
Buy discount antabuse 250mg on line
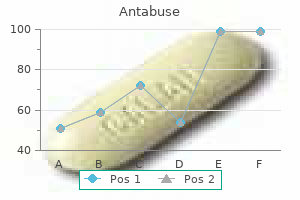
This article symptoms 6 days after iui cheap 500mg antabuse fast delivery, therefore, includes both scale-up and scale-down considerations that are important for the commercial lyophilization process development. It must be noted that the discussion in this chapter focuses on lyophilization in vials. It is recognized that lyophilization is also conducted in other container closures, for example, syringes, dual-chamber cartridges, and trays for bulk lyophilization. Many of the principles discussed here are general Science of Scale for Freeze Drying and applicable to any container closure configuration. However, heat and mass transfer models for drying are primarily available for vials. Design freeze-drying process in such way that estimated product temperature profile would essentially match the product temperature in laboratory-scale lyophilization. This should, in principle, ensure identical or very similar product thermal history (same degree of crystallinity of bulking agent; similar pore size, if difference in the degree of ice nucleation is compensated by additional annealing; similar extent of phase separation within cake; etc. Importantly, if an appropriate model is established, it allows accounting for the process variability during commercial manufacturing. One of the goals of lyophilization cycle technology transfer team is to design a robust process that could withstand the majority of stresses due to anticipated deviations in process parameters. To ensure that cycle could produce acceptable material within wide range of process parameters, a robustness study (not necessarily on the commercial scale) should be performed and stability of product, made at extreme cycle conditions, should be assessed, thus, creating drug product temperature design space (or allowed product temperature range). In addition, an "extreme" robustness study to identify the edge of failure may also be performed. For example, a product could be stressed well above the known critical temperature to simulate an unexpected deviation. Robustness experiments performed at the laboratory scale can be employed to suitably assess the effect of deviations during commercial manufacturing on product quality if the link between development and commercial lyophilizers is firmly established [11], meaning that resulting product temperature, as consequence of deviation, could be estimated and compared to established product temperature design space. Presumably, drying above collapse will result in loss of product elegance, but that may be the only impact. Science of Scale and Technology Transfer the change in scale from laboratory- to pilot- or commercialscale dryers has an impact on product and, in many cases, requires modifications to the laboratory-scale lyophilization processes. There are no strict rules or set of equations that one can use to design a commercial-scale cycle. However, previous experience, common sense, and good knowledge of heat and mass transfer are all helpful in assessing scalability of the laboratory process. Review design and characteristics of pilot or commercial freeze dryer to which cycle would be transferred (ramp rates, minimum cooling temperatures for shelf and condenser, temperature distribution across the shelf and between shelves, evacuation time and minimum pressure, condenser capacity, pressure control options). With exception of condenser capacity test, which involves sublimation test with predetermined amount of water to challenge the condenser performance, the majority of tests are performed on "dry and empty dryer. This will allow estimation of appropriate cooling and warming rates for fully loaded dryer with predetermined criteria for temperature heterogeneity. Sublimation tests, described by Rambhatla and Pikal [10], could also be performed to test freeze-dryer performance and establish relationship between the sublimation rate and the pressure that could be controlled (Pmin-minimum controllable pressure) at a particular load conditions or determine maximum sublimation rate for a dryer. Lastly, vial heat transfer coefficients and edge factor could be measured on the pilot or commercial dryers to account for the differences in heat transfer. All this additional information could be used as inputs in the model that allow establishing a "link" between laboratory dryer and commercial dryer to enable the most efficient process transfer and scale-up. Having established model will also help to address any deviations during commercial manufacturing. Scale-Up Considerations the main reason for complications during lyophilization scale-up is the difference between small-scale (laboratory) and large-scale (pilot and commercial) dryers in the heat transfer, resistance to mass flow and ability to capture water vapor, product cake resistance and difference in process control. If channels pattern is not provided by the manufacturer, one could use a simple "condensation test": open the freeze-dryer door, allow humid air to enter the chamber, and cool shelves at the maximum cooling rate. The condensation of water on the surface of shelves will reveal the pattern of the channels and could help in identification of proper thermocouple positions. At a similar rate, maximum temperature gradient across the shelf in a commercial size dryer was about 11. The large heat capacity of shelves in a commercial freeze dryer is the source of significant temperature gradients during nonsteady (ramps) conditions. The difference in shelf design between laboratory- and commercial-scale dryers is another source of variability. In laboratory-scale dryer, the channels are normally small compared to the large-scale dryer. Based on shelf design, the heat to the surface of shelf can be supplied either through the Differences in Heat Transfer between Laboratory and Commercial Dryers In lyophilization, the size of dryers does indeed matter. While manufacturers of freeze-drying equipment are trying to use the same principles of design when they build large-scale dryers, it is difficult, or economically inefficient, to match the laboratoryscale dryer in ability to quickly adjust process parameters when it is needed. This indicates that slow cooling rates are necessary in order to minimize the differences in product temperature profiles during cooling between laboratory and commercial processes. In most commercial freeze dryers, inlet and outlet are also positioned on opposite sides of the shelf. In the commercial dryer, the size of vial could be comparable to the size of channels. In this case, some vials could be located over a "cold" spot, whereas neighboring vials could be sitting over a "hot" spot, creating more heterogeneity at large scale in regard to the heat transfer. The bumps in the graphs representing temperature difference between inlet and outlet likely indicate a sporadic crystallization of water upon heterogeneous freezing. An increase in the size of the dryer from 6 to 42 m2 resulted in significant increase in the temperature difference across the shelf surface. The temperature difference across the shelf between different scale dryers translates into the difference in product temperature in vials positioned in different locations. Brown line represents the shelf surface temperature difference, measured during cooling of fully loaded (6,000 of 20 mL vials filled with 5 mL water) 6 m 2 dryer at approximately 0. Blue line represents the shelf surface temperature difference measured during cooling of the partially loaded (2 shelves out of 15, filled with 2. Left panel represents fully loaded 6 m 2 dryer, and right panel represents partially loaded 42 m2 dryer. Note that only data set prior to onset of water crystallization was used to calculate the difference in product temperature. The apparent fluctuation in temperature difference is due to fluctuations of inlet temperature during the ramps. The difference between inlet and outlet temperatures should, in principle, be a function of sublimation or desorption rates. Without knowledge of the exact geometry inside the shelf and accurate temperature distribution within the shelf, it is almost impossible to calculate Kheat tranfer, but it can be estimated from the experiment. The Kheat tranfer for different types of dryers can be estimated from Equation 36. Note that laboratory dryers have the highest heat transfer coefficient (slope has the lowest value) compared to the commercial-scale dryer and, especially, to older pilot freeze dryer. The slope in linear fit equations, shown on the graph for different freeze dryers, is proportional to the shelf heat transfer coefficient. The difference in heat transfer within shelves of laboratory and commercial dryers converts to the difference in vial heat transfer coefficient (Kv) between laboratory and commercial dryers. The values of Kv as a function of pressure for both laboratory-scale and pilot-scale dryers were calculated using Equation 36. The water weight loss during drying was measured for at least 25 vials, positioned in the area not affected by the edge effect. The experiments were performed at different pressures (at least 4 pressure points), calculated values of Kv were fit to Equation 36. Fissore and Barresi [16] proposed using only one test at larger scale to estimate coefficient a in Equation 36.
Buy antabuse 500 mg visa
Medication adherence may require verification with the pharmacist k-9 medications order antabuse now, caregivers, or family. Transitions in patient care, such as hospital to sub-acute nursing facility or home, lead to medication errors because medications may have been deleted or added. Patient Education Geriatric patients often have difficulty understanding and retaining provider instructions. Medicare covers all or part of the cost of skilled nursing care for a limited period post hospitalization. Nursing homes are highly regulated by state and federal government through the Center for Medicare and Medicaid Services. Such a team approach is vital to coordinate care for the typical frail, complex long-term care patient. Health, United States, 2015: With a Special Feature on Racial and Ethnic Health Disparities. The health consequences of smoking-50 years of progress: a report of the surgeon general. Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health. Pharmacokinetics and pharmacodynamic changes associated with aging and implications for drug therapy. Age-related pharmacokinetic and pharmacodynamic changes and related risk of adverse drug reactions. Drug metabolism in older people-a key consideration in achieving optimal outcomes with medicines. Changes in prescription and over-the-counter medication and dietary supplement use among older adults in the United States, 2005 vs. Inappropriateness of medication prescriptions to elderly patients in the primary care setting: a systematic review. American Geriatrics Society 2015 updated Beers Criteria for potentially inappropriate medication use in older adults. Underprescription of beneficial medicines in older people: causes, consequences and prevention. Drug-related-problem outcomes and program satisfaction from a comprehensive brown bag medication review. Adverse drug events after hospital discharge in older adults: types, severity, and involvement of Beers Criteria medications. Incidence and preventability of adverse drug events among older persons in the ambulatory setting. Drug-related falls in older patients: implicated drugs, consequences, and possible prevention strategies. Assessing medication adherence in the elderly: which tools to use in clinical practice The mini-cog: a cognitive "vital signs" measure for dementia screening in multilingual elderly. Transitional care management service: optimizing medication reconciliation to improve the care of older adults. Identify factors that affect selection of safe and effective drug therapy in pediatric patients. Explain general pharmacokinetic and pharmacodynamic differences in pediatric versus adult patients. Develop strategies for appropriate and effective medication administration to infants and young children. Determine approaches to effectively communicate with patients and caregivers about appropriate medication use including expected outcomes, possible adverse effects, and appropriate administration. These markers of growth and development are both age- and gender-dependent; thus, the use of the correct tool for measurement is important. Failure to thrive is defined as inadequate physical growth with weight that falls below the 5th percentile or decreases over time, crossing two or more major percentile lines. Clinicians serve as advocates for this unique and vulnerable patient population to optimize their well-being. Care for pediatric patients is relevant in both inpatient and outpatient settings and requires additional considerations with regard to selection and monitoring of drug therapy. Despite the common misconception of pediatric patients as "smaller adults" where doses are scaled only for their smaller size, there are multiple factors to consider when selecting and providing drug therapy for patients in this specific population. Pediatric patients significantly differ within their age groups and from adults regarding drug administration, psychosocial development, and organ function development, which affect the efficacy and safety of pharmacotherapy. Normal values for blood pressure vary based on gender and age for all pediatric patients, and also height percentile for patients older than 1 year. Normal values for blood pressure in pediatric patients can be found in various national guidelines and other pediatric diagnostic references. In general, blood pressure increases with age, with average blood pressures of approximately 70/50 in neonates, increasing throughout childhood to approximately 110/65 in adolescents. As a newborn continues to progress to infant, child, and adolescent stages, different variables are monitored to assess growth compared with the general population of similar age and size. Another vital sign commonly monitored in children by their caregivers is body temperature, especially when they seem "warm to the touch. For those 3 months and older, use of temporal artery measurement is an available option. Axillary measurement is not considered first-line in this all age groups, as proper technique is important for accurate measurement and other accurate options are available. Indicators of possible pain include physiological changes, such as increased heart rate, respiratory rate, and blood pressure, decreased oxygen saturation, as well as behavior changes such as prolonged, high pitch crying, and facial expressions. Maintenance fluid requirement can be calculated based on body surface area for patients greater than 10 kg, with a range of 1500 to 2000 mL/m2 per day. It is noteworthy that pediatric patients may require the use of different medications from those used in adults affected by certain diseases. There also exist commonalties between pediatric and adult patients, such as therapeutic serum drug concentrations required to treat certain diseases. For example, gentamicin peak and trough serum concentrations needed for bacteremia treatment are the same in children and adults. Appropriate selection and dosing of drug therapy for a pediatric patient depends on a number of specific factors, such as age, weight, height, disease, comorbidities, developmental pharmacokinetics, and available drug dosage forms. Pediatric drug doses are often calculated based on body weight (eg, mg/kg/ dose) compared with uniform dosing (eg, mg/day or mg/dose) for adult patients. Thus, accurate weight should be available while prescribing or dispensing medications for this patient population. Pediatric doses may exceed adult doses by body weight for certain medications due to differences in pharmacokinetics and pharmacodynamics; hence, the use of pediatric drug dosing guides is recommended. For off-label medication dosing, when no alternative treatment is available and limited dosage guidelines have been published, clinicians may estimate a pediatric dose based on body surface area ratio. Beats per minute b Breaths per minute c mm Hg d Exact normal values will vary based on age, height, and sex. L O 3 L O 3 due to lower gastric acid output by body weight, reaching adult values by approximately 2 years of age.
Purchase antabuse 250mg on line
When initiating therapy medications 25 mg 50 mg purchase antabuse 500 mg with visa, monitor serum levels every 1 to 4 weeks, depending on the severity of hyperphosphatemia. Once target levels are achieved, monitor serum calcium and phosphorus levels every 1 to 3 months. Patients who develop hyperkalemia should restrict dietary intake of potassium to 50 to 80 mEq (mmol) per day. Acute hyperkalemia that results in cardiac abnormalities can be managed with calcium, insulin, and dextrose. Patiromer is a nonabsorbed potassiumbinding polymer that is used for the treatment of hyperkalemia. Mild hyperkalemia and metabolic acidosis are generally not associated with overt symptoms. Symptoms of chronic metabolic acidosis present as bone abnormalities and growth retardation in children. Electrolyte disorders resulting from an acute increase in intake can be more severe and prolonged. Changes in sodium intake should occur slowly over a period of several days to allow adequate time for the kidney to adjust urinary sodium content. Sodium restriction produces a negative sodium balance, which causes fluid excretion to restore sodium balance. Fluid restriction is generally unnecessary as long as sodium intake is controlled. Fluid intake should be maintained at the rate of urine output to replace urine losses, usually fixed at approximately 2 L/day as urine concentrating ability is lost. Significant increases in free Outcome Evaluation Monitor serum electrolytes and bicarbonate levels regularly. Monitor fluid intake to ensure obligatory losses are being met and avoid dehydration. If adequate diuresis is not attained with a single agent, consider combination therapy with another diuretic, such as a loop plus thiazide diuretic. Evaluate serum potassium and glucose levels within 1 hour in patients who receive insulin and dextrose therapy. Monitor blood pressure and serum potassium levels in 1 week after starting fludrocortisone. Correct metabolic acidosis slowly to prevent the development of metabolic alkalosis or other electrolyte abnormalities. Parameters of adequacy of dialysis are better defined and therefore underdialysis can be detected early. Even though intermittent heparinization is required, hemostasis parameters are better corrected with hemodialysis than peritoneal dialysis. Requires multiple visits each week to the hemodialysis center, which translates into loss of control by the patient. Infections in hemodialysis patients may be related to the choice of membranes; the complement-activating membranes are more deleterious. Decline of residual renal function is more rapid compared with peritoneal dialysis. Ideally, initiation of dialysis should be done at a point when the patient is ready to undergo treatment, rather than when the patient is in emergent need of dialysis. Symptoms that may indicate the need for dialysis include persistent anorexia, nausea, vomiting, fatigue, and pruritus. Other criteria that indicate the need for dialysis include declining nutritional status, declining serum albumin levels, electrolyte abnormalities, particularly hyperkalemia, and volume overload, which may manifest as chronic heart failure and uncontrolled hypertension. The dialyzer is composed of thousands of capillary fibers made up of the semipermeable membrane, which are enclosed in the dialyzer, to increase the surface area of blood exposure to maximize the efficiency of removing substances. The dialysate is composed of purified water and electrolytes, and it is run through the dialyzer countercurrent to the blood on the other side of the semipermeable membrane. The process allows for the removal of several substances from the bloodstream, including water, urea, creatinine, electrolytes, uremic toxins, and some drugs. Sterilization is not required for dialysate because the membrane prevents bacteria from entering into the bloodstream. Three types of membranes used for dialysis are classified by the size of the pores and the ability to remove solutes from the bloodstream: low flux, high efficiency, and high flux. Low flux membranes have small pores, which limit solute removal to relatively small molecules, such as creatinine and urea. Highefficiency membranes also have small pores but have a higher surface area that increases removal of small molecules, such as water, urea, and creatinine from the blood. The most widely used dialyzers are high-flux membranes which larger pores allow for the removal of substances with higher molecular weight, including some drugs, such as vancomycin. At times, solutes can be added to the dialysate that are diffused into the bloodstream. Changing the composition of the dialysate allows for control of the amount of electrolytes that are being removed. Increased clearance of larger solutes, which may explain good clinical status in spite of lower urea clearance 3. Convenient intraperitoneal route of administration of drugs such as antibiotics and insulin 5. Suitable for elderly and very young patients who may not tolerate hemodialysis well 6. Freedom from the "machine" gives the patient a sense of independence (for continuous ambulatory peritoneal dialysis) 7. Less blood loss and iron deficiency, resulting in easier management of anemia or reduced requirements for erythropoietin and parenteral iron 8. Protein and amino acid losses through the peritoneum and reduced appetite owing to continuous glucose load and sense of abdominal fullness predispose to malnutrition 2. Inadequate ultrafiltration and solute dialysis in patients with a large body size, unless large volumes and frequent exchanges are employed 5. Mechanical problems such as hernias, dialysate leaks, hemorrhoids, or back pain may occur 8. An anticoagulant (usually heparin) is administered to prevent clotting in the dialyzer. The dialysate is pumped at the rate of 500 to 1000 mL/min through the dialyzer countercurrent to the flow of blood. The rate of fluid removal from the patient is controlled by adjusting the pressure in the dialysate compartment. Changing the hydrostatic pressure applied to the dialyzer or the osmotic concentration of the dialysate allows for control of the amount of water being removed. Changing the pore size of the dialyzer membrane alters the efficiency of convection and allows for control of the amount of water removed in relation to the amount of solute being removed. The catheters are tunneled beneath the skin to an exit site to reduce the risk of infection. Venous catheters can also be used as permanent access in patients in whom arteriovenous access cannot be established. However, venous catheters carry the greatest risk of complications, namely thrombosis and infections. Ultrafiltration removes fluid from the plasma, which promotes redistribution of fluids from extracellular spaces into the plasma. Elderly age, diabetes, autonomic neuropathy, uremia, and cardiac disease also increase the potential for hypotension. The cause of infection is usually related to organisms found on the skin, namely Staphylococcus epidermidis and S. The predominant types of vascular access for chronic dialysis patients are (A) the arteriovenous fistula and (B) the synthetic arteriovenous forearm graft. The first primary arteriovenous fistula is usually created by the surgical anastomosis of the cephalic vein with the radial artery. The flow of blood from the higher-pressure arterial system results in hypertrophy of the vein.
Generic antabuse 250mg without a prescription
The inability to associate quality attributes with safety and efficacy increases the level of uncertainty in assessing risk medicine in ancient egypt buy 250 mg antabuse overnight delivery. Furthermore, the inherent difficulty to precisely characterize many biological molecules reduces the opportunities to develop concrete process understanding. QbD principles can be utilized for large-molecule drug product development (formulation and process) can be performed and are illustrated in sections below. Design Space for Drug Product Drug product development typically includes an assessment of the formulation (via a DoE study) and the manufacturing process. In this section, an example of a formulation DoE is provided, which defines the factors that impact the quality attributes. This will be followed with an assessment of one unit operation lyophilization where the important parameters that impact quality attributes are defined. Based on the assessment of prior knowledge, impact of formulation excipients on the quality attributes during storage needs to be assessed. A formulation DoE design was prepared for a protein at a concentration of 150 mg/mL. The study was performed with 1 mL fill volume in a prefilled syringe with a coated plunger for closure. A full-factorial experimental design was utilized, for studying each factor individually and the interactions between the factors. A total of 15 different formulations including the formulations with varying excipient levels, and dual center point formulation were evaluated during the stability study. A significant change in percent total impurities was seen in samples at the high and low pH conditions during storage for up to 6 months. Risks should be characterized by their respective and relevant relationship to quality attributes and process parameters and documented in a logical manner that shows the relationships between product quality and the attributes and parameters that influence quality. A general summary of the risk assessment approach and justifications for decisions regarding the attributes and parameters that warrant concern is helpful to regulatory authorities and should be transparent and reproducible. In a regulatory submission, a description of the process used to evaluate and characterize risks should be provided. Use of QbD Principles in Protein Drug Product Development QbD principles are applicable to both small-molecule drugs and large molecular biologics. However, the challenges of executing risk assessments are greater for a biological because the large size molecule (biological molecule) is vastly more complex and the impact of attributes and process parameters on product quality attributes is generally more uncertain than for small molecules. In addition, the complicated nature of generating biological molecules from living organisms can lead to significant product heterogeneity. The inherent complexity of biological 820 showed a variation which is expected for proteins stored at stress conditions. In addition to assessing the formulation, the manufacturing process also needs to be assessed. In this article, the authors have performed a QbD-based assessment of the lyophilization process. Loading of the filled partially stoppered vials on to the shelves of the lyophilizer, freezing and annealing the product in the vials 2. For each process step, the parameters that impact quality attributes were assessed and are listed as follows: 1. Based on prior knowledge and published literature, the parameters that were found to have a higher potential impact on product quality are further defined. A formulation was defined for a model monoclonal antibody (mAb-1), a sucrose-based formulation at an optimal pH and also containing polysorbate 80. Lyophilization cycle definition and optimization Process ranging DoE for assessing annealing process Impact of ice nucleation. Following the definition of the baseline cycle, the cycle was optimized using experimental data and modeling. The lyophilization cycles were optimized cycle (Run 1), high ranging cycle (Run 2), low ranging cycle (Run 3A), and conservative (Run 4). The product quality of lyophilized samples subjected to the low and high ranging cycles as well as the conservative and optimized cycles was assessed. Secondary structure changes relative to the liquid state are often found to be reversible upon reconstitution [48]. The impact of ice nucleation was evaluated to assess whether the differences in ice nucleation prior to primary drying would impact product quality. The ice nucleation was altered using different techniques, and there were no significant changes in product quality when these samples were assessed. The modification of the freezing portion of the optimum lyophilization cycle of mAb-1, either by slowing the ramp or by using a vacuum to reduce supercooling or by fast freezing in liquid nitrogen, was assessed. The ice nucleation conditions did not result in any significant changes in product quality as measured by appearance, moisture, long-term stability, or solid-state characteristics of the resulting lyophilized drug product. Impact of the level of cake moisture on quality attribute is important to assess and define stability [49]. Primary drying and secondary drying are critical steps in freeze-drying in order to achieve low moisture levels in lyophilized cakes. In addition, the detection of the completion of primary and secondary drying steps is important to ensure that the lyophilization cycle is optimized. Chamber pressure decay data from Pirani gauge as stated before measures the thermal conductivity of the gas Parenteral Medications phase. Both techniques are measuring different properties of water vapor and therefore should agree with each other. The moisture level was assessed during secondary drying and the end point was defined at 43 hours where the moisture levels were constant (at approximately 0. Control Strategy the control strategy for a product is a comprehensive set of planned controls that reflect existing product knowledge and process understanding. In particular, an effective and contemporary change management system and knowledge management process ensures continuity and consistency in the quality control of the product. Process parameter control includes functionality linked to both process performance and product quality attributes. In adopting a QbD approach and applying the science and risk-based principles to assess quality attributes and process parameters, design space can be created to describe the boundaries within which unit operations of a manufacturing process may operate. In fact, where the risk is understood, and the severity and probability of impact are controllable, the demonstration of process control through the creation of design space could conceivably reduce the need to perform in-process testing as well.
Buy antabuse 250 mg low price
However medicinenetcom medications discount antabuse 500mg without a prescription, this relationship is consistently incorrect because the measured cations are higher than the measured anions by 10 to 12 mEq/L (mmol/L). This discrepancy results from the presence of unmeasured anions (eg, circulating proteins, phosphates, and sulfates). The concept of the increased anion gap is applied later in Patient Encounters 6 through 10. The anion gap may be artificially lowered by decreased serum albumin, multiple myeloma, lithium intoxication, or a profound increase in the serum potassium, calcium, or magnesium. However, supportive treatment of the pH and electrolytes is often needed until the underlying disease state is improved. If the anion gap was initially abnormal, serial chemistries should be followed to ensure that the anion gap resolves with treatment. Specific treatment decisions depend on the underlying pathophysiologic state (eg, dialysis for renal failure, insulin for diabetic ketoacidosis, or improving tissue perfusion and oxygenation for lactic acidosis). High anion gap metabolic acidosis is most frequently caused by lactic acidosis, ketoacidosis, and/ or renal failure. Although there is considerable variation, the largest anion gaps are caused by ketoacidosis, lactic acidosis, and methanol or ethylene glycol ingestion. Respiratory compensation requires marked increases in minute ventilation and may lead to dyspnea, respiratory fatigue, and respiratory failure. Acidemia predisposes to ventricular arrhythmias and reduces cardiac contractility, each of which can result in pulmonary edema and/or systemic hypotension. Because he has not felt well for the past week, he skipped his last three routine hemodialysis sessions. He had the onset of vomiting and confusion 2 days ago but consistently refused medical evaluation. These changes are believed to be caused by the release of calcium and phosphate during bone buffering of excess H+ ions. As previously discussed, in anion gap metabolic acidosis, the isoelectric state is maintained because unmeasured anions are present. With a normal anion gap metabolic acidosis, the isoelectric state is maintained by an increase in the measured chloride. Because of this, normal anion gap metabolic acidosis is often referred to as hyperchloremic acidosis. Patient Encounter 9 A frail, 69-year-old man is being evaluated for altered mental status. His wife says he has suffered from "stomach flu" for several days and has experienced frequent bouts of bilious emesis. He is a poorly controlled diabetic and his wife states that she stopped giving him his insulin since he has not been able to eat. She called an ambulance today when she noticed his breathing was very slow and shallow. Patient Encounter 6 A 19-year-old woman with Prader-Willi Syndrome and hyperphagia is admitted to the intensive care unit after ingesting an unknown quantity of aspirin tablets. This occurs because the urinary Cl- concentration now markedly exceeds the urinary Na+ and K+ concentrations. In order to effectively treat metabolic acidosis, the causative process must be identified and treated. Additional infusions are given as dictated by the severity and progression of acidosis. Chronic metabolic acidosis can successfully be managed using potassium citrate/citric acid (Polycitra-K, Cytra-K) or sodium citrate/citric acid (Bicitra, Oracit). Patients will always hypoventilate to compensate for metabolic alkalosis-even if it results in profound hypoxemia. Rather, complaints are usually related to volume depletion (muscle cramps, positional dizziness, weakness) or to hypokalemia (muscle weakness, polyuria, polydipsia). In order to effectively treat metabolic alkalosis, the causative process must be identified and treated. If the etiology of the metabolic alkalosis is still unclear, measurement of the urinary chloride may be useful. Some processes leading to metabolic alkalosis (eg, vomiting, nasogastric suction losses, factitious diarrhea) will have low urinary Cl- concentrations (< 25 mEq/L [mmol/L]) and are likely to respond to administration of saline. Other causes (eg, diuretics, hypokalemia, and mineralocorticoid excess) will have higher urinary Cl- concentrations (> 40 mEq/L [mmol/L]) and are less likely to correct with saline infusion. In general, contributing factors such as diuretics, nasogastric suction, and corticosteroids should be discontinued if possible. Acetazolamide is typically dosed at 250 mg every 6 to 12 hours as needed to maintain the pH in a clinically acceptable range. Arterial pH must be monitored at least hourly and the infusion stopped as soon as clinically feasible. Ammonium chloride may cause accumulation of ammonia leading to encephalopathy while arginine hydrochloride can induce life-threatening hyperkalemia through unclear mechanisms. Severe, acute respiratory acidosis produces a variety of neurologic abnormalities. If untreated, terminal manifestations include peripheral vasodilation leading to hypotension and cardiac arrhythmias. Chronic respiratory acidosis is typically associated with cor pulmonale and peripheral edema. In order to effectively treat respiratory acidosis, the causative process must be identified and treated. This may include naloxone for opiate-induced hypoventilation or bronchodilator therapy for acute bronchospasm. Because respiratory acidosis represents ventilatory failure, an increase in alveolar ventilation is required. This can often be achieved by controlling the underlying disease (eg, bronchodilators and corticosteroids in asthma) and/or physically augmenting ventilation. Although their precise role and mechanisms of action are unclear, agents such as medroxyprogesterone, theophylline, and doxapram stimulate respiration and have been used to treat mild to moderate respiratory acidosis. Patients given doxapram required monitoring of their blood pressure, pulse, and deep tendon reflexes as this drug can cause cardiac excitation and spasticity. In mechanically ventilated patients, respiratory acidosis is treated by increasing the minute ventilation. The use of tromethamine in respiratory acidosis (see Metabolic Acidosis section earlier) has unproven safety and benefit. The goals of therapy in patients with chronic respiratory acidosis are to maintain oxygenation and to improve alveolar ventilation if possible. Because of the presence of metabolic compensation it is usually not necessary to treat the pH, even in patients with severe hypercapnia. Some causes of hyperventilation and respiratory acidosis are remarkably common (hypoxemia or anemia).
Generic antabuse 500 mg fast delivery
On the other hand symptoms heart attack women purchase 250 mg antabuse free shipping, a very fast freezing rate obtained by flash-freezing droplets in liquid nitrogen was shown to have a high risk for crystallization of trehalose, with slower rates being preferable [33]. The use of "freezing rates" as a way to reduce risk for crystallization of trehalose is however fraught with danger and should not be considered a practical solution to preventing this phenomena. The freezing rates will vary with geometry and size of container, and there is a range of freezing rates in every practical system-what may be "fast" in one system may be "slow" in another. Clearly, one way to prevent crystallization of trehalose or any crystallizing excipient is to reduce the ratio of the excipient to protein, that is, poison the crystallization. However, care must be taken to ensure that there is sufficient excipient to provide a stabilizing effect, while hindering its ability to crystallize (see discussion below). Mannitol is a common excipient that readily crystallizes out of solution on cooling and thus provides no protection in the frozen state (see. A mixture that is generally used, especially in lyophilization applications, is a combination of mannitol and sucrose. If this combination has to be frozen, it is likely that the mannitol will crystallize out if present in ratios higher than 2:1 w/w mannitol:sucrose [35]. At lower ratios, the crystallization of mannitol may be poisoned and thus prevented. Lower ratios can delay/prevent crystallization but also carry the risk of crystallization occurring over time (which is likely to be a problem) or during thaw (which may be acceptable). Since a crystalline excipient does not provide any protection to protein, it is important to consider the amount of sucrose available in the mixture 953 in relation to the protein concentration. The ability to add sufficient sucrose to protect the protein while also allowing the mannitol to crystallize becomes an issue for high-protein-concentration solutions due to the limited solubility of mannitol (approximately 120 mg/mL). Sorbitol, unlike its isomer mannitol, does not readily crystallize on freezing and instead forms a glass. A damaging consequence of crystallization of excipients during freezing or from the frozen state is the phenomenon of vial breakage. When such a solution is warmed, the concentrated mannitol may crystallize with the available mobility and cause the vial to crack. The primary cause is not the mannitol crystals themselves but the simultaneous crystallization of water that is associated with the amorphous mannitol phase and is released when the mannitol crystallizes. The (sudden) volumetric expansion of water (converting to ice) results in the strain that causes the breakage. The effect is further exacerbated by large fill volumes and is worse in large vials (for same percentage fill volume). Higher concentrations of mannitol increase the risk, as does the rate of processing. The shrinkage caused a sudden separation of the frozen matrix from the wall of the vial resulting in a shock that cracked the vial. Breakage rate was found to increase with increasing protein concentration as well as fill volume. Common parenteral formulation excipients and their generalized behavior at concentrations normally used in drug products are summarized below. Note that the actual behavior of a solute in a solution depends on its concentration and interference. In the case of polymeric excipients, the phase behavior and kinetics are dependent on the molecular weight. These changes occurring simply due to the low temperature ("chill") lead to reversible changes in the protein structure and destabilization called cold denaturation [44,46,47]. Coldinduced unfolding or cold denaturation is a physical consequence of the temperature sensitivity of the non-covalent electrostatic and hydrophobic interactions, which maintain the protein structure, becoming weaker at lower temperatures [44,48,49]. It is a thermodynamic consequence of the large and positive Cp of unfolding of proteins (and which, within experimental error, can be taken to be a constant for a given protein). This equation describes a skewed inverted parabola-shaped protein stability curve over experimentally accessible temperature ranges. Hence, during freezing, the protein structure reacts to a combination of effects-(i) the changing temperature, (ii) the changing solution conditions, and (iii) the changing physical environment, that is, the ice. The impact of (i) changing temperature should be looked upon as the impact of "chill" and is a result of changes in the property of liquid water with temperature. The protein structure reacts to these changes in the solution environment in a manner that is generally reversible and the phenomenon is called "cold denaturation. However, the normal freezing process also results in the removal of water as ice causing (ii) changes in the solution environment. A protein a in solution with 85 mg/mL sucrose will end up with a sucrose concentration of ~800 mg/mL (~80%), that is, a factor of ~10. The high concentration of solutes creates an environment where the protein molecules are exposed to high ionic strengths, possible pH changes, etc. The resulting cryoconcentration and dessication of protein can be classified as an "osmotic stress. Since proteins are attracted to interfaces, the resultant stress on protein structure is called the "ice interfacial stress. It may be readily understood that the overall outcome of freezing on protein structure is not easily deconvoluted into the above three factors, but these factors offer a good framework for developing a product from fundamental principles. The mechanism of protection is likely to be preferential hydration, thus providing indirect proof of the operation of this mechanism even at low temperatures (in the absence of ice). Chill-induced unfolding (denaturation) of a molecule, while potentially reversible in short time frames, would lead to aggregation over longer time frames and thus an increase in aggregation. Hydration is important for maintaining the three-dimensional structure of a protein. The entire hydration shell of the protein is unlikely to be completely removed by freezing: Part of it is unfreezable or bound water, but outer shells or loosely bound water could potentially be lost. These structural changes were prevented with 10% sucrose, which satisfied the hydrogen bonding requirements of the protein. An indirect effect of cryoconcentration can however be seen through the impact on pH of certain buffers. Buffer salts can crystallize if their concentration limit is reached, which changes pH. In practical systems, the actual crystallization of buffer or solution components will be dependent on multiple factors such as concentration, sample size, cooling rate, and presence of other solutes. Nucleation of salt crystals and subsequent precipitation is generally slower than ice crystal growth, leading to formation of supersaturated solutions that may crystallize when some mobility is afforded, possibly during storage at temperatures above Tg. The Tg values of several buffers as a function of pH in the frozen state (sodium tartrate, sodium malate, potassium citrate, and sodium citrate) have been reported by Shalaev et al. It is known that even if the buffer salts do not reach their solubility limits, their pKa value is sensitive to temperature. In general, dissociation constants for carboxylic and inorganic acids have dpKa /dT values close to zero. Proteins that are sensitive to pH-induced changes in conformation or stability will be particularly susceptible to freezing in buffers that are temperature-sensitive. The same changes were not seen with potassium phosphate buffer, whose pH increases slightly on freezing.
Cheap antabuse 250mg with mastercard
Subsequent demonstration that the process consistently operates within the design space reduces the risk medications zoloft generic 500 mg antabuse with amex. In many instances, an appropriate risk management strategy will reduce the risk to an acceptable level where severity and probability may be mitigated by adherence to parameter and attribute boundaries. The acceptability of risk is often a decision that balances the presumed impact of the risk relative to appropriate controls to mitigate that impact. However, if the drug itself is mutagenic and is indicated for firstline therapy for breast cancer, the presence of these impurities should be balanced with the benefit of the drug and its duration of use. If reduction or elimination of genotoxic impurities is cost prohibitive or results in other quality issues, then acceptance of limits for these impurities that exceed the standard regulatory expectation may be justified. Continuous Improvement QbD is by definition a mechanism to develop and improve process understanding and product knowledge. The nature of quality risk management is and should be inherently iterative in that the development of product knowledge and process understanding stimulates regular reassessment to improve mechanistic understanding and potentially control of variability. The characterization of the severity, uncertainty, probability, and detectability of risk through the lifecycle also allows for accommodation of optimizations to support business objectives. The investment in QbD should therefore be construed as the appropriate cost of doing business, prospectively moving toward a paradigm of continual improvement rather than retrospectively reacting to unanticipated variability in the manufacture of products. Specific evaluations and studies are usually inserted/included into the development timeline or lifecycle plan as a complement to or in concerted alignment with other business critical investments. However, QbD can, and perhaps should, be more than a collection of scientific exercises that incrementally improve understanding and may increase opportunities to improve a manufacturing process and reduce costs. In fact, several proponents of QbD have argued that the intrinsic value of QbD is the "full understanding of how product attributes and process variables relate to or influence product performance" [51]. The principles embodied in QbD provide valuable opportunities to increase understanding of how the quality of a pharmaceutical product contributes to patient safety and efficacy. Understanding properties and characteristics of raw materials and components; their relative combination and compatibility with one another; the influence of basic conditions of temperature, pressure, and time; and the operational criteria of manufacturing processes can collectively improve assurance of quality regardless of the product or process to which it is applied. While not all development timelines will permit a comprehensive execution of certain elements of QbD. The adoption and implementation of principles of QbD is a responsible and advantageous approach to managing the lifecycle of pharmaceutical products. Acknowledgments First and foremost, we are indebted to Roger Nosal, Tom Garcia, Vince McCurdy, Carol F. We have borrowed generously from the chapter of the previous edition and left some of the key sections unchanged. The authors appreciate and acknowledge the contributions from many Pfizer colleagues as well as many experts in the field of QbD in the pharmaceutical industry. Pikal who provided valuable input to the lyophilization studies provided in this chapter. In addition, frequent and exhaustive discussions among individuals within the pharmaceutical industry at multiple forums Quality by Design and Control Strategies and conferences have yielded a tremendous wealth of meaningful scientific, technical, and regulatory understanding of QbD. The authors also recognize that the concept of QbD can effectively be applied using several approaches. As a direct result of increased process understanding, Pfizer was able to realize reduced regulatory expectations and expeditious implementation of multiple post-approval changes simultaneously. Draft Guidance for Industry: Comparability protocols- chemistry, manufacturing, and controls information. Guidance for Industry: Demonstration of comparability of human biological products including therapeutic biotechnology-derived products-protein drug products and biological products-chemistry, manufacturing, and controls information. Draft Guidance for Industry: Powder blends and finished dosage units-stratified in-process dosage unit sampling and assessment. Design of Experiments Simplified; Practical Tools for Effective Experimentation, 2nd ed. Response Surface Methodology; Product and Process Optimization Using Designed Experiments, 3rd ed. Experiments with Mixtures (Design, Models and the Analysis of Mixture Data), 2nd ed. Quality by Design for Biopharmaceuticals: Principles and Case Studies, New York: John Wiley & Sons, Inc; 2009. Use of laboratory data in freeze drying process design: heat and mass transfer coefficients and the computer simulation of freeze drying. Fourier-transform infrared spectroscopic investigation of protein stability in the lyophilized form. Evaluation of tunable diode laser absorption spectroscopy for in-process water vapor mass flux measurements during freeze drying. Administration of products by injection parenterally requires that a product be free of infectious microorganisms and essentially free of endotoxin. Concerns regarding microbiological risk are logically heightened when a parenteral product is administered to patients whose health is already compromised, which is a common circumstance in clinical settings. There are two very different manufacturing processes by which product is considered microbiologically safe enough to be labeled sterile. These two methods are commonly known as aseptic processing and terminal sterilization. The selection of the manufacturing method used for the production of sterile products is dependent principally on the physicochemical characteristics of the total product. For a product to be suitable for terminal sterilization, both the product and its delivery system must be functionally unharmed by a method that will achieve sterilization of the product as an integral final dosage form. The use of microbiologically effective sterilization processes on finished formulations in their final container is favored because of their universal antimicrobial effectiveness and the resulting certainty of outcome. However, the potentially deleterious effects of these sterilization processes on the product and/or primary package have limited their application to only about 15% of all products labeled sterile. It follows then that the remaining 85% of all sterile products are manufactured by aseptic processing because that approach to sterile product manufacturing is less physicochemically impactful on both the formulated active pharmaceutical ingredient and the primary packaging which serves as a contamination barrier. The sterilization processes are chosen and applied in a manner that assures the key quality attributes for each of the materials are 829 830 maintained and that the product is therapeutically effective poststerilization. The core aseptic process assembles the sterilized product along with the sterile primary packaging components into the final dosage form in an environment designed and maintained specifically for that purpose. Because the product is not hermetically sealed into its primary package until after the individual sterilization processes are carried out, the potential for contamination during the required transport and handling exists during aseptic processing. The sampling of air, facility and equipment surfaces, as well as of personnel gloves and gowns within the aseptic environment, were instituted with the expectation of gaining information about aseptic process risk. When monitoring was first instituted, aseptic facility contamination control, equipment capability, and gowning materials were markedly less capable than those presently in use. As a consequence, both performance expectations and demonstrated performance were properly non-absolute. It was understood by both practitioners and the regulatory agencies that improvements in contamination control performance were both desirable and attainable and that those improvements would be attained primarily through equipment, engineering, and facilities improvements. The primary focus of these improvements was simply to reduce the impact of human carried and released contamination in the critical areas of aseptic processing. It is not hyperbolic to label dramatic the improvements that have occurred in every aspect in aseptic processing technology over a period of some 50 years of evolution. These enormous improvements have impacted every aspect of aseptic processing and resulted in what can now legitimately be termed advanced aseptic processing, an enhanced means of aseptic operation that is becoming more prevalent. It has proven difficult, however, for standard setting organizations and regulatory authorities to keep up with the revolutionary technical developments in facilities, environment, and machine automation. The understanding of clinical risk arising from aseptically produced products, as well as the understanding of how such risk can be accurately assessed has been outdistanced by the improvements in aseptic processing capability. To best comprehend this circumstance and its implications to the parenteral products industry, we must consider the relationship between safety and the process attribute often called sterility assurance. Parenteral Medications serious matter that can have profound consequences on product costs, market access, drug availability, product liability costs, implementation of new technology, and even the careers of scientists and engineers. A superficial consideration of the concept of sterility might lead one to believe that it is simple to define what sterility is, and therefore, it must be obvious when (or if) a material lacks sterility or sterility assurance. Unfortunately, determining that a material lacks sterility is not straightforward. This determination is largely a judgment call, rather than an absolute assertion that can be made and supported based upon provable scientific fact(s) and empirical data. Central to this problem is the analytical reality that the product release test used to release products regarding the attribute of sterility is both statistically limited and analytically unreliable. Simply stated, microbiological analysis does not allow us to assert that a product is or is not sterile.
Purchase 250mg antabuse amex
In low-risk patients with proctitis treatment shingles order antabuse, mesalamine suppositories 1 g daily may prevent relapse in up to 90% of patients. Oral sulfasalazine or mesalamine is effective in maintaining remission in low-risk patients with more extensive disease. Oral or topical corticosteroids are not effective for maintaining remission and should be avoided due to the high incidence of adverse effects. Systemic corticosteroids and budesonide should be tapered over 60 days in low-risk patients achieving remission. Vedolizumab may be used as an alternate maintenance option if patients had a favorable response to induction therapy and may be combined with azathioprine or methotrexate. L O 5 Patient Encounter 2, Part 1 A 21-year-old African-American woman presents to the gastroenterology clinic because of a 1-month history of crampy abdominal pain and two to three loose stools 3 to 4 days per week. She denies vomiting, fever, or chills, and has missed several days of school and work in the past 2 weeks. What other pertinent information from the history would be beneficial to help determine the cause of her symptoms Response rates of up to 50% are reported, but data are conflicting, and these agents should generally not be considered first-line therapy. For patients with perianal fistulae, antibiotics (metronidazole or ciprofloxacin), infliximab, adalimumab, and certolizumab are appropriate treatment options. Patients should be assessed for possible surgical intervention if abdominal distention, masses, abscess, or obstruction are present. Depending on the outcome this may necessitate a dose increase or a switch to another drug within the class. Ustekinumab is generally reserved for outpatients with severe disease who have failed other traditional therapies. Nutritional support with enteral or parenteral nutrition may be indicated for patients unable to eat for more than 5 to 7 days. Within 2 years, up to 80% of patients experience a relapse; therefore, many patients require indefinite Maintenance of remission of maintenance therapy. Similarly, evaluation of azathioprine metabolites, particularly 6-thioguanine, should be performed to evaluate the need for dose escalation if there is lack of response or in the setting of potential thiopurine toxicity. Unfortunately, up to 50% of patients treated acutely with corticosteroids become dependent on them to prevent symptoms. Such conditions include ischemic colitis, diverticular disease, and microscopic colitis. Corticosteroids may worsen diabetes, hypertension, heart failure, or osteoporosis. What factors should you consider in choosing appropriate therapy for this patient What are some important educational points you would provide to this patient regarding appropriate use of her medication Aggressive nutritional interventions may be required to facilitate adequate caloric intake. Chronic corticosteroid therapy may also be associated with reductions in growth and bone demineralization. Using lower doses in patients who are corticosteroid dependent may reduce altered height velocity. Use of immunosuppressive therapy or infliximab may help reduce overall corticosteroid exposure. Maintenance medications may generally be continued, but certain adjustments may be required. Because pregnancy results in a higher folate requirement, pregnant patients treated with sulfasalazine should be supplemented with folic acid 1 mg orally twice daily. As pregnancy progresses, there is a potential risk of increased placental transfer of biologic drugs. Recommendations are to modify the dosing schedule in the third trimester to allow for the last dose to be given as far in advance of delivery as possible to reduce placental transfer. Prolonged use of metronidazole should be avoided in pregnant patients due to lack of safety data supporting its use. Identify potential barriers to adherence, such as cost or inability to properly use certain drug formulations. Earlier telephone follow-up may be required to determine whether the patient is achieving some relief of symptoms. Educate the patient regarding signs and symptoms of pancreatitis (nausea, vomiting, and abdominal pain). Also monitor patients with a prior history of hepatitis B virus infection for signs of liver disease, such as jaundice. Ulcerative practice guidelines in adults: American College of Gastroenterology, Practice Parameters Committee. Role for intestinal bacteria, viruses, and fungi in pathogenesis of inflammatory bowel diseases and therapeutic approaches. An evidenced based systematic review on medical therapies for inflammatory bowel disease. Advances in use of endoscopy, radiology, and biomarkers to monitor inflammatory bowel diseases. Mechanisms, management, and treatment of fibrosis in patients with inflammatory bowel disease. Nonsteroidal anti-inflammatory drugs and inflammatory bowel disease: current perspectives. Extraintestinal manifestations of inflammatory bowel disease: epidemiology, diagnosis, and management. Lessons learned from trials targeting cytokine pathways in patients with inflammatory bowel disease. Maintaining remission in ulcerative colitis-role of once daily extended-release mesalamine. Glucocorticosteroid therapy in inflammatory bowel disease: systematic review and meta-analysis. Rectal budesonide and mesalamine formulations in active ulcerative proctosigmoiditis: efficacy, tolerance, and treatment approach. American Gastroenterological Association Institute Guideline on the management of Crohns disease after surgical resection. Therapeutic drug monitoring of anti-tumor necrosis factor agents in patients with inflammatory bowel disease. American Gastroenterological Association Institute guideline on therapeutic drug monitoring in inflammatory bowel disease. Management of inflammatory bowel disease in the elderly patient: challenges and opportunities. Drug safety and risk of adverse outcomes for pregnant patients with inflammatory bowel disease. Tumor necrosis factor-alpha antagonists twenty years later: what do Cochrane reviews tell us Antibiotic therapy in inflammatory bowel disease: a systematic review and metaanalysis. Systematic review and meta-analysis of the efficacy and tolerability of nicotine preparations in active ulcerative colitis. Probiotics in the management of inflammatory bowel disease: a systematic review of intervention studies in adult patients. Efficacy of 5-aminosalicylates in ulcerative colitis: systematic review and meta-analysis. Combination therapy with infliximab and azathioprine is superior to monotherapy with either agent in ulcerative colitis. Recommend treatment regimens for nausea and vomiting associated with cancer chemotherapy, surgery, pregnancy, or motion sickness.
