogens are frequently transmitted through contaminated food or water, and some pathogens with low infectious doses may spread from person to person. These pathogens may cause outbreaks of local and international significance and are among the leading causes of childhood morbidity and mortality, particularly in populations with limited access to safe water or adequate sanitation. Travel and the globalization of the food supply are important factors in the global dissemination of enteric infections. In such cases a specific microbiologic diagnosis is not necessary unless the disease is more severe or is part of an outbreak. The emergence of multidrug-resistant enteric pathogens, such as nontyphoidal Salmonella, Shigella, and Vibrio cholerae, and the increasing frequency and severity of nosocomial Clostridioides difficile (formerly Clostridium difficile) infection underscore the need for optimal, cost-effective approaches to the diagnosis, management, and control of enteric infections. Diarrhea is commonly defined as three or more loose stools in a 24-hour period1; it is considered acute when the duration is 14 days or less and persistent when the duration is 14 days or longer. Causative organisms differ significantly between gastroenteritis that is community acquired and that which is nosocomial. A broader spectrum of organisms may cause enteric infection in the immunocompromised 1330 host, and clinical manifestations may be more severe and more prolonged in such individuals. The Global Burden of Disease Study found that diarrhea was the ninth leading cause of death globally in 2015 and was responsible for 8. Nevertheless, diarrheal disease continues to cause significant morbidity, with nearly 1. Undernutrition, particularly micronutrient deficiency, increases susceptibility to acute infectious diarrhea and predisposes to more prolonged episodes of diarrheal illness. Conversely, diarrheal disease may exacerbate nutritional deficiencies in several ways. Gut injury causes malabsorption, and anorexia and altered eating habits may also affect caloric intake. In parts of the world where body stores of vitamin A are low, children with acute or persistent diarrhea can quickly develop complications of vitamin A deficiency, including xerophthalmia. Repeated episodes of diarrheal illness are associated with deficits in the physical and cognitive development of children. A multivariate analysis of longitudinal data from five developing countries found that the odds of stunting at 2 years increased with each diarrheal episode and with each day of diarrhea. Norovirus, which is highly contagious and robust in surviving on surfaces, is the most common etiologic agent associated with outbreaks of acute gastroenteritis and the leading cause of medically attended acute gastroenteritis in the United States. Historically, rotavirus has been the most common cause of acute gastroenteritis among infants and young children; pediatric rotavirus vaccination was broadly recommended in the United States in 2006,12 and pediatric diarrheal hospitalizations and medical expenditures have declined sharply since then.
Ramipril 10 mg sale
Empiric outpatient therapy with trimethoprim-sulfamethoxazole arteria basilaris cheap 1.25mg ramipril amex, cephalexin, or clindamycin for cellulitis. Review of infectious diseases in refugees and asylum seekers-current status and going forward. Epidemic diphtheria in the newly independent states of the former Soviet Union: implications for diphtheria control in the United States. Streptococcal necrotizing fasciitis: comparison between histological and clinical features. Streptococcal toxic-shock syndrome: spectrum of disease, pathogenesis, and new concepts in treatment. Hemolytic streptococcus gangrene: an uncommon but frequently fatal infection in the antibiotic era. Bacterial synergism in disease processes with a confirmation of the synergistic bacterial etiology of a certain type of progressive gangrene of the abdominal wall. Gangrenous cutaneous mucormycosis in a child with a solid organ transplant: a case report and review of the literature. Mucormycosis caused by unusual mucormycetes, non-Rhizopus, -Mucor, and -Lichtheimia species. Influences of linezolid, penicillin, and clindamycin alone and in combination, on streptococcal pyrogenic exotoxin A release. Antibiotic susceptibility of Corynebacterium minutissimum isolated from lesions of Turkish patients with erythrasma. Interventions in the management of infection in the foot in diabetes: a systematic review. Overview of the etiology of wound infections with particular emphasis on community-acquired illnesses. Laceration injuries and infections among workers in the poultry processing and pork meatpacking industries. Skin, soft tissue and systemic bacterial infections following aquatic injuries and exposures. Sporotrichoid Skin Infection Caused by Nocardia brasiliensis in a Kidney Transplant Patient. Cutaneous invasive aspergillosis: retrospective multicenter study of the French invasive-aspergillosis registry and literature review. Severe dermatophytosis in solid organ transplant recipients: a French retrospective series and literature review. Analysis of patient claims data to determine the prevalence of hidradenitis suppurativa in the United States. A clinicalpathological review of hidradenitis suppurativa: using immunohistochemistry one disease becomes two. Hidradenitis suppurativa and diabetes mellitus: a systematic review and meta-analysis. Spondyloarthritis associated with acne conglobata, hidradenitis suppurativa and dissecting cellulitis of the scalp: a review with illustrative cases. The role of anaerobic bacteria in cutaneous and soft tissue abscesses and infected cysts. Subcutaneous nodule as a manifestation of Pseudomonas sepsis in an immunocompromised host. Ecthyma gangrenosum without bacteremia: report of six cases and review of the literature. The acute arthritis-dermatitis syndrome: the changing importance of Neisseria gonorrhoeae and Neisseria meningitidis. Multifocal cellulitis and monoarticular arthritis as manifestations of Helicobacter cinaedi bacteremia. Clinical features of Staphylococcus aureus endocarditis: a 10-year experience in Denmark. Cerebral, myocardial and cutaneous ischemic necrosis associated with calcific emboli from aortic and mitral valve calcification in a patient with end-stage renal disease. Fever, rash, and muscle tenderness: a distinctive clinical presentation of disseminated candidiasis. Fatal disseminated Scedosporium inflatum infection in a neutropenic immunocompromised patient. Multifocal soft tissue cryptococcosis in a renal transplant recipient: the importance of suspecting atypical pathogens in the immunocompromised host. Clostridium septicum bacteremia and diffuse spreading cellulitis of the head and neck in a leukemic patient. Chapter 93 Cellulitis, Necrotizing Fasciitis, and Subcutaneous Tissue Infections 200. Monomicrobial Klebsiella pneumoniae necrotizing fasciitis: an emerging life-threatening entity. High mortality of non-Fournier necrotizing fasciitis with Enterobacteriales: time to rethink classification Assessing the relationship between the use of nonsteroidal anti-inflammatory drugs and necrotizing fasciitis caused by group A streptococcus. The roles of injury and nonsteroidal anti-inflammatory drugs in the development and outcomes of severe group A streptococcal soft tissue infections. Group A streptococcal necrotizing fasciitis following varicella in children: case reports and review. Getting under the skin: the immunopathogenesis of Streptococcus pyogenes deep tissue infections. Determination of the relationship between group A streptococcal genome content, M type, and toxic shock syndrome by a mixed genome microarray. Necrotizing fasciitis due to Serratia marcescens: case report and review of the literature. Clinical features of neutrophilic dermatosis variants resembling necrotizing fasciitis. Outcomes from treatment of necrotizing soft-tissue infections: results from the National Surgical Quality Improvement Program database. Soft-tissue infections and their imaging mimics: from cellulitis to necrotizing fasciitis. Early recognition of potentially fatal necrotizing fasciitis: use of frozen-section biopsy. Intravenous immunoglobulin in necrotizing fasciitis: a case report and review of recent literature. Management of soft-tissue infections of the upper extremity in parenteral drug abusers. Factitious fever and self-induced infection: a report of 32 cases and review of the literature. A Comprehensive Approach to the Management of Children and Adults with Chronic Granulomatous Disease. Rare presentation of Streptococcus pneumoniae pneumonia with bacteremia and multiple subcutaneous abscesses. Direct inoculation of muscle as the result of penetrating trauma is also an important mechanism of infection (associated with clostridial myonecrosis). More generalized muscle inflammation may also accompany a variety of acute and chronic viral and parasitic disorders. Epidemiology Clostridium perfringens myonecrosis complicates penetrating trauma, but nontraumatic clostridial myonecrosis may develop after hematogenous dissemination of more aerotolerant species. Group A streptococci can also cause severe myonecrotic infection, which is a true medical emergency. Acute generalized muscle inflammation occurs after influenza and dengue virus infections, but a wide variety of viral pathogens have sporadically led to significant muscle injury and even severe rhabdomyolysis.
Buy ramipril discount
The presentation in patients with septic lateral sinus thrombosis is typically more gradual blood pressure chart age 1.25 mg ramipril fast delivery, and patients complain predominantly of headache (>80% of cases); photophobia, earache, vomiting, and vertigo may also occur because otitis media is a common predisposing condition. Posterior auricular swelling and pain (Griesinger sign) are present in almost 50% of cases; a common complication is otitic hydrocephalus. In one study of 13 patients, the majority exhibited cranial neuropathies and raised intracranial pressure. Thrombosis of the superior sagittal sinus produces an abnormal mental status, motor deficits, nuchal rigidity, and papilledema. The majority of cases occur in the setting of bacterial meningitis, in which the onset may be fulminant. Patients with sinusitis as a predisposing condition tend to have a subacute onset of symptoms. Laboratory studies are usually nonspecific in suppurative intracranial thrombophlebitis. Blood cultures may be positive, especially in patients with a rapidly progressive course. Chest radiographs may reveal evidence of septic pulmonary emboli after propagation of the thrombus into the inferior petrosal sinus and jugular vein. Magnetic resonance venography is extremely useful in showing detailed venous anatomy and demonstrating an area of decreased or absent signal in the area of the thrombus. Selection of appropriate antimicrobial therapy for suppurative intracranial thrombophlebitis depends on the antecedent clinical condition; the likely microorganisms are similar to those observed in cranial subdural empyema and cranial epidural abscess (see earlier discussions). If the antecedent clinical condition is paranasal sinusitis, empirical antimicrobial therapy should be directed toward staphylococci, streptococci, aerobic gram-negative bacilli, and anaerobes. In septic cavernous sinus thrombosis, an antistaphylococcal agent should always be included because of the high likelihood of isolation of S. Vancomycin is recommended empirically, pending results of in vitro susceptibility testing. An appropriate empirical regimen is vancomycin, metronidazole, and a third- or fourth-generation cephalosporin, pending culture results and in vitro susceptibility testing. Intravenous antimicrobial therapy is usually continued for at least 3 to 4 weeks, but the duration needs to be individualized depending on the clinical response. The role of corticosteroids is not well established in the management of septic cerebral venous thrombosis; although they may help in decreasing inflammation and swelling, this use is not well supported by evidence. In fact, some authors have recommended operative intervention for all patients who develop cavernous sinus thrombosis as a complication of sinusitis. Arrow points to contrast-enhanced cavernous sinus with a dark circle of a flowing carotid artery (flow void signal). The dark white area below is the inflamed sphenoid sinusitis, which caused the cavernous sinus thrombosis. There is increased signal with the vessel on the T2-weighted image (arrowheads), indicating the presence of thrombus. Some authors have recommended ligation of the internal jugular vein for patients who develop septic embolization despite antimicrobial therapy and surgical drainage. However, it must be recognized that anticoagulation carries the risk of intracranial hemorrhage from sites of cortical venous infarction or from sites on the intracavernous walls of the carotid artery. Some authors have not recommended anticoagulation in patients with septic lateral sinus or superior sagittal sinus thrombosis because of the high number of venous hemorrhagic infarcts observed postmortem110; most of these infections can also be controlled with antimicrobial therapy and surgery, and the use of anticoagulation has not been shown to be beneficial. Some practitioners use anticoagulation in cavernous sinus thrombosis only as an adjunct to antimicrobial therapy in patients with a deteriorating clinical condition. Before the availability of antimicrobial therapy, suppurative intracranial thrombophlebitis carried a mortality rate of 80% to 100%. Since 1940, mortality rates have ranged from 0% to 16% in patients with septic lateral sinus thrombosis116 and from 13% to 30% in patients with septic cavernous sinus thrombosis,110,113 although in one series of 14 pediatric patients with septic cavernous sinus thrombosis, 79% died despite parenteral antimicrobial therapy. Patients should be observed for several months after completion of antimicrobial therapy because isolated relapses have been documented within 6 weeks after apparent clinical resolution, and intracranial abscesses have been demonstrated as long as 8 months later. Intracranial subdural empyemas in the era of computed tomography: a review of 699 cases. Craniotomy improves outcomes for cranial subdural empyemas: computed tomography-era experience with 699 patients. Spinal epidural abscesses in children: a 15-year experience and review of the literature. Is there a difference in neurologic outcome in medical versus early operative management of cervical epidural abscess Management of spontaneous spinal epidural abscess: a single-center 10-year experience. Contemporary management of pediatric lateral sinus thrombosis: a twenty year review. Systematic review and case report: intracranial complications of pediatric sinusitis. Subdural empyema caused by Escherichia coli: hematogenous dissemination to a preexisting chronic subdural hematoma. Intracranial suppuration: a modern decade of postoperative subdural empyema and epidural abscess. Risk factor of complications requiring neurosurgical intervention in infants with bacterial meningitis. Role of anaerobic bacteria in subdural empyema: report of four cases and review of 327 cases from the English literature. Intracranial Salmonella infections: meningitis, subdural collections and brain abscess: a series of six surgically managed cases with follow-up results. Propionibacterium as a cause of postneurosurgical infection in patients with dural allografts: report of three cases. Focal intracranial infections due to Propionibacterium acnes: report of three cases. Subdural empyema caused by Neisseria meningitidis: a case report and review of the literature. Pediatric intracranial subdural empyema caused by Mycobacterium tuberculosis-a case report and review of the literature. Primary Candida albicans empyema associated with epidural hematomas in craniocervical junction. Subdural empyema of the cervical spine: clinicopathologic correlates and magnetic resonance imaging. Focal intradural brain infections in children: an analysis of management and outcome. Halo pin intra-cranial penetration and epidural abscess in a patient with a previous cranioplasty: case report and review of the literature. Spinal epidural abscess: contemporary trends in etiology, evaluation, and management. Spinal epidural abscess: experience with 46 patients and evaluation of prognostic factors. Spinal epidural abscess: clinical manifestations, prognostic factors, and outcomes. Spinal epidural abscess: aetiology, predisponent factors and clinical outcomes in a 4-year prospective study. Comparison of primary and secondary spinal epidural abscesses: a retrospective analysis of 29 cases. Spinal epidural abscess in adults caused by Staphylococcus aureus: clinical characteristics and prognostic factors. Clinical characteristics and therapeutic outcome of gram-negative bacterial spinal epidural abscess in adults. Thoracic vertebral actinomycosis: Actinomyces israelii and Fusobacterium nucleatum. Successful treatment of Aspergillus flavus spondylodiscitis with epidural abscess in a patient with chronic granulomatous disease. Chapter 91 Subdural Empyema, Epidural Abscess, and Suppurative Intracranial Thrombophlebitis 1271. Treatment strategies and outcome in patients with non-tuberculous spinal epidural abscess-a review of 46 cases.
RGAE (Rehmannia). Ramipril.
- Diabetes, anemia, fever, osteoporosis, allergies, or other conditions.
- How does Rehmannia work?
- What is Rehmannia?
- Dosing considerations for Rehmannia.
- Are there safety concerns?
- Are there any interactions with medications?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=97099
Cheap 5mg ramipril
Efforts should be made to reduce the degree of host immunosuppression whenever possible arrhythmia that makes you cough buy ramipril 2.5mg. Prognosis for survivors is excellent; 90% return to normal function, and the remaining 10% have only mild residual deficits. It is transmitted through various routes, including body fluids such as saliva and genital secretions, blood transfusions, and organ transplants. Patients may develop a nonspecific febrile encephalopathy with or without focal signs. Case studies have suggested that therapy with ganciclovir or foscarnet can be successful in bone marrow transplant recipients. Humans develop disease after a monkey bite or scratch or mucosal contact with infected body fluid. Vesicles develop at the site of exposure, followed by onset of a flulike syndrome characterized by fever, chills, myalgias, and headache. Diagnosis is made through wound or contact site culture and demonstration of an antibody response with acute and convalescent sera. For example, the upper Midwest and Northeast of the United States have seen a significant increase in Powassan virus infections. The most common vectors that transmit encephalitic viruses in the United States are mosquito species142 and tick species. Viruses included in this group belong to four families: Togaviridae, Flaviviridae, Bunyaviridae, and Reoviridae; each specific arbovirus within a family is commonly transmitted by a specific species of mosquito or tick. When the virus has penetrated the blood-brain barrier, arboviruses can directly infect and cause death of neurons. Approximately 20% of infected individuals develop an acute febrile flulike illness (West Nile fever) characterized by fever, headache, fatigue, anorexia, nausea, myalgia, and lymphadenopathy. Cranial neuropathies, most commonly involving unilateral or bilateral peripheral facial palsy, occur in approximately 20%. Cerebellar abnormalities including incoordination and gait ataxia occur in a variable percentage of cases. Patients typically develop acute onset of asymmetrical limb paralysis associated with decreased or absent reflexes and preserved sensation. Weakness may be associated with respiratory impairment from diaphragm or intercostal muscle paralysis. Electrophysiology studies obtained acutely show reduction in amplitude or absence of compound muscle action potentials with relatively preserved sensory nerve action potentials. Electromyographic studies obtained 2 to 3 weeks after onset show characteristic features of denervation, including increased insertional activity and fasciculations. Neutralization antibody titers are typically highest against the inciting virus compared with crossreacting species. Transmission to humans in the western United States is primarily via Culex tarsalis; in the eastern United States, it is through Culex pipiens, Culex quinquefasciatus, and Culex nigripalpus. The pathogenesis in adults is likely similar to that of other flaviviruses described earlier and results in asymptomatic infection in up to 80% of adults exposed to infection. Louis Encephalitis After the bite of an infected mosquito, an incubation period of 4 to 21 days precedes the onset of clinical symptoms. In patients younger than 20 years, 40% develop meningitis and 50% develop encephalitis. Louis encephalitis virus include reduced level of consciousness with lethargy, coma, tremors, myoclonic jerks, opsoclonus, nystagmus, and ataxia. Louis encephalitis virus infections ranges from 4% to 27%,175 seizures develop in 47% of patients, and acute flaccid paralysis has been associated with 6% of encephalitis cases. Severely affected patients may have seizures or periodic lateralizing epileptiform discharges. General laboratory studies reveal a peripheral leukocytosis, hyponatremia, mild transaminitis, and sterile pyuria. Eastern equine encephalitis virus is an alphavirus that causes a sporadic, mosquito-borne viral infection endemic in the eastern United States and the Caribbean. Eastern equine encephalitis virus is maintained in an enzootic cycle with avian species after a bite from a mosquito vector, Culiseta melanura. There have been 5590 reported symptomatic infections in the continental United States and Eastern Equine Encephalitis Virus 1243 Culex and Aedes spp. Approximately 1 in 30 individuals exposed to eastern equine encephalitis virus develops disease. Patients with eastern equine encephalitis virus develop nonspecific symptoms common to other causes of viral encephalitis, including fever, chills, malaise, and myalgias. There is no commercial vaccine for eastern equine encephalitis virus, but standard precautions to prevent mosquito bites may help to prevent infection. Overall mortality is approximately 30%, although higher mortality rates have been reported in older individuals. Forty percent of patients with Venezuelan equine encephalitis virus have virus in the pharynx, suggesting that direct spread between humans may be possible, although this has never been shown. Pharyngeal inflammation, painful cervical lymphadenopathy, somnolence, and tremulousness may occur. General laboratory abnormalities include leukopenia and elevated transaminase levels. Twenty-four cases of encephalitis were reported for a cumulative incidence rate of 8. Incidence rates were highest in patients younger than 1 year and in those older than 65 years. Of these viruses, La Crosse virus, California encephalitis virus, and Jamestown Canyon virus are causes of disease in the United States, and Tahyna virus is predominantly a cause of encephalitis in Russia. La Crosse virus is the most common cause of disease in the California encephalitis group. It was originally described in 1965 after a postmortem examination of a child who died of encephalitis in La Crosse, Wisconsin. It emerges during epizootic outbreaks to infect horses and humans via bridge vectors such as Aedes taeniorhynchus. Epidemics typically occur in northern South America but have extended as far north as Mexico and Texas. During an outbreak of Venezuelan equine encephalitis virus in Venezuela and Colombia in 1995, approximately 3000 cases of neurologic disease were reported, resulting in 300 deaths. Symptoms of encephalitis include fever, headache, vomiting in 70%, seizures in 46%, and altered mental status in 42%. No antiviral therapy currently exists for the California encephalitis group of viruses, and no vaccine is available. Mortality from La Crosse encephalitis is approximately 1% to 3%, and most survivors return to normal function. Similar to other flaviviruses, humans are incidental hosts that become infected when encountering the enzootic cycle. Personal protection with insect repellents, mosquito avoidance, and mosquito population control programs are important approaches. Less commonly, influenza has been associated with encephalitis in children and young adults. During the influenza A (H1N1) pandemic in 2009, influenza was associated with encephalitis and neurologic complications. Severe influenza in children and young adults with underlying neurologic or neurodevelopmental conditions has occurred in smaller outbreaks. Symptoms include fever; respiratory abnormalities (cough, coryza, wheezing, labored breathing); nausea; and diarrhea. Patients with severe influenza develop increased work of breathing, and neurologic involvement can be characterized by altered mental status, seizures, or focal neurologic signs. It is transmitted by the wood tick Dermacentor andersoni mainly in the western mountain regions of the United States and Canada above 4000 feet in elevation.
Order ramipril overnight
Staphylococcus bacteremia and endocarditis: new diagnostic and therapeutic concepts blood pressure fitbit generic ramipril 5mg fast delivery. Clindamycin therapy of Staphylococcus aureus endocarditis: clinical relapse and development of resistance to clindamycin, lincomycin, and erythromycin. Clinical significance of tolerant strains of Staphylococcus aureus in patients with endocarditis. Role of tolerance in cloxacillin treatment of experimental Staphylococcus aureus endocarditis. Addition of rifampin to standard therapy for treatment of native valve infective 678. The role of -lactamase in staphylococcal resistance to penicillinase-resistant penicillins and cephalosporins. Ciprofloxacin therapy of experimental endocarditis caused by methicillin-susceptible or methicillin-resistant Staphylococcus aureus. Efficacy of trovafloxacin, a new quinolone antibiotic, in experimental staphylococcal endocarditis due to oxacillin-resistant strains. Development of resistance to fleroxacin during therapy of experimental methicillin-susceptible Staphylococcus aureus endocarditis. Trimethoprimsulfamethoxazole compared with vancomycin for treatment of Staphylococcus aureus infection. Ceftaroline in combination with trimethoprim-sulfamethoxazole for salvage therapy of methicillin-resistant Staphylococcus aureus bacteremia and endocarditis. Salvage treatment of methicillin-resistant staphylococcal endocarditis with ceftaroline: a multicentre observational study. Staphylococcus aureus bacteremia: clinical, serologic, and echocardiographic findings in patients with and without endocarditis. Infective endocarditis due to Staphylococcus aureus: 59 prospectively identified cases with follow-up. Endocarditis due to glycopeptide-intermediate Staphylococcus aureus: case report and strain characterization. Staphylococcus epidermidis causing prosthetic valve endocarditis: microbiologic and clinical observations as guides to therapy. Value of antibiotic levels in serum and cardiac vegetations for predicting antibacterial effect of ceftriaxone in experimental Escherichia coli endocarditis. Impact of dosage schedule on the efficacy of gentamicin, tobramycin, or amikacin in an experimental model of Serratia marcescens endocarditis: in vitro-in vivo correlation. Identification of factors affecting in vivo aminoglycoside activity in an experimental model of gram-negative endocarditis. Endocarditis due to ampicillin-resistant nontyphoid Salmonella: cure with a third-generation cephalosporin. Vegetectomy: an alternative surgical treatment for infective endocarditis of the atrioventricular valves in drug addicts. Total tricuspid valvulectomy without replacement in the treatment of Pseudomonas endocarditis. Comparative pharmacokinetics and pharmacodynamics of amikacin and ceftazidime in tricuspid and aortic vegetations in experimental Pseudomonas endocarditis. Mechanisms of aminoglycoside resistance in variants of Pseudomonas aeruginosa isolated during treatment of experimental endocarditis in rabbits. Absence of a post-antibiotic effect in experimental Pseudomonas endocarditis treated with imipenem, with or without gentamicin. Effects of alginase on the natural history and antibiotic therapy of experimental endocarditis caused by mucoid Pseudomonas aeruginosa. Long-term oral ciprofloxacin: experience in the treatment of incurable infective endocarditis. Efficacy of ceftazidime and aztreonam alone or in combination with amikacin in experimental left-sided Pseudomonas aeruginosa endocarditis. Effect of penicillin resistance of Streptococcus pneumoniae on the presentation, prognosis, and treatment of pneumococcal endocarditis in adults. Fungal prosthetic valve endocarditis: an 11-year experience in a tertiary hospital. Combination antifungal chemotherapy for experimental disseminated candidiasis: lack of correlation between in vitro and in vivo observations with amphotericin B and rifampin. A comparison of the efficacy of itraconazole, amphotericin B and 5-fluorocytosine in the treatment of Aspergillus fumigatus endocarditis in the rabbit. Comparison of fluconazole and amphotericin B for prevention and treatment of experimental Candida endocarditis. Fluconazole treatment of catheter-related right-sided endocarditis caused by Candida albicans and associated with endophthalmitis and folliculitis. Long-term survival after fluconazole therapy of candidal prosthetic valve endocarditis. Treatment of Q fever endocarditis: comparison of 2 regimens containing doxycycline and ofloxacin or hydroxychloroquine. Endocarditis due to Q fever in Nova Scotia: experience with five patients in 1981-1982. Experience with trimethoprimsulfamethoxazole in treatment of infective endocarditis. In vitro activity of rifamycins alone and in combination with other antibiotics against Chlamydia trachomatis. Valve replacement in patients with native valve endocarditis: what really determines operative outcome Operative intervention in active endocarditis in children: report of a series of cases and review. Outcome in patients with left-sided native-valve infective endocarditis and isolated large vegetations. Prognostic significance of valvular regurgitation in patients with infective endocarditis. Clinical utility of cardiac valve Gram stain and culture in patients undergoing native valve replacement. Influence of the timing of cardiac surgery on the outcome of patients with infective endocarditis and stroke. Tricuspid valvulectomy without prosthetic replacement: ten years of clinical experience. Tricuspid valve endocarditis in the drug addict: a reconstructive approach ("vegetectomy. Endocarditis-associated paravalvular abscesses: do clinical parameters predict the presence of abscess Role of transthoracic echocardiography in predicting embolic events in patients with active endocarditis involving native cardiac valves. Long-term complications of native valve infective endocarditis in non-addicts: a 15-year follow-up study. Intravenous therapy in burn patients: suppurative thrombophlebitis and other life-threatening complications. Suppurative thrombophlebitis: correlation between pathogen and underlying disease. Venous thrombosis in patients with short- and long-term central venous catheter-associated Staphylococcus aureus bacteremia. Diagnosis of thrombosis by catheter phlebography after prolonged central venous catheterization. Association of hypercoagulable states and increased platelet adhesion and aggregation with bacterial colonization of intravenous catheters. Candida septic thrombosis of the great central veins associated with central catheters: clinical features and management. Serious complications of vascular catheter-related Staphylococcus aureus bacteremia in cancer patients. Septic atrial thrombosis: a potentially lethal complication of Broviac catheters in infants.
Buy generic ramipril canada
Pleural biopsy was established in the 1950s as a high-yield procedure blood pressure medication causes diabetes 10 mg ramipril otc, especially for the diagnosis of tuberculous pleurisy, because the additional histopathologic evidence and culture of tissue increase the sensitivity of microbiologic diagnosis substantially. Data on the specifics of antibiotic activity and pharmacokinetics in the pleural space are limited. Small-bore catheters have proven effective in tube thoracostomy, and flushing of catheters. The goal was to decrease the area of pleural opacity; 210 subjects were enrolled, and combination therapy was significantly effective compared to placebo. Significant secondary effects of reduced surgical referral and length of stay, but not reduced mortality, were found. In patients unable to tolerate this, medical thoracoscopy, although less studied as an intervention, seems to achieve acceptable rates of success with conscious sedation and without the use of an operating room. The choice of simple drainage (pigtail catheter or chest tube) was the strongest predictor of death or need for further procedure, but was still adequate/definitive treatment in 60 patients with stage I empyema, and the study did not attempt to address better staging. In addition to showing increased rates of disease during the period studied and significant imbalances related to younger age and lower comorbidity in patients undergoing surgery, adjustment for those factors still yielded a 58% lower risk of death in those undergoing operative therapy. There is no evidence to support antibiotic instillation into an infected space, although this was the basis of the Clagett procedure, in which a hole in the chest wall was created for periodic antibiotic instillation. Resection of the anterior ends of the lower ribs, called thoracoplasty, was designed to bring the chest wall toward the remaining lung. A persistent bronchopleural fistula was a relative contraindication for thoracoplasty and needed surgical repair. An even more intractable empyema can occur in a postpneumonectomy thoracic cavity. When empyema treatment fails and long-term chest tube drainage is used, an alternative is formation of an opening through the skin into the base of the thoracic cavity, allowing spontaneous drainage. Association of 2009 pandemic influenza A (H1N1) infection and increased hospitalization with parapneumonic empyema in children in Utah. Impact of human immunodeficiency virus infection on clinical and radiographic presentation. Pneumococcal empyema and complicated pneumonias: global trends in incidence, prevalence, and serotype epidemiology. The bacteriology of pleural infection by genetic and standard methods and its mortality significance. Report of a 63-case series of Candida empyema thoracis: 9-year experience of two medical centers in central Taiwan. Do pulmonary radiographic findings at presentation predict mortality in patients with community-acquired pneumonia Accuracy of pleural puncture sites: a prospective comparison of clinical examination with ultrasound. Pleural biopsy as an aid in the etiologic diagnosis of pleural effusion: review of the literature and report of 132 biopsies. Cholesterol: a useful parameter for distinguishing between pleural exudates and transudates. Volume and cellular content of normal pleural fluid in humans examined by pleural lavage. Management of pleural infection in adults: British Thoracic Society Pleural Disease Guideline 2010. The American Association for Thoracic Surgery consensus guidelines for the management of empyema. Medical and surgical treatment of parapneumonic effusions: an evidence-based guideline. Innate immune responses in murine pleural mesothelial cells: toll-like receptor-2 dependent induction of beta-defensin-2 by staphylococcal peptidoglycan. Vascular endothelial growth factor: the key mediator in pleural effusion formation. Mycobacteria induces pleural mesothelial permeability by down-regulating beta-catenin expression. Interleukin-1 receptor antagonist in pleural effusion due to inflammatory and malignant lung disease. Diagnostic value of interleukin-1alpha, interleukin-6, and tumor necrosis factor in pleural effusions. Immune response to Mycobacterium tuberculosis infection in the parietal pleura of patients with tuberculous pleurisy. Interleukin-8 is a major neutrophil chemotactic factor in pleural liquid of patients with empyema. Intrapleural injection of transforming growth factor-beta antibody inhibits pleural fibrosis in empyema. Nonmalignant pleural effusions: a prospective study of 356 consecutive unselected patients. Diagnosis and management of malignant pleural effusions: state of the art in 2017. The use of indwelling tunneled pleural catheters for recurrent pleural effusions in patients with hematologic malignancies: a multicenter study. Diagnosis and outcome of early pleural space infection following lung transplantation. Changing ecology of acute bacterial empyema: occurrence and mortality at Boston City Hospital during 12 selected years from 1935 to 1972. Duration of hospitalization for acute bacterial empyema at Boston City Hospital during 12 selected years from 1935 to 1972. An urgent problem of aerobic gram-negative pathogen infection in complicated parapneumonic effusions or empyemas. Frequency of tuberculinreactive T-lymphocytes in pleural fluid and blood from patients with tuberculous pleurisy. The optimal number of pleural biopsy specimens for a diagnosis of tuberculous pleurisy. The prevalence of pulmonary parenchymal tuberculosis in patients with tuberculous pleuritis. Comparison of polymorphonuclear- and lymphocyte-rich tuberculous pleural effusions. Interferon gamma release assays for diagnosis of pleural tuberculosis: a systematic review and meta-analysis. Improved diagnosis of pleural tuberculosis using the microscopicobservation drug-susceptibility technique. Amplified mycobacterium tuberculosis direct test for diagnosing tuberculous pleurisy-a diagnostic accuracy study. The incidence and clinical correlates of parapneumonic effusions in pneumococcal pneumonia. Temporal trends of invasive disease due to Streptococcus pneumoniae among children in the intermountain west: emergence of nonvaccine serogroups. Complicated parapneumonic effusion in Belgian children: increased occurrence before routine pneumococcal vaccine implementation. Comparison of invasive pneumococcal disease caused by serotype 19a and non-19A pneumococci in children: more empyema in serotype 19a invasive pneumococcal disease. Pneumonia with empyema among children in the first five years of high coverage with 13-valent pneumococcal conjugate vaccine. Microbial aetiology of paediatric pneumonia complicated with parapneumonic effusion in the era of pneumococcal vaccination. Microbiological diagnosis of empyema in children: comparative evaluations by culture, polymerase chain reaction, and pneumococcal antigen detection in pleural fluids. Serotype distribution and susceptibility of Streptococcus pneumoniae isolates from pleural fluid in Spain from 1997 to 2008. Clinical characteristics and outcomes of patients with community-acquired, health care-associated, and hospital-acquired empyema. Pneumonia and empyema caused by streptococcus intermedius that shows the diagnostic importance of evaluating the microbiota in the lower respiratory tract. A higher significance of anaerobes: the clone library analysis of bacterial pleurisy. Clinical relevance and characteristics of pleural effusion in patients with Mycoplasma pneumoniae pneumonia. Lower respiratory tract infections caused by Haemophilus influenzae: clinical features and predictors of outcome. A 10-year experience with bacteriology of acute thoracic empyema: emphasis on Klebsiella pneumoniae in patients with diabetes mellitus.
Purchase genuine ramipril on line
The renal abnormalities range from minimal proteinuria to profound renal failure; postmortem studies have found focal acute tubular injury and minimal glomerular damage blood pressure side effects buy ramipril overnight delivery. Nonetheless, even small acute increases in serum creatinine are associated with decreased long-term survival in critically ill patients. The cardiac depression associated with septic shock reflects the effects of inflammatory mediators on cardiac myocyte and microcirculatory function, is not caused by ischemia, and usually does not require inotropic therapy. However, if hypovolemic shock cannot be reversed by administering intravenous fluids, the use of vasopressors is indicated to restore tissue perfusion pressure. Adrenergic agonists are the first-line vasopressors, norepinephrine being the first-choice agent. Mechanisms implicated in the development of sepsis-induced myocardial depression include alterations in calcium homeostasis, mitochondrial dysfunction, apoptosis, circulating cardiosuppressant mediators, and nitric oxide. A postmortem study found that cardiac 994 Brain dysfunction in sepsis may manifest as coma or delirium. Patients who experience severe sepsis may have cognitive and functional defects that last for years. Clinical features include difficulty in weaning from a ventilator, generalized wasting of the limbs, and diffuse weakness. Skin manifestations of sepsis include a cutaneous reaction at a local inoculation site (pustule, eschar), lesions that appear at sites of hematogenous seeding of the skin or underlying soft tissue (petechiae, pustules, ecthyma gangrenosum, cellulitis), diffuse eruptions caused by bloodborne toxins. Other common manifestations of sepsis include altered glycemic control, adrenal dysfunction, and sick euthyroid syndrome. There is substantial variability in the reported incidence and mortality of sepsis depending on the case definitions and diagnosis codes used to identify patients. Abnormalities range from subclinical coagulation disorders to prolongation of clotting times (most notably prothrombin time and partial thromboplastin time), low platelet counts, and elevated D-dimer levels. Coagulopathy and Disseminated Intravascular Coagulation Mortality Gastrointestinal Tract and Hepatic Injury Trends in Time: Incidence and Mortality In the past 2 decades, numerous studies have suggested that the incidence of sepsis is increasing over time, while mortality is decreasing. In the absence of comorbidities and older age, the case-fatality rate of severe sepsis or septic shock was less than 5% in 2012. People at the highest risk of developing sepsis include infants and elderly adults as well as patients with chronic or serious illnesses such as diabetes and cancer and patients with an impaired immune system. Potential explanations for this sex difference include gender dissimilarities in behavior, social factors, chronic comorbidities, and the effect of sex hormones. Environmental factors and socioeconomic status also influence the incidence of sepsis. For example, poor socioeconomic status enhances the risk for bloodstream infection. Patients with cancer have a threefold to fourfold increased risk to be hospitalized for sepsis compared with the overall population. The risk of death in patients with cancer compared with patients without cancer who acquire sepsis is approximately 50% higher. Even so, there is evidence that chronic comorbidities have an impact on both infection risk and sepsis outcome. For example, patients with diabetes have an increased risk of developing infections and sepsis. Some studies have shown an association with increased mortality, others found no effect, and still others found improved survival. Compared with Western Europe and North America, the prevalence of gram-negative infections in Eastern Europe, Central and South America, and Asia is significantly higher, mainly caused by higher numbers of Klebsiella spp. For example, in northeast Thailand, melioidosis is among the most common causes of community-acquired sepsis, as illustrated by the finding that its causative agent, Burkholderia pseudomallei, is the cause of 20% of community-acquired bloodstream infections. First, they must adhere to and traverse the mucosal barrier, after which they must multiply and overcome antimicrobial host defense systems. Bacteria can coordinate their gene expression according to the density of their local population in a process known as quorum sensing. Activation of quorum sensing can help a bacterial population to remain inactive and not express virulence factors to avoid detection by the host or-at the other side of the spectrum-increase the expression of virulence factors and launch a coordinated overpowering attack on the host. Pathogens can also injure the host by the expression of toxins that damage natural barriers such as the mucosa to enable further bacterial spread. Toxic shock syndrome is caused by the production of so-called superantigens during an invasive streptococcal infection or a localized staphylococcal infection. The bacterial production of these exotoxins cause nonspecific activation of T cells, resulting in the massive release of proinflammatory cytokines. In sepsis the pathogen has succeeded in evading protective immunity, while continuing to stimulate host cells, resulting in an unbalanced and harmful immune response and a failure to return to homeostasis. Knowledge of the course of immune dysregulation during infection is almost exclusively derived from animal studies, which are limited by lack of sufficient relevance for sepsis in humans. Most investigations on the host response in patients during sepsis have been done on admission to the hospital, thereby not affording information about the time course and character of the immune response before clinical recognition of severe disease and the diagnosis of sepsis. In patients with sepsis with a prolonged clinical course, the disturbances in the host response involve different leukocyte subsets and parenchymal cells, encompassing key functions at both intercellular and intracellular levels, such as barrier function of epithelium and endothelium and cellular metabolism and mitochondrial dysfunction. In the next section, we describe the most important features of the septic host response. The widespread emergence of antibiotic resistance genes among bacteria, viruses, fungi, and even protozoa has led to enormous challenges in the treatment of sepsis. Not only will empirical antibiotic treatment be less efficient, the same holds true for the chosen definitive antibiotic treatment. Equally worrisome is the finding that antibiotic-resistant bacteria can increase the total burden of sepsis. These results highlight the growing challenge of bloodstream infections that are effectively impossible to treat in resource-limited settings. In the Netherlands, for example, the proportion of extendedspectrum cephalosporin-resistant E. As an example, a study from Western Europe did not find an association between inadequate treatment and mortality of S. Nucleotide-binding oligomerization domain-like receptors include inflammasomes, which are cytosolic multimolecular complexes that sense intracellular microbial danger signals and metabolic perturbations. Activation of nuclear factor kappa B is key for induction of the inflammatory response, resulting in the transcription of multiple early activation genes including those encoding cytokines. These cytokines are released in the circulation in animals challenged with high doses of bacteria or their products, and in these models their inhibition or elimination protects against organ damage and mortality. Patients with sepsis display elevated circulating levels of S100A8/9, and mice deficient for this protein are protected from endotoxin shock and E. Besides cytokines, several other mediator systems have received attention with regard to their potential involvement in sepsis pathogenesis, most notably the complement system, the coagulation system, and the vascular endothelium. Activation of the Complement System the complement system comprises a group of small proteins mostly synthesized by the liver that typically circulate as inactive precursors. On complement activation, small activation fragments known as anaphylatoxins are generated, particularly C3a and C5a, which exert strong proinflammatory effects on leukocytes, endothelial cells, and platelets. Uncontrolled activation of complement can cause collateral damage to surrounding tissues and multiple organ failure at the systemic level. Inhibition of C5a improved the outcome in several animal sepsis models including E. Tissue factor also can be present in microparticles derived from leukocytes, endothelial cells, vascular smooth muscle cells, and platelets. Perivascular cells such as fibroblasts, pericytes, and epithelial cells express tissue factor constitutively, thereby safeguarding hemostasis and vessel integrity. Platelets are small circulating anucleate cells that are of vital importance in hemostasis. In addition, von Willebrand factor can activate platelets by binding platelet glycoprotein Ib.
Discount ramipril 2.5 mg fast delivery
In two meta-analyses of well-conducted trials hypertension history cheap 10 mg ramipril overnight delivery, aminoglycoside-based regimens were deemed inferior compared with several other regimens for the treatment of patients with intraabdominal infections. An aminoglycoside may be included with a -lactam antibiotic in the initial antimicrobial regimen for patients who are critically ill or in whom a resistant pathogen. The fluoroquinolones (norfloxacin, ofloxacin, ciprofloxacin, levofloxacin, and moxifloxacin) are active against almost all aerobic gram-negative bacilli. Levofloxacin and moxifloxacin are more active than the older fluoroquinolones against gram-positive cocci, although enterococci and methicillin-resistant S. In contrast to other fluoroquinolones, moxifloxacin is active against obligate anaerobes. The addition of an antimicrobial agent active against anaerobic bacteria and aerobic or microaerophilic gram-positive cocci. The use of levofloxacin, even combined with a second agent with reliable activity against anaerobic gram-negative bacilli for the treatment of intraabdominal infections, does not have any published support, and perhaps this fluoroquinolone should be reserved for respiratory and urinary tract infections for which it may be better suited. It has been determined to be noninferior to -lactam/-lactamase inhibitors, cephalosporin-based regimens, and carbapenems in several comparator studies. The first glycylcycline antibiotic approved for the treatment of complicated intraabdominal infections was tigecycline. In addition, tigecycline has reliable activity against vancomycin-resistant strains of enterococci and methicillin-resistant S. One limitation with the use of tigecycline may be the relatively high incidence of nausea and vomiting experienced by patients treated with this agent. Eravacycline, an injectable synthetic fluorocycline antibiotic, belongs to the tetracycline group of antibiotics. Dosing is weight-based given as an intravenous infusion at 1 mg/kg every 12 hours, with no required adjustment of dose required in patients with renal impairment. A Cochrane Collaboration review of antimicrobial therapy for intraabdominal infections was unable to demonstrate clinical superiority of any one regimen. In cases in which exact clinical efficacy data are ambivalent, pharmacodynamic modeling may be a useful adjunct in choosing a treatment regimen. Antibiotic therapy should be given before, during, and after surgery to ensure adequate tissue and blood levels at which the antibiotic can combat local and metastatic spread of the infection. The duration of antimicrobial therapy after adequate surgery is usually 4 to 7 days and depends on severity of infection, clinical response, and normalization of the leukocyte count. The utility and proven benefit of antibiotic therapy to decrease secondary infection in noninfectious intraabdominal inflammatory disease has been an area of controversy. Quite often antibiotics are given to patients diagnosed with acute necrotizing pancreatitis who do not have a secondary infection complication. However, meta-analyses have failed to demonstrate any significant proven benefit, and the risks of bacterial resistance and complications, such as C. Similarly, a 5-year follow-up of antibiotic therapy alone for uncomplicated appendicitis had similar outcomes as in patients who underwent an appendectomy; the likelihood of late recurrence within 5 years was 39. Patients able to tolerate oral intake may switch to oral therapy after an initial response to intravenous therapy. When ileus no longer precludes oral intake, efficacy of oral therapy depends on the adequacy of absorption after oral administration of the antimicrobial agents, the availability of potent oral agents against the significant aerobic and anaerobic gram-negative bacilli and gram-positive cocci pathogens. The potential oral agents most studied for this purpose include amoxicillin-clavulanate, ciprofloxacin with metronidazole, and moxifloxacin, with recognition of the heightened prevalence of E. Levofloxacin is often substituted as the fluoroquinolone component but has never been studied for this purpose. Likewise, the oral cephalosporin drugs and trimethoprim-sulfamethoxazole have little proven evidence as antibiotics for the treatment of intraabdominal infections, but may be potential treatment options in specific cases. Although in many studies the orally administered antibiotics allowed treatment courses longer than the current recommendation of 4 to 7 days, the purpose of the switch should be the intention to shorten the length of parenteral antibiotic administration. Povidone-iodine has been shown to be a potent inactivator of neutrophil functions such as chemotaxis and phagocytosis, however, and may have a detrimental effect. The increased oxygen tension attainable with hyperbaric oxygen therapy inhibits and kills C. Hyperbaric oxygenation has been used clinically and experimentally for clostridial myonecrosis with some reported success. However, except for a few reports,297 almost no clinical or experimental data are available. Hill298 reported suppression of experimental liver abscesses caused by anaerobes in mice after treatment with hyperbaric oxygen therapy alone. In one study, it seemed that the use of hyperbaric oxygen therapy favorably affected the outcome of experimental sepsis in a rat model, perhaps by enhancing host defense mechanisms. If no distention is present when treatment is instituted, continuous gastric suction is usually sufficient. For patients with distention when treatment is started and for patients who acquire distention despite gastric drainage, the small intestine should be intubated. Water and Electrolyte Administration the type of fluid replacement is determined in large part by the chemical abnormalities found. Early goal-directed volume resuscitation is essential in treating uncomplicated intraabdominal infections but becomes critical in cases of severe sepsis or septic shock. Regardless of whether the end point for resuscitation is mixed venous oxygen (>65%), correction of lactic acidosis, or normalization of base deficit, the goal of volume resuscitation is correction of cellular oxygen. With regard to the types of fluids, timing, and amounts to be given, the recommendations put forth in the Surviving Sepsis Campaign should be followed. Inflammation of the parietal peritoneum, including the diaphragmatic surface, leads to guarding and splinting of the muscular wall, which interferes with deep breathing and coughing. These factors impair the ability to augment respiratory exchange in the presence of the increased expenditure of energy required by the inflammatory process, and this leads to hypoxemia and respiratory alkalosis. When the patient tires, the combination of metabolic and respiratory acidosis may develop and prove fatal. Arterial blood gas studies are necessary to detect and quantitate respiratory decompensation. Measures aimed primarily at gastrointestinal decompression, elevation of the head of the bed, and control of the inflammation may improve respiration sufficiently. If these measures are inadequate, endotracheal intubation or tracheostomy should be performed without delay. A volume-cycled respirator should be used and adjusted to produce a partial pressure of oxygen of 80 to 100 mm Hg and a normal pH. If the partial pressure of carbon dioxide is then not normal, metabolic acidosis or alkalosis may be present and must be treated. As the intraabdominal process subsides, the patient may be able to breathe spontaneously again and may be weaned from the ventilator. Acute increase in intraabdominal pressure, which itself can lead to multiorgan dysfunction. Stable, noncritical patients with localized intraabdominal infections including perforated appendicitis with localized phlegmon or periappendiceal abscesses; acute colonic diverticulitis with inflammation into the adjacent colonic tissues or small abscesses; and localized upper gastrointestinal perforations, may be treated conservatively with antibiotics alone, at times. Continuous postoperative peritoneal lavage for 48 to 72 hours or until the fluid is clear, with the use of large volumes of fluid to ensure dispersion of the fluid and to prevent loculations, has, however, not been effective. On resolution of the septic process and establishment of granulation, the mesh would be removed and a skin graft would be applied to the granulating bed. These demanding and costly procedures have been complicated by multiple fistulas, wound contamination, incisional hernias, and secondary peritonitis with organisms such as enterococci or Candida spp. A review concluded that in the absence of randomized, controlled prospective trials with appropriate stratification of patients by severity of illness, evidence is now insufficient to determine whether these procedures improve outcome in severe diffuse peritonitis; nevertheless, they may be lifesaving in some patients. Less invasive source-control procedures, including interventional radiologic percutaneous drainage of intraabdominal and pelvic fluid collections, are increasingly relied on when the infection is localized and a safe window for introduction of the drainage tube exists.
