
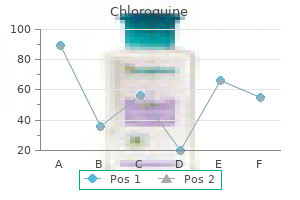
Effective 250 mg chloroquine
It has been hypothesized that a metabolite of ifosfamide inhibits mitochondrial activity and this inhibition could be reversed by methylene blue medicine 44291 purchase 250mg chloroquine with visa, which facilitates electron transfer in the mitochondrial enzymatic respiratory chain. This case represents a dramatic example of the effects of an effective antidote for an acute intoxication affecting the central nervous system. Recognition of a specific intoxication and knowing what antidote to use can be major challenges for any physician. Neurologists are often involved in these cases because intoxications produce neurological signs. Depressed level of consciousness (drowsiness, stupor, or even coma), altered content of consciousness (confusion, delusions, hallucinations), agitation, abnormal movements (myoclonus, asterixis, tremor), ataxia, rigidity, changes in deep tendon reflexes, and seizures can occur in various combinations depending on the type of toxin and the severity of the intoxication. Clues to the toxic nature of the neurological syndrome and even to the specific agent involved can be gathered from the history and the general physical examination. Knowledge of the physical manifestations of common toxidromes- syndromes caused by toxic agents-is therefore helpful to streamline management. Therefore, in intoxicated comatose patients one should keep a low threshold for ordering electroencephalography to exclude nonconvulsive status epilepticus. The treatment of these intoxicated patients depends greatly on the identification of the toxidrome and whether a specific antidote can be tried. Unfortunately, in cases of intentional overdoses, most patients have ingested several drugs instead of a single one. These cases are even more challenging not only in terms of diagnosis (a pure toxidrome is never clearly present) but also in terms of management, because drug interactions may produce additional manifestations and complications. Flumazenil lowers the seizures threshold and should not be used in patients with a history of seizures or at high risk for having them. Naloxone and flumazenil are short-acting, so the improvement of patients may be quite brief. Intubated patients should not be extubated while transiently more alert, as many will lapse again into stupor and become once more unable to protect the airway. One should also be prepared to treat symptoms of acute opiate or benzodiazepine withdrawal when trying these medications. These agents are useful to prove the diagnosis and repeated doses can be used (continuous infusion of naloxone can be used as well), but they do not eliminate the toxin and therefore do not solve the problem. Supportive therapy is needed for severe opiate and benzodiazepine intoxications to resolve. The management of a severe intoxication may be complex and requires a comprehensive game plan. Poor outcome may be due to the initial effects of the toxin or due to secondary complications, such as poor oxygenation and shock. The irony, of course, is that most self-intoxicated patients actually want to recover. Antidotes (such as naloxone, flumazenil) may be administered in appropriate cases. The role of activated charcoal and gastric emptying in gastrointestinal decontamination: a state- of-the-art review. The poisoned patient with altered consciousness: controversies in the use of a "coma cocktail. Drugs of abuse: the highs and lows of altered mental states in the emergency department. Following surgery, the patient was initially agitated and thought to have delirium from withdrawal. Neurology was consulted, and on our examination the patient has a markedly dysarthric speech, limited upgaze, and vertical nystagmus. The total incidence of postoperative coma (24 hours or more) in one very large study of 858,606 patients was very small (0. Complex cardiac or vascular procedures are most often associated with ischemic brain lesions. Ischemic stroke involving major arterial territories is a well-known complication of any type of vascular surgery, such as aortic arch replacement, surgery for aortic dissection, or any type of open-heart surgery. Multiple cases of postoperative stupor associated with bithalamic infarcts have been described. In patients undergoing a general (nonvascular-noncardiac) surgical procedure- as in our case example-neurological complications are not expected. It occurs most often in patients who have other stroke risk factors, such as peripheral vascular disease or ischemic cardiomyopathy. Hypotension does not play a major role unless an unexpected large blood loss has occurred. When ischemic stroke involves the posterior circulation resulting in cerebellar infarcts with obstructive hydrocephalus (explaining stupor), the diagnosis is difficult and often not recognized. Following any type of surgery, there is a tendency for strokes to occur in the posterior circulation territories. Therefore, it has been speculated that these strokes could be due to vertebral dissection occurring as a result of neck manipulation associated with anesthesia preparation. In our patient, the sudden appearance of a bilateral cerebellar infarct compressing the fourth ventricle led to an obstructive hydrocephalus. After ventriculostomy was placed, the patient improved substantially, and eventually the ventriculostomy was weaned and removed. Finally, it is worth emphasizing that the cause of postoperative stupor in general surgical intensive care units usually is due to prolonged clearance of sedative drugs or excessive opioid use. The additional presence of multiorgan failure in critically ill patients may reduce clearance of any of these drugs, and a careful look at the medication dose, infusion rate, and expected clearance is necessary. Reduced renal clearance of sedatives and analgesics is a major determinant of prolonged awakening after cardiac surgery. It can occur more often in patients who have had seizures or in patients who had a known seizure disorder and did not have their antiepileptic drugs administered. Acute metabolic derangement such as acute hyponatremia or acute hypoglycemia is always considered and, occasionally, these derangements explain the clinical picture. In susceptible patients a surgical procedure has led to an acute increase in serum ammonia (mostly young females in teenage years with an ornithine transcarbamylase deficiency or in patients after a lung transplantation). But frankly, the three major causes of failure to awaken slowly postoperatively are drugs, drugs, and drugs. As a general rule, the expected clearance of an opioid or benzodiazepine is usually five times its half-life. Hypoglycemia requires immediate correction, while hyponatremia should be corrected more slowly. Ischemic stroke after surgical procedures: clinical features, neuroimaging, and risk factors. Incidence, predictors and outcomes of postoperative coma: an observational study of 858,606 patients. Predictors of duration of unconsciousness in patients with coma after cardiac surgery. On the second day of surgery he underwent a re-exploration with removal of an extradural hematoma in the posterior fossa and recovered well. A week later, he unexpectedly became gradually more stuporous, developed a new hemiparesis, and was transferred back to the neurosciences intensive care unit. C) the cerebral angiogram (sample of multiple series) shows cerebral vasospasm in the anterior circulation. When neurointensivists are asked by neurosurgeons to become involved in postoperative care, it is because the current clinical condition is unexplained and unusual, seizures have occurred, or a major systemic complication needs very close attention. Complications after craniotomy are uncommon but may be more frequent after extensive and complex neurosurgery. Any patient with an early deterioration may be having seizures, but most patients who are stuporous or comatose from seizures will have already shown focal twitches that then became more generalized and evolved into a nonconvulsive status epilepticus. The cause may not be clear or may simply be related to the mechanical disruption of brain tissue. A more recently identified cause of neurological deterioration is the appearance of a hematoma remote from the surgical site. These hemorrhages are thought to be largely venous in origin and may be located in the opposite hemisphere or in the cerebellum in patients with surgery of cerebral hemispheres or the spine.
Buy generic chloroquine line
Moreover treatment yellow fever safe chloroquine 250mg, few cross-sectional studies carried out to date have related olive consumption and blood pressure. In this latter study, men in the highest category of olive oil intake presented a 50% lower risk of developing hypertension, as compared to those with the lowest intake. In addition, a signi cant inverse trend in the association between olive oil consumption and risk of hypertension in men was observed, which was independent of the consumption of fruits and vegetables. Intervention studies have also reported blood pressure reductions in hypertensive subjects after consumption of virgin olive, regardless the presence of hypercholesterolemia (Perona et al. More recently, supplementation with olive oil rich in phenolic compounds was effective in reducing blood pressure levels in a group of individuals from nonMediterranean countries (Bondia-Pons et al. Although the mechanisms of the hypotensive effect of virgin olive oil are still uncertain, changes have been found in the fatty acid composition of the erythrocyte membrane of women with untreated essential hypertension after the intake of diets rich in virgin olive oil (Ruiz-Gutierrez et al. Virgin olive oil consumption induces signi cant changes of speci c fatty acid moiety Olive Oil in Metabolic Syndrome 2. Analysis adjusted for age, body mass index, energy intake, alcohol consumption, calcium intake, and physical activity during leisure time. Quintile 1 is comprised of individuals with the lowest olive oil intake, whereas quintile ve represents the highest olive oil intake. Likewise, G-protein expression, involved in cell signal transduction and the regulation of blood pressure, is also modulated by changes in membrane lipids (Escriba et al. The reduction in membrane uidity (high cholesterol/phospholipid ratio) has been associated with the development of hypertension (Tsuda et al. Therefore, the effects of virgin olive oil, helping to normalize blood pressure in hypertensive patients, could be originated by the modulation of the interaction of G-proteins and other signal-related proteins, in addition or alternatively to membrane uidity (Perona et al. These normotensive effects have been attributed to minor components present in virgin olive oil, such as -tocopherol, oleuropein, hydroxytyrosol, and tyrosol, all of them with antioxidant and free radical scavenging activities (Tuck and Hayball 2002). These substances could help to revert the imbalance between increased oxidative stress and impaired antioxidant defense that affects endothelial function (Visioli and Galli 1998) and modulate eicosanoid metabolism in endothelial cells (Jialal et al. The reduction of blood pressure by virgin olive oil has also been linked to improvements in the endothelial function. This is what was observed in a randomized trial with 180 participants diagnosed with MetS, after 2 years on a Mediterranean-style diet including virgin olive oil (Esposito et al. In these subjects, blood pressure and platelet aggregation response to -arginine, the natural precursor of nitric oxide, were improved. The mechanism might also be triggered by other minor components like triterpenic acids and alcohols, which are present in low concentrations in virgin olive oil but in relevant content in pomace olive oil. Nevertheless, in these latter studies, the number of participants was lower and the duration of the intervention was shorter. The consequence was an increased release of excess cholesterol from human monocyte-derived macrophages by 44% (Helal et al. Diets with a low glycemic index, that is, those with a low glucose-raising effect, are associated with improvements of glycemic control and insulin sensitivity (Thomas and Elliott 2009). This is even more relevant in obese subjects, who must increase their insulin secretion in order to reestablish glucose homeostasis following a high-glycemic index meal (Sunehag et al. The effect of olive oil minor components on glucose homeostasis and insulin sensitivity has not been extensively addressed. Sitosterol and other plant sterols have been found in lower concentrations in plasma of subjects with impaired fasting glucose compared with normoglycemic subjects (Gylling et al. However, when rats were supplemented with oral -sitosterol, they showed increased fasting insulin level, decreased fasting glucose level, improved oral glucose tolerance, and increased insulin release from isolated rat pancreatic islet cells (Ivorra et al. In vitro, -sitosterol induced glucose uptake and stimulated both adipogenesis and lipolysis in adipocytes. Squalene has been found to correlate with visceral obesity but not with insulin sensitivity in the normoglycemic offspring of patients with type 2 diabetes (Peltola et al. However, in vitro studies have reported that squalene can enhance glucose-stimulated insulin secretion in -cells (Tsuchiya et al. Dietary supplementation with -tocopherol decreased insulin and glucose levels in diet-induced obesity Sprague-Dawley rats (Shen et al. In a group of Swedish volunteers, lower serum -tocopherol concentrations were independently associated with impaired insulin sensitivity and -tocopherol independently predicted type 2 diabetes during 7 years of follow-up. Maslinic and oleanolic acids, potent triterpenic compounds present in relevant concentrations in pomace olive oil, have been related with glucose homeostasis and insulin sensitivity. Both compounds have shown hypoglycemic effects Olive Oil in Metabolic Syndrome 225 by reducing insulin resistance in animal models of type 2 diabetes (de Melo et al. In addition, oleanolic acid may promote insulin signal transduction and inhibit oxidative stress-induced hepatic insulin resistance and gluconeogenesis (Wang et al. There is also some evidence indicating that virgin olive oil phenolics might have also some hypoglycemic effect. Hydroxytyrosol was ef cient to prevent hyperglycemia in alloxan-induced diabetic rats. In these animals, glucose concentration in plasma was decreased by 55% compared to untreated diabetic rats. The reduction was concomitant to an enhancement in the oxidant status and the activity of enzymatic defenses (Hamden et al. Similar results were obtained in the same experimental model by administration of an oleuropein-rich extract (Jemai et al. Some of these factors are also implicated in MetS and recent reports are pointing out to a role of olive oil also in glucose homeostasis, insulin sensitivity, and the other components of MetS. Despite being rich in fat, the Mediterranean diet has not been related with an increase in body weight in epidemiological and intervention studies. However, the mechanisms and actual components of this dietary oil that are responsible for the observed effects are still uncertain. There is a roughly uniform consensus that the high presence of oleic acid in the oil has an important role, but comparative studies with other dietary oils are showing that there must be other factors in uencing the effects of olive oil on health. Several studies are starting to associate minor components of olive oil with some of the observed effects. These components, despite being present in low concentrations in the oil, have potent biological activities as anti-in ammatory, antithrombotic, and antioxidant agents. Nevertheless, the actual cellular and molecular mechanisms by which these components, at the concentrations present in the oil, exert their protective activities are only envisaged. Therefore, there is need of studies at the cellular and molecular level to ascertain the processes involved in these mechanisms in different experimental models. Additionally, a higher level of evidence is needed in order to con rm the results obtained so far and give recommendations of olive oil intake to the population. Very few randomized controlled trials focused on the role of olive oil and MetS have been carried out to date. Still, more large-scale clinical trials are needed, as well as metaanalysis of those studies. Despite all the data supporting the bene cial role of olive oil against cardiovascular disease and MetS, recommendations should be given in the direction of a whole healthy diet including this oil, as there is no suf cient evidence of a protective role of the oil isolated from a healthy dietary pattern, such as the Mediterranean diet. Monounsaturated fatty acids, olive oil and blood pressure: Epidemiological, clinical and experimental studies. Effect of a moderately hypoenergetic Mediterranean diet and exercise program on body cell mass and cardiovascular risk factors in obese women. A comprehensive study of hazelnut oil composition with comparisons to other vegetable oils, particularly olive oil. Accumulation of large very low density lipoprotein in plasma during intravenous infusion of a chylomicron-like triglyceride emulsion re ects competition for a common lipolytic pathway. Carbohydrate and lipid metabolism in patients with noninsulin-dependent diabetes mellitus: Effects of a low-fat, high-carbohydrate diet vs a diet high in monounsaturated fatty acids. Moderate consumption of olive oil by healthy European men reduces systolic blood pressure in non-Mediterranean participants. The lipolysis of chylomicrons derived from different dietary fats by lipoprotein lipase in vitro. Gene regulation in -sitosterol-mediated stimulation of adipogenesis, glucose uptake, and lipid mobilization in rat primary adipocytes. Insulin sensitivity index, acute insulin response, and glucose effectiveness in a population-based sample of 380 young healthy Caucasians. Analysis of the impact of gender, body fat, physical tness, and life-style factors. Lipoprotein cholesterol concentrations in the plasma of human subjects as measured in the fed and fasted states.
Purchase chloroquine 250 mg line
The other limitation is that there is no current consensus regarding the sensitivity of this technique medications that raise blood sugar buy chloroquine 250 mg line, with estimates ranging from 50% to greater than 90%. To date, there has been no evidence of any strains developing antibiotic resistance. Severe disease and disease that fails to respond to oral regimens is usually treated parenterally with ceftriaxone, cefotaxime, or meningeal dose penicillin. The one remaining argument would be to have baseline information should a follow up be necessary. Just as in patients who have been microbiologically cured of bacterial pneumonia, urosepsis, or other major infections, fatigue, malaise, headaches, and other nonspecific systemic symptoms often persist following effective treatment. Logically then, treatment can best be considered to have failed if new symptoms develop, previously present ones worsen, or the original symptoms persist for an inordinate period of time. However numerous studies have consistently failed to demonstrate persistent infection or antibiotic responsiveness in patients with persistent nonspecific symptoms,26,27,41 so in only the first two groups does persistent infection need to be considered. Several studies have suggested that experimentally infected animals might harbor small numbers of viable spirochetes following usually recommended treatment. On the other hand, it is worth considering how persistent bacteria might cause symptoms. Remaining organisms might provoke a persistent immune inflammatory response, with symptoms due to circulating cytokines or other immunomodulators. Alternatively, the bacteria might release an exotoxin, which could circulate and directly or indirectly cause symptoms. In the absence of any plausible mechanism, arguing that bacterial persistence is responsible for persistent symptoms seems difficult to sustain. Although some patients have persistent nonspecific symptoms following treatment, there is no evidence that these are due to persisting infection or respond to additional antibiotics, nor is there evidence to suggest they are due to a neurologic process. Memory impairment and depression in patients with Lyme encephalopathy: Comparison with fibromyalgia and nonpsychotically depressed patients. Immune activation is clearly occurring, with obvious cellular, antibody, and cytokine responses; yet there is no evidence of antibody or other immunomodulator deposition at sites of active inflammation. The former has led to speculation that ongoing nervous system damage could result from induced autoimmunity; yet the rapid resolution of symptoms following antibiotic treatment, and the absence of evidence of ongoing nonspecific immune stimulation in such patients, makes this seem unlikely. Although the classic triad of lymphocytic meningitis, cranial neuritis, and radiculoneuritis represents the most typical presentation, other forms of multifocal inflammation of the peripheral (common) and central (rare) nervous systems do occur. Psychiatric comorbidity and other psychological factors in patients with "chronic Lyme disease". Diagnostic utility of Borrelia burgdorferi cerebrospinal fluid polymerase chain reaction in children with Lyme meningitis. Recommendations for test performance and interpretation from the Second National Conference on Serologic Diagnosis of Lyme Disease. Lyme neuroborreliosis: A new sensitive diagnostic assay for intrathecal synthesis of Borrelia burgdorferi- specific immunoglobulin G, A, and M. The clinical assessment, treatment, and prevention of lyme disease, human granulocytic anaplasmosis, and babesiosis: Clinical practice guidelines by the Infectious Diseases Society of America. Persistence of Borrelia burgdorferi in rhesus macaques following antibiotic treatment of disseminated infection. Viruses associated with congenital or intrauterine infections include cytomegalovirus, herpes simplex virus types 1 and 2, varicella zoster virus, rubella virus, lymphocytic choriomeningitis virus, human immunodeficiency virus and Zika virus. Important viruses associated with perinatal infections include herpes simplex virus types 1 and 2, parechoviruses, and the non-polio enteroviruses. Infections that occur in the immediate perinatal period can also severely damage the immature nervous system; despite effective, well-tolerated antiviral therapy, neonatal herpes simplex virus meningoencephalitis is often associated with permanent neurodevelopmental disability in the surviving infants. The features of these infections include pneumonitis, hepatitis, gastroenteritis, jaundice, and less commonly, meningoencephalitis. The outcome of intrauterine rubella virus infection in susceptible women relates directly to the timing of maternal infection. Except in the remaining endemic regions, postnatal rubella virus infections rarely occur. The latter, known as a cicatrix, consists of scarring and new skin formation corresponding to a dermatomal distribution. By contrast, maternal zoster is not associated with severe fetal or neonatal disease. Later, fever, jaundice, tachypnea, petechiae, vesicular rash, and neurological symptoms or signs such as seizures, somnolence, abnormal tone, or bulbar dysfunction, may appear. Examination of the cerebrospinal fluid can show a mixed or lymphocytic pleocytosis and elevations of the protein content, especially in those infants with signs of meningoencephalitis. The majority of viruses causing congenital or perinatal infections can be detected in various body fluids using traditional cell culture techniques or nucleic acid amplification methods based principally on the polymerase chain reaction (Table 160. These imaging abnormalities range from isolated cerebral calcifications or edema to severe encephaloclastic lesions, such as hydranencephaly or widespread cystic encephalomalacia (Table 160. In general, maternal infections that occur early in gestation are more likely to induce fetal loss or severe neurological sequelae. Infants infected congenitally or perinatally with some of the viruses discussed in this section may benefit from antiviral therapy, as summarized in Table 160. Unfortunately, postnatal antiviral therapy can not reverse the teratogenic or encephaloclasitic abnormalities that occurred in utero as a consequence of fetal viral infection. Several genetic disorders produce abnormalities that can be confused with the systemic or neurological features of congenital viral infections. Aicardi-Goutierres syndrome, also known as the OutcOmE Each of the congenital viral infections described in this section can induce permanent neurodevelopmental sequelae consisting of cerebral palsy, epilepsy, cognitive impairment, and hearing or vision loss. Symptomatic congenital cytomegalovirus infection: neonatal morbidity and mortality. The outcome of congenital cytomegalovirus infection in relation to maternal antibody status. Symptomatic congenital cytomegalovirus infection in infants born to mothers with preexisting immunity to cytomegalovirus. Rubella in pregnancy: intrauterine transmission and perinatal outcome during a Brazilian epidemic. Congenital lymphocytic choriomeningitis virus syndrome: A disease that mimics congenital toxoplasmosis or Cytomegalovirus infection. Lymphocytic choriomeningitis virus infection of the developing brain: Role of host age. Congenital enterovirus 71 infection: A case study with virology and immunochemistry. Neuroradiography findings in the newborn period and the long-term outcome in children with symptomatic congenital cytomegalovirus infection. Early predictors of neurodevelopmental outcome in symptomatic congenital cytomegalovirus infection. Neuropathogenesis of congenital cytomegalovirus infection: Disease mechanisms and prospects for intervention. Toxoplasmosis in the fetus and newborn: update on the prevalence, diagnosis and treatment. Some isolated foci have been also described in Middle East and Australo-Melanesia. An efficient transfer of the virus from an infected cell to a target cell can occur through the formation of a viral synapse and/or by virofilm structure. In healthy carriers the provirus was predominantly integrated in transcriptionally silenced parts of the genome, whereas integration into transcriptionally active units and subsequently increased expression of the provirus predisposed individuals to disease. Both anatomically determined hemodynamic conditions and adhesion molecule-mediated interactions between circulating infected T cells and endothelial cells may contribute to the localization of the main lesions. Age and sex incidence Mostly sporadic and adult, but sometimes familial; occasionally seen in childhood; females predominant B. Chronic spastic paraparesis, which usually progresses slowly, sometimes remains static after initial progression 2.
Generic chloroquine 250mg without prescription
Acute laryngeal dystonia may occur after administration of a phenothiazine or other neuroleptic agents and can result in lifethreatening upper airway obstruction or diaphragmatic spasm treatment 3rd metatarsal stress fracture buy chloroquine 250 mg line. Chorea and athetosis are often overlapping and described as involuntary jerking or writhing movements affecting especially the shoulders, hips, face, and hands. In the intensive care unit setting these typically result from a drug effect, new-onset hyperthyroidism, basal ganglia stroke causing hemichorea, or in patients with lupus or polycythemia vera. Acute hemiballism (flailing, violent, undesired movements of the limbs resulting from a decrease in activity of the subthalamic nucleus of the basal ganglia) is very rare but can result from a stroke or nonketotic hyperglycemia. A lumbar puncture should be performed in any patient with recent onset of psychiatric symptoms, cognitive changes, or fever in conjunction with the movement disorder to rule out autoimmune or infectious encephalitis (Chapter 6). Initial drug therapies for the major acute movement disorder emergencies are listed in Table 26. Hydration, control of the involuntary movements with benzodiazepines and neuromuscular blocking agents if necessary, fever control, and removal of the precipitating drugs are the mainstays of treatment in serotonin syndrome, neuroleptic malignant syndrome, and acute dystonia. The clinical syndrome of our patient was one of sympathetic and serotonergic excess. She had focal seizures, acute encephalopathy, increased sympathetic output including hyperthermia, increased tone in her legs compared with in her arms (classic feature of serotonin syndrome), hyperreflexia, myoclonus, and tremor. Her urine drug screen was positive for amphetamines, methamphetamines, and tetrahydrocannabinol, and we later learned from her friends that she had been experimenting with K2 "spice," a synthetic form of marijuana. She was started on levetiracetam, hydrated, paralyzed, and continued on a midazolam infusion for the first 12 hours to suppress the movements while initiating cyproheptadine. Lorazepam was continued as needed to control the myoclonus over the next 48 hours, and the syndrome fully resolved by the fifth hospital day. As in any other recovered patient with substance abuse, psychiatry was called in for long-term management. Motor symptoms in 100 patients with delirium versus control subjects: comparison of subtyping methods. Serotonin syndrome in the intensive care unit: clinical presentations and precipitating medications. Over the subsequent days the intracranial pressures ranged mostly between 15 and 25 mmHg, requiring occasional doses of 20% mannitol and 10% hypertonic saline to keep it under control. Seven days after the injury she started to exhibit recurrent episodes of sinus tachycardia, tachypnea, hypertension, profuse sweating, and extensor posturing, She was also hyperthermic during the episodes. They are not associated with major episodes of oxygen 193 desaturation, and arterial blood gases do not reveal hypoxia. Blood cultures are negative, and serum lactic acid and creatine kinase levels are normal. Electroencephalogram does not demonstrate epileptiform activity during the spells. When severe, these episodes are associated with transient elevations of intracranial pressure beginning after the onset of the changes in vital signs. Physicians who are unfamiliar with this complication may consider these manifestations a mere epiphenomenon of severe brain injury. Some may even obsessively search for an infectious source or, worse, treat it as seizures with multiple doses of benzodiazepines. These spells, also known as "sympathetic storms," are frequent in patients with severe acute brain injury. They are most common in young patients with diffuse axonal traumatic brain injury, but we have also seen them after severe anoxic-ischemic encephalopathy, large intraparenchymal hemorrhages, subarachnoid hemorrhage, and acute hydrocephalus. Patients become tachycardic, hypertensive (with increased pulse pressure), tachypneic, febrile, and diaphoretic, and often they develop markedly increased muscle tone, which may result in dystonic postures. However, it important to consider other causes of sudden, exaggerated sympathetic response. There are effective therapies for this condition, and there are also drugs that should be avoided as they can exacerbate the problem. This favorable response is not related to the analgesic effect of opiates, but rather to modulation of central pathways responsible for the autonomic dysfunction. In our experience, beta-blockers and clonidine are useful in controlling the tachycardia and hypertension, but less so for the dystonia. Baclofen and benzodiazepines (especially diazepam) do cause muscle relaxation, but they may not improve the other dysautonomic manifestations. We have seen dramatic improvement in the frequency and severity of spells within days of starting gabapentin, which has become our first choice for the longerterm control of this disorder. Antidopaminergic drugs, such as haloperidol, and other sympathomimetics need to be avoided (Table 27. Choosing the right medication to treat the spells is not enough, and other aspects of management are equally important. These patients sweat profusely, and fluid intake should be adjusted to compensate for this marked increase in insensible losses and to prevent volume contraction. Fever must be aggressively treated with cooling measures, as it has a negative impact on the acutely injured brain. The manifestations excessively increase the metabolic demand, risk increase in intracranial pressure, and may cause long-term complications. Because it is a relatively common and treatable complication in comatose patients, physicians need to be aware of it and start effective therapy. When the clinical signs are not characteristic, consider pulmonary embolism, early sepsis, and seizures. A critical review of the pathophysiology of dysautonomia following traumatic brain injury. Gabapentin in the management of dysautonomia following severe traumatic brain injury: a case series. Paroxysmal sympathetic hyperactivity after acquired brain injury: consensus on conceptual definition, nomenclature, and diagnostic criteria. Cerebral angiogram showed an anterior communicating artery aneurysm, which was successfully coiled. His condition improved after placement of a ventriculostomy catheter, but shortly thereafter his level and content of consciousness started to fluctuate because of alcohol withdrawal. Despite treatment with benzodiazepines and dexmedetomidine, he had frequent episodes of agitation, diaphoresis, hyperthermia, and tachycardia. Serial transcranial Doppler measurements showed progressively increasing mean blood flow velocities in the anterior and middle cerebral arteries bilaterally starting on post bleeding day 6. The implication is important: the threshold for suspecting early severe sepsis should be very low. Delays can be problematic, even more so in patients with possible compromise of cerebral perfusion. The general principles of management of septic shock apply to patients with acute brain injury. However, in critically ill neurological patients, certain aspects of care may have to be adjusted (Box 28. In patients with cerebral edema normal saline is preferable to lactated Ringer to avoid fluids with lower tonicity. The usual set target in the treatment of sepsis is a mean arterial pressure of 65 mmHg, but a higher target may be necessary in patients at risk of cerebral ischemia. Serum lactate should be measured quickly and it is an important indicator of the seriousness of the situation. Goaldirected therapy protocols within the first 6 hours (aiming for a central venous oxygen saturation 70%) do not provide added benefit as long as adequate support is otherwise provided, and these protocols may result in overtreatment. However, the pure alpha-adrenergic agonist phenylephrine is not a good choice in septic shock because it can reduce cardiac output by increasing afterload without providing inotropic support and, even more, patients with sepsis may already have myocardial dysfunction. If the left ventricular ejection fraction is reduced and shock persists, dobutamine-an inotropic agent-should be started. After the patient has been successfully resuscitated, fluid administration must be very conservative. However, this approach can create a dilemma in certain acute neurological disorders. In patients with brain edema, maintaining a negative fluid balance is actually preferred. On the contrary, patients with symptomatic cerebral vasospasm can become ischemic if they develop intravascular volume contraction.
Cheap chloroquine 250 mg overnight delivery
However medicine 3605 discount chloroquine 250 mg overnight delivery, recent studies are pointing out that in Mediterranean countries, restricted energy diets that were relatively high in fat from olive oil may be more effective than the traditional low-fat diet for weight loss in obese persons (Schroder et al. The Mediterranean patterns show better palatability and compliance, which helps to maintain the weight loss (Shai et al. Olive oil consumption was associated with nonsigni cant lower likelihood of weight gain in a large Mediterranean cohort of 7368 individuals, who were followed for a median period of 28. Therefore, the investigators suggested that promoting eating habits consistent with the traditional Mediterranean patterns may be useful to combat obesity (Mendez et al. In this regard, recent experimental evidence suggests that mobilization of intestinally derived oleoylethanolamide, a lipid messenger of satiety, is enabled by the uptake of dietary oleic acid (Schwartz et al. The statement also indicates that knowledge of the metabolic pathways of triglyceride-rich particles and the consequences of hypertriglyceridemia are crucial in understanding the characteristic lipid alterations in diabetes mellitus. Consumption of the olive oil with the highest phenolic content led to increased concentrations of oleic and palmitic acids, as well as decreased content of linoleic acid, in these lipoproteins. Olive oil minor components can also have a role on the fate of plasma triglycerides. Most studies evaluating the association between diet and risk of hypertension have been conducted in the United States and northern Europe, regions with speci c dietary patterns. For that reason, the role of foods less represented in these populations in the prevention of hypertension, such as olive oil, has not been adequately addressed. Only a few controlled experiments in small groups of individuals and a clinical trial have been conducted and suggest that consumption of olive oil could reduce the need for antihypertensive medications on hypertensives (Alonso et al. The effect of polyphenols in olive oil on heart disease risk factors: A randomized trial. Oleanolic acid, a natural triterpenoid improves blood glucose tolerance in normal mice and ameliorates visceral obesity in mice fed a high-fat diet. Dietary patterns, insulin resistance, and prevalence of the metabolic syndrome in women. Mediterranean and low-fat diets improve endothelial function in hypercholesterolemic men. Comparison of a high-carbohydrate diet with a high-monounsaturated-fat diet in patients with non-insulin-dependent diabetes mellitus. Differential utilization of saturated palmitate and unsaturated oleate: Evidence from cultured myotubes. Squalene in a sex-dependent manner modulates atherosclerotic lesion which correlates with hepatic fat content in apoE-knockout male mice. Differences in hydrocarbons of virgin olive oils obtained from several olive varieties. Hypoglycemic and antioxidant effects of phenolic extracts and puri ed hydroxytyrosol from olive mill waste in vitro and in rats. Effect of beta-sitosterol-3-beta- -glucoside on insulin secretion in vivo in diabetic rats and in vitro in isolated rat islets of Langerhans. Measurement of apolipoprotein B-48 in the Svedberg otation rate (S(f))>400, S(f) 60-400 and S(f) 20-60 lipoprotein fractions reveals novel ndings with respect to the effects of dietary fatty acids on triacylglycerol-rich lipoproteins in postmenopausal women. Antidiabetic and antioxidant effects of hydroxytyrosol and oleuropein from olive leaves in alloxan-diabetic rats. Saturated, but not n-6 polyunsaturated, fatty acids induce insulin resistance: Role of intramuscular accumulation of lipid metabolites. Distinctive postprandial modulation of beta cell function and insulin sensitivity by dietary fats: Mono-unsaturated compared with saturated fatty acids. Differential in uence of different dietary fatty acids on very low-density lipoprotein secretion when delivered to hepatocytes in chylomicron remnants. Dietary intake and the development of the metabolic syndrome: the Atherosclerosis Risk in Communities study. Effects of minor constituents (nonglyceride compounds) of virgin olive oil on plasma lipid concentrations in male Wistar rats. Membrane structure modulation, protein kinase C alpha activation, and anticancer activity of minerval. Comparison of the effects of saturated, monounsaturated and polyunsaturated fatty acids on plasma lipids and lipoproteins in man. Inhibition of circulating immune cell activation: A molecular antiin ammatory effect of the Mediterranean diet. Adherence to a Mediterranean diet is associated with reduced 3-year incidence of obesity. Mediterranean diet, but not red wine, is associated with bene cial changes in primary haemostasis. American Heart Association Clinical Lipidology, Thrombosis, and Prevention Committee of the Council on Nutrition, Physical Activity, and Metabolism; Council on Arteriosclerosis, Thrombosis and Vascular Biology; Council on Cardiovascular Nursing; Council on the Kidney in Cardiovascular Disease. Triglycerides and cardiovascular disease: A scienti c statement from the American Heart Association. Erythrocyte membrane cholesterol distribution in patients with untreated essential hypertension: Correlation with sodium-lithium countertransport. Effect of age on plasma embrane asymmetry and membrane uidity in human leukocytes and platelets. Phenolic compounds and squalene in olive oils: the concentration and antioxidant potential of total phenols, simple phenols, secoroids, lignans and squalene. High-monounsaturated-fat/low-carbohydrate diet improves peripheral insulin sensitivity in non-insulin- dependent diabetic patients. Relationship of dietary saturated fatty acids and body habitus to serum insulin concentrations: the Normative Aging Study. Quantitative determination of hydroxyl pentacyclic triterpene acids in vegetable oils. A Mediterranean and a high-carbohydrate diet improve glucose metabolism in healthy young persons. Consumption of diets with different type of fat in uences triacylglycerols-rich lipoproteins particle number and size during the postprandial state. Uptake of triacylglycerol-rich lipoproteins of differing triacylglycerol molecular species and unsaponi able content by liver cells. Differential modulation of hepatic very lowdensity lipoprotein secretion by triacylglycerol-rich lipoproteins derived from different oleic-acid rich dietary oils. Dietary virgin olive oil triacylglycerols as an independent determinant of very low-density lipoprotein composition. Olive oil phenols modulate the triacylglycerol molecular species of human very low-density lipoprotein. The unsaponi able fraction of virgin olive oil in chylomicrons from men improves the balance between vasoprotective and prothrombotic factors released by endothelial cells. Triacylglycerol molecular species are depleted to different extents in the myocardium of spontaneously hypertensive rats fed two oleic acid-rich oils. Consumption of virgin olive oil in uences membrane lipid composition and regulates intracellular signaling in elderly adults with type 2 diabetes mellitus. Antiatherogenicity of extra virgin olive oil and its enrichment with green tea polyphenols in the atherosclerotic apolipoprotein-E-de cient mice: Enhanced macrophage cholesterol ef ux. Plasma lipids, erythrocyte membrane lipids and blood pressure of hypertensive women after ingestion of dietary oleic acid from two different sources. Diabetes and the Mediterranean diet: A bene cial effect of oleic acid on insulin sensitivity, adipocyte glucose transport and endothelium-dependent vasoreactivity. The diet rich in monounsaturated fat modi es in a bene cial way carbohydrate metabolism and arterial pressure. Relationships between the responses of triglyceriderich lipoproteins in blood plasma containing apolipoproteins B-48 and B-100 to a fat-containing meal in normolipidemic humans. Adherence to the traditional Mediterranean Diet is inversely associated with body mass index and obesity in a Spanish population. Effect of vitamin E supplementation on oxidative stress in a rat model of diet-induced obesity. Randomized trial on the effects of a 7-d low-glycemic diet and exercise intervention on insulin resistance in older obese humans. Cardiovascular, antihyperlipidemic and antioxidant effects of oleanolic and ursolic acids in experimental hypertension. Oleic acid from cooking oils is associated with lower insulin resistance in the general population (Pizarra study). Identi cation and quantitation of major carotenoids in selected components of the Mediterranean diet: Green leafy vegetables and olive oil.
Purchase chloroquine 250 mg otc
Yet treatment hiccups chloroquine 250 mg without prescription, when fever is accompanied by hypotension, patients should be rapidly treated for early sepsis following a comprehensive protocol. Society of Critical Care Medicine Consensus Conference: definitions for sepsis and organ failure and guidelines for the use of innovative therapies in sepsis. Surviving Sepsis Campaign: international guidelines for management of severe sepsis and septic shock. Effect of erythropoietin and transfusion threshold on neurological recovery after traumatic brain injury: a randomized clinical trial. According to the first responders he was dazed before he was brought by helicopter to our emergency department. His neurological examination was completely normal, and he could clearly describe the sequence of events before and after the accident. He asked for opioids frequently to control his pain but remained alert and oriented. Three days after the operation, he suddenly developed respiratory distress and very shortly thereafter he became comatose with irregular breathing. His neurological examination revealed small reactive pupils, intact corneal reflexes, but extensor motor responses. You are asked for an opinion on his neurological examination and whether this represents "neurogenic" pulmonary edema. In the acute setting, several disorders should be considered, including pulmonary contusion, aspiration pneumonitis, and the much less common neurogenic pulmonary edema. Pulmonary emboli are usually seen after a considerable time interval, but they may occur after only a few days of immobilization in predisposed patients. A pulmonary embolus should always be considered after neurosurgical procedures, in patients on prolonged bed rest, and in patients with hemiplegia in whom the paralyzed leg is particularly at risk of developing deep venous thrombosis. Acute respiratory distress in a mechanically ventilated patient may have multiple other causes, including acute main bronchus obstruction, inappropriate ventilator settings, pneumothorax, atelectasis, or dislodgement of the tracheostomy tube. Flash pulmonary edema is usually a result of increased sympathetic activation due to an acute medulla oblongata lesion or to a rapidly increased intracranial pressure. Pulmonary arterial constriction leads to shunting to other areas that cannot handle pressure, resulting in capillary leak and edema. It can also be seen as a secondary phenomenon of severe stress-induced cardiomyopathy (takotsubo cardiomyopathy). In these patients, there is significant apical ballooning from a major sympathetic outburst associated with acute brain injury, in turn resulting in severe pulmonary edema. Vasodilators and diuretics may be used to relieve pulmonary congestion and reduce ventricular preload. Stress-induced cardiomyopathy may require specific treatment to improve ventricular contractility. Acute coma and respiratory distress in a patient with a recent femur fracture are sufficient clues to arrive at the diagnosis. In practice, this entity is not always so easily recognized, and reports are infrequently published. Furthermore, the diagnosis is difficult to prove; the "textbook" truncal and axillary petechiae may disappear quickly, and fat in bronchial secretions suctioned out by bronchoscopy and fat globules in urine may not be found (identification of fat globules requires a special stain such as Sudan red, which is often not readily available). Fat embolization syndrome is rare but can be recognized usually about 48 hours after trauma. Ventilation should maintain plateau pressure <30 cm of water and low tidal volumes (6 mL/kg of ideal body weight) to prevent volutrauma. Patients may remain comatose for weeks but then may slowly awaken and go on to recover. Often these lesions have been incorrectly interpreted as an indicator of poor outcome. This case taught us that fat emboli to the brain resulting in coma may have a good outcome against all odds-even in situations with persistent extensor motor responses for weeks and episodes of paroxysmal hyperactivity. Of course, these conditions are not common and we should expect more mundane causes in a trauma patient who develops sudden respiratory distress. Patients with decreased level of consciousness and a weak cough often develop pooling of oral and respiratory secretions which may lead to bronchial obstruction. The differences between pulmonary complications in acute brain injury are shown in Table 29. Neurogenic pulmonary edema due to traumatic brain injury: evidence of cardiac dysfunction. Fat embolism in pediatric patients: an autopsy evaluation of incidence and etiology. Pearls & oysters: good recovery following cerebral fat embolization with paroxysmal hyperactivity syndrome. The patient is potentially a candidate for intravenous thrombolysis, but after these two doses of labetalol, the blood pressure is increasing to 194/106 mmHg. There are no other clinical or laboratory contraindications for intravenous thrombolysis. All recommendations mentioned here on blood pressure management are based on collective experience of experts in the field, but unfortunately, very few clinical trials have evaluated this matter. Expert guidelines recommend reducing the systolic blood pressure below 185 mmHg and the diastolic blood pressure below 110 mmHg before infusing the thrombolytic. If these Acute stroke and hypertension Ischemic Intracerebral hemorrhage Subarachnoid hemorrhage Candidate for thrombolysis If suspected increased intracranial pressure, then monitor intracranial pressure and maintain cerebral perfusion pressure >60 mmHg. Some clinicians apply the same principle to endovascular recanalization therapies (mechanical clot retrieval or suctioning, intracranial stent placement), though this has not been well studied. The rationale for deferring any type of acute recanalization therapies in patients with severe uncontrolled hypertension is that the risk of reperfusion hemorrhage is likely too high. Failure to control hypertension during this first day could result in a reperfusion hematoma with mass effect and rapid neurological deterioration. Therefore, when the patient is not a candidate for acute recanalization therapy, the prevailing thought is that it is better not to lower the blood pressure unless it is exceedingly high (above 220/120 mmHg). The concept of accepting high blood pressures ("permissive hypertension") is based on the notion that lowering the blood pressure in these patients with persistent vessel occlusion could worsen the brain ischemia by reducing collateral flow. When allowing blood pressure to remain high, it is important to monitor patients for possible signs of congestive heart failure, acute kidney injury, and other complications of acute hypertension. That said, gradual and modest blood pressure reduction (by 10 or 15 mmHg) is probably safe, and studies are investigating whether this approach can be beneficial. If the blood pressure control is not optimal upon discharge, we arrange for very close follow-up as an outpatient until the goal of blood pressure normalization is reached. Aggressive antihypertensive treatment to achieve this goal was safe and it was associated with some improved functional outcomes. However, hematoma expansion was not significantly different in patients treated to keep systolic blood pressures <140 mmHg as compared to <180 mmHg. Consequently, the mechanism whereby aggressive blood pressure lowering resulted in slightly better outcomes is not clear. It is also important to note that the benefit was more pronounced in patients without a history of pre-existent hypertension. Ongoing trials may further clarify the ideal blood pressure target after acute intracerebral hemorrhage. We reduce the blood pressure of patients with intracerebral hemorrhage as soon as the diagnosis is made, but try to do so gradually to avoid compromising cerebral perfusion. If intracranial pressure is monitored-rarely the case in clinical practice and then often obtaining data from a ventriculostomy-the cerebral perfusion pressure should be maintained above 60 mmHg. Most patients with aneurysmal subarachnoid hemorrhage have elevated blood pressures due to the excessive sympathetic release that immediately follows the aneurysm rupture. Moreover, in these patients intracranial hypertension is common, and most patients with an abnormal level of consciousness will need a ventriculostomy. When intracranial pressure is known, the cerebral perfusion pressure should be kept above 60 mmHg. Once the aneurysm is treated by means of clipping or endovascular coiling, we stop antihypertensives except for nimodipine (and low-dose beta-blocker in patients who were previously on beta-blockers), anticipating the need to maintain adequate cerebral perfusion in a narrowed arterial bed from vasospasm. If intermittent doses of these medications fail to control the hypertension, we place an arterial catheter and start an infusion of nicardipine (or sometimes labetalol).
Chloroquine 250 mg low price
A prospective study to assess the relation between long-term coffee and decaffeinated ltered coffee consumption and markers of in ammation and endothelial dysfunction treatment using drugs is called order chloroquine 250 mg online. Adiponectin, a plasma protein derived from adipose tissue, has several bene cial effects on human health, such as antiatherogenic effects on vascular cells and antidiabetic properties. Although type 2 diabetes is a complication and not a risk factor for MetS, studies regarding the relationship between coffee daily intake and T2D were included in the summary table, since abnormal glucose homeostasis is a major risk factor for T2D (Table 22. Results from various studies regarding blood pressure were not consistent, and recent studies have reported a protective effect against T2D, a strong risk factor for cardiovascular disease, raising the interest again to study the effects of caffeine on the cardiovascular system. Additionally, coffee has other components, such as potassium, magnesium, and chlorogenic acid, that may protect the cardiovascular system (Noordzij et al. Moderate consumption of caffeinated and decaffeinated coffee may lower the risk of T2D in younger and middle-aged women. Conclusion Negative relationship between diabetes risk and consumption of ground coffee and regular tea observed for all nonelderly subjects, who had previously lost weight. Coffee consumption was associated with a substantially lower risk of clinical T2D. Studies found that boiled coffee increased the concentration of cholesterol levels in humans (Thelle et al. Most studies associating coffee with obesity, glucose homeostasis, and in ammatory/oxidative stress markers had either no effect or positive effects on human health. The T2D-protective potential of coffee seems promising and needs to be further studied considering that the rate of diabetes is growing rapidly worldwide. A 3-month single-blind (investigator), three-stage clinical trial to investigate the effects of daily coffee consumption on biomarkers of coffee intake, subclinical in ammation, oxidative stress, glucose, and lipid metabolism A prospective, controlled study to assess the effects of the intake and abstention of ltered brewed coffee on blood lipids A prospective intervention study to assess the effects of ltered coffee consumption on the concentrations of total homocysteine and total cholesterol A randomized controlled trial to determine the effect of ltered coffee consumption on plasma lipoprotein cholesterol levels in healthy men A randomized controlled trial to study caffeinated and decaffeinated coffee effects on plasma lipoprotein cholesterol, apolipoproteins, and lipase activity. Abstaining from even commonly consumed amounts of ltered coffee may lower the concentrations of both total homocysteine and total cholesterol. Although studies have suggested that the cholesterol-raising component, cafestol, does not pass the paper lter, and hydroxyhydroquinonefree coffee may even have a hypotensive effect, those results must be con rmed in other studies. More studies are needed to evaluate the effects of coffee on the components of the MetS. The studies should ideally specify the coffee genotype, brewing, and degree of roasting as well as the concentration of the major components involved in the health effect since these components seem to in uence the health outcomes. Caffeine and coffee: Their in uence on metabolic rate and substrate utilization in normal weight and obese individuals. The glucose intolerance induced by caffeinated coffee ingestion is less pronounced than that due to alkaloid caffeine in men. An oral lipid challenge and acute intake of caffeinated coffee additively decrease glucose tolerance in healthy men. Weight gain in older adolescent females: the internet, sleep, coffee, and alcohol. Effects of caffeine on energy metabolism, heart rate, and ethylxanthine metabolism in lean and obese women. Association of lifestyle and personality characteristics with blood pressure and hypertension: A cross-sectional study in the elderly. Cafestol and kahweol, two coffee speci c diterpenes with anticarcinogenic activity. Abstention from ltered coffee reduces the concentrations of plasma homocysteine and serum cholesterol-A randomized controlled trial. Glucose homeostasis remains altered by acute caffeine ingestion following 2 weeks of daily caffeine consumption in previously non-caffeineconsuming males. Coffee consumption is not related to the metabolic syndrome at the age of 36 years: the Amsterdam Growth and Health Longitudinal Study. Normal caffeine consumption: In uence on thermogenesis and daily energy expenditure in lean and postobese human volunteers. Caffeinated coffee does not acutely effect energy intake, appetite, or in ammation but prevents serum cortisol concentrations from falling in healthy men. Caffeine ingestion decreases glucose disposal during a hyperinsulinemic-euglycemic clamp in sedentary humans. Habitual coffee but not green tea consumption is inversely associated with metabolic syndrome: An epidemiological study in a general Japanese population. Coffee, decaffeinated coffee, and tea consumption in relation to incident type 2 diabetes mellitus a systematic review with meta-analysis. The effect of chronic coffee drinking on blood pressure: a meta-analysis of controlled clinical trials. Coffee consumption and serum lipids: A meta-analysis of randomized controlled clinical trials. Effects of coffee consumption on subclinical in ammation and other risk factors for type 2 diabetes: A clinical trial. Relation to age, sex, weight, height, diabetes, serum lipids and consumption of coffee, tobacco and alcohol. Antihypertensive effect of green coffee bean extract on mildly hypertensive subjects. Caffeine, trigonelline, chlorogenic acids and sucrose diversity in wild Coffea arabica L. Impact of dairy products on biomarkers of in ammation: A systematic review of randomized controlled nutritional intervention studies in overweight and obese adults. Caffeine increases ambulatory glucose and postprandial responses in coffee drinkers with type 2 diabetes. Caffeine ingestion is associated with reductions in glucose uptake independent of obesity and type 2 diabetes before and after exercise training. Coffee in human health: A discussion on the substances present in beverages related to cardiovascular diseases (in Portuguese). Coffee consumption and markers of in ammation and endothelial dysfunction in health and diabetic women. The Relationship of Coffee Consumption with Total and Disease-Speci c Mortality: A Cohort Study. Nutrition and blood pressure among elderly men and women (Dutch Nutrition Surveillance System). Homeostasis model assessment: Insulin resistance and beta-cell function from fasting plasma glucose and insulin concentrations in man. Total polyphenol excretion and blood pressure in subjects at high cardiovascular risk. Blood pressure response to chronic intake of coffee and caffeine: A meta-analysis of randomized controlled trials. Metabolic effects of caffeine ingestion and physical work in 75-year old citizens. Effects of hydroxyhydroquinone-reduced coffee on vasoreactivity and blood pressure. Coffee consumption and risk of type 2 diabetes mellitus: An 11-year prospective study of 28 812 postmenopausal women. Caffeine ingestion increases the insulin response to an oral-glucose-tolerance test in obese men before and after weight loss. Combined effects of coffee consumption and serum -glutamyltransferase on serum C-reactive protein in middle-aged and elderly Japanese men and women. Coffee and tea consumption in relation to in ammation and basal glucose metabolism in a multi-ethnic Asian population: A cross-sectional study. Comparison of C-reactive protein and lowdensity lipoprotein cholesterol levels in the prediction of rst cardiovascular events. A 4-week consumption of medium roast and dark roast coffees affects parameters of energy status in healthy subjects. Caffeine ingestion before an oral glucose tolerance test impairs blood glucose management in men with type 2 diabetes. Caffeinated and decaffeinated coffee effects on plasma lipoprotein cholesterol, apolipoproteins, and lipase activity: A controlled, randomized trial.
Buy chloroquine 250mg overnight delivery
Inhibition of cholesterol biosynthesis impairs insulin secretion and voltage-gated calcium channel function in pancreatic -cells medicine man lyrics generic 250 mg chloroquine amex. Identi cation and classi cation of olive oils by high-resolution c-13 nuclear-magnetic-resonance. The excessive accumulation of adipose tissue in obesity may be caused by endocrine, metabolic, or genetic changes, or by changes in energy expenditure factors due to reduced physical activity and increased food intake (Ali et al. Adipocytes in greater number and volume in obesity have functional aspects in metabolism and energy homeostasis (Rayalam et al. The central adiposity induces chronic systemic in ammation by increasing the concentration of in ammatory markers, which may be a risk for the onset of metabolic syndrome (MetS) (Duarte et al. Increased blood cholesterol content and oxidative modications of low-density lipoproteins (Nwose et al. Soybeans exert antioxidant effects when people consume soy foods (Bertipaglia et al. MetS is an independent predictor of cardiovascular morbidity and mortality (Ford et al. Abdominal obesity and insulin resistance are the core features of MetS (Reaven 1988). Several dietary patterns and dietary components have been studied to evaluate their in uence on MetS parameters. Therefore, it has been shown that there are nutritional alternatives, which can improve many factors related to MetS. Most studies, which evaluated the effect of soy intake, have been performed on healthy people, hypercholesterolemic, or diabetic patients (Hall et al. Several studies suggest that soy protein and its phytoestrogens (iso avones) may have bene cial effects in obesity and correlated dysfunctions. Soy phytoestrogens have numerous physiological activities, particularly in lipid metabolism, playing an important role in hypercholesterolemic and hyperlipidemic patients (Bhathena et al. In addition, reduction in fat mass can occur through lipolysis and loss of mature fat cells via apoptosis (Rayalam et al. This chapter will report the main biological effects of soy, soy-based products, and soy components, and their effects on MetS indicators. Researchers are interested in both the nutritional value and the potential health bene ts of soybeans. This research includes a wide range of areas, such as cancer, coronary heart disease (cardiovascular disease), osteoporosis, cognitive function (memory related), menopausal symptoms, renal function, and many others. Remarkably, seeds of soy contain very high levels of protein, carbohydrate conjugates, fatty acids (soybean oil), amino acids, and inorganic materials (minerals). Among these soybean components, protein and fatty acid content account for about 40% and 20%, respectively. Some molecules with biological effects are the iso avones, phytic acid, soy lipids, soy phytoalexins, soy saponins, lectins, hemagglutinin, soy toxins, and vitamins (Table 14. Food and Drug Administration recognized soy protein functionality in 1999 (Department of Health and Human Services 1999). It was stated that "diets with low content in saturated fat and cholesterol and that include 25 g soy protein can reduce cardiovascular risk. The American Heart Association recommends the ingestion of soybeans and soy-based products to patients with high cholesterol levels. In Federal Programs of School Feeding, it was reported that soybeans could substitute animal protein until 30% without any prejudice (Messina et al. Brazil is one of the main soybean producers of the world (The American Soybean Association 2014). Lecithin has been a popular supplement because of its high choline (N,N,Ntrimethylethanol) content. Choline is an essential nutrient that has bene t for heart health and brain development, as choline de ciency plays a role in liver disease, atherosclerosis, and possibly neurological disorders (Kunnen and Van Eck 2012). Soya-cerebroside was reported to exhibit moderate tyrosinase inhibitory activity and applied for making skin-care cosmetics for the removal of (black) freckles. In humans, sphingomyelin represents ~85% of all sphingolipids in the membranous myelin sheath that surrounds some nerve cell axons (Fuller 2010). Phytoalexins are known to inhibit bacterial or fungus cell wall biosynthesis, or delay maturation, or disrupt metabolism. Coumestrol was reported to inhibit the enzymes involved in the biosynthesis of steroid hormone (aromatase and hydroxysteroid dehydrogenase), and inhibition of these enzymes results in the modulation of hormone production. Cancer cells have more cholesterol-type compounds in their membranes than normal cells. Soy saponins can bind cholesterol in vitro and thus interfere with cell growth and division (Mac Donald et al. They typically agglutinate certain animal cells and/or precipitate glycoconjugates. Nutritional Intervention in Metabolic Syndrome Source: Adapted from Parh, 2001 and Carter, T. However, the mechanisms whereby soy protein may exert its bene cial effects on obesity are not completely clear. Several lines of evidence suggest that soy protein may favorably affect lipid absorption, insulin resistance, fatty acid metabolism, and other hormonal, cellular, or molecular changes associated with adiposity. Soy-based products, due to their high contents of protein and ber, may have bene cial effects on satiety (Allison et al. They may even produce weight loss with a decrease in fat mass but not muscle mass in overweight and obese subjects (Deibert et al. The consumption of soybean or its bioactive compounds has been reported to contribute signi cantly to reducing cholesterol and triglyceride levels in laboratory animals and humans (Reynolds et al. Hypocholesterolemic effect has been found in peptide Leu-Pro-Tyr-Pro-Arg, a protein fragment derived from soybean glycinin, which reduced serum cholesterol in mice (-25. Although both have hypocholesterolemic activities, enterostatin did not increase fecal excretion of bile acids, suggesting that they may act by different mechanisms (Takenaka et al. It is known that phytate exerts an effect on hepatic glucose-regulating enzyme activities and reduces the risk of high-fat diet-induced hyperglycemia (Kim et al. The hypocholesterolemic effect of soy consumption may be attributed not only to the presence of bioactive Soy and Soy-Based Products 239 compounds (intrinsic effect) but also to replacing animal foods rich in saturated fat and cholesterol (extrinsic effect). A recent study estimated the intrinsic and extrinsic effects of soybean to reduce cholesterol and veri ed that the combined effects are important to reduce cholesterol in approximately 4% (Jenkins et al. In fact, the synergistic action of amino acids and iso avones in improving lipid metabolism has been demonstrated (Bertipaglia et al. On the other side, a study performed with a group of postmenopausal women found no signi cant hypocholesterolemic effect of ingesting soymilk for 4 weeks, despite good adherence of the participants (Beavers et al. The authors discussed that the baseline cholesterol status, supplement type, dosage, and duration, as well as dietary control, are all potential confounding factors, and they have been identi ed as determinants of the con icting results. In contrast, a study performed with MetS women using 35 g/day of textured soy protein (obtained by manufacturing; in this process, 95% of its fat is extracted, with a reduction in many of its nutrients) or soy nut for 12 weeks showed an improvement in lipid pro le, mainly in the group of patients that ingested soy nut (Bakhtiary et al. The aforementioned data allow suggesting that ingestion of soy or soy products seems to offer more bene ts to MetS patients when compared to soy-isolated component. In the literature, improvement in lipid pro le is usually reached with soy ingestion above 50 g/day. Therefore, soy is a robust candidate to reproduce, in a weaker way, the characteristic of statins (Pak et al. Although the bene cial effects of soy and soy-based products are undisputed, some components, such as iso avones, deserve special attention. The effect of iso avones in reducing blood glucose may be explained by the stimulus by genistein to pancreatic cells, which increases insulin production and consequently the glucose uptake by cells (Esteves et al. These effects has been demonstrated in studies with animals that received genistein (Jonas et al.
