
Purchase 5 mg clarinex mastercard
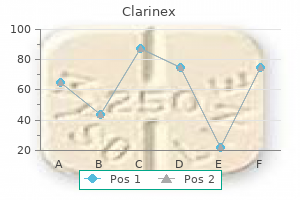
In recent years allergy shots vs xolair buy 5mg clarinex amex, new psychoactive substances have been introduced via internet sites. Whereas most of these are psychostimulants or hallucinogenic, a few may be opioid agonists. In recent years, fentanyl analogues have been produced on a large scale and many of these can be purchased as nasal sprays from internet sites. Acetylfentanyl was among the first to appear on the market and caused a large number of deaths [25,30]. Furanylfentanyl appeared on the market for a short period, and when found in postmortem cases, it was almost always in the context of an opioid overdose [12]. Hence, the mere detection of a fentanyl analogue should raise the suspicion of an opioid toxicity death. Other asphyxiants There are a number of other substances which may cause asphyxia. Severe poisonings may be caused by 354 Asphyxiation, Suffocation, and Neck Pressure Deaths industrial exposures, and suicide attempts have been reported among laboratory workers [4]. Strychnine is a classic poison which eliminates the inhibition of all nerves and results in tetanus-like convulsions. Deaths are generally due to asphyxiation caused by failure of the respiratory muscles to contract in a regular pattern [27]. This drug is no longer marketed, but barbiturate intoxications with preparations that have been removed from the market still occur since many people keep drugs for long periods of time. Organophosphorus compounds present in many pesticides are responsible for a substantial number of deaths, particularly in the least developed, low-income countries, and are known to produce respiratory arrest. Although acetylcholinesterase inhibition is believed to be the pathophysiological mechanism behind the respiratory failure, it has recently been observed that a hypoperfusion of the respiratory control centres in the brainstem contributes to the inhibition of the respiratory muscles [18]. Role of 6-monoacetylmorphine in the acute release of striatal dopamine induced by intravenous heroin. Postmortem and toxicological findings in a series of furanylfentanyl-related deaths. Studies on the respiratory chain-linked reduced nicotinamide adenine dinucleotide dehydrogenase. Puffer fish poisoning in Bangladesh: Clinical and toxicological results from large outbreaks in 2008. An epidemic of tetrodotoxin poisoning following ingestion of the horseshoe crab Carcinoscorpius rotundicauda. Central respiratory effects on motor nerve activities after organophosphate exposure in a working heart brainstem preparation of the rat. Macisaac J, Harrison R, Krishnaswami J, McNary J, Suchard J, Boysen-Osborn M, Cierpich H, Styles L, Shusterman D. The potential threat of acetyl fentanyl: Legal issues, contaminated heroin, and acetyl fentanyl "disguised" as other opioids. Characteristics and outcome of children with carbon monoxide poisoning with and without smoke exposure referred for hyperbaric oxygen therapy. The inhibition of mitochondrial cytochrome oxidase by the gases carbon monoxide, nitric oxide, hydrogen cyanide and hydrogen sulfide: Chemical mechanism and physiological significance. Hair morphine concentrations of fatal heroin overdose cases and living heroin users. Evaluation of the role of abstinence in heroin overdose deaths using segmental hair analysis. Typical symptoms after neck compression are dysphagia, dysphonia, tenderness and pain of the laryngeal region, especially when moving the neck. The percentage of victims losing consciousness during the assault varies depending on the composition of the study material. The same applies to the frequency of involuntary loss of urine and faeces, which almost exclusively happens in association with unconsciousness. Retrograde amnesia was reported in a quarter of the victims who had become unconscious in the course of neck compression [33]. Occasionally, fractures of the cricoid cartilage and tracheal disruption can lead to stridor and life-threatening respiratory distress. If the space between the larynx and the spine is infiltrated with blood or oedema fluid, the normal laryngeal crepitus felt in movements from side to side may be absent [11]. Blood extravasations due to congestion provide important diagnostic clues not only in cases of fatal strangulation, but also in survived assaults to the neck. It has to be emphasized, however, that this finding is not a specific sign of asphyxia. Petechial haemorrhages in the conjunctivae have been repeatedly reported in physiological processes involving a pressing effect (labour, fits of coughing, massive vomiting) [10]. In surviving strangulation victims, the presence of petechial bleedings depends on several factors, i. Isolated petechiae in the eyelids and conjunctivae may escape detection after only a relatively short period of time. On the other hand, there are examples in which it took several weeks until a confluent subconjunctival haemorrhage (hyposphagma) disappeared completely. Obstruction of venous outflow and at least partly maintained arterial inflow (vertebral arteries) are considered essential causes of congestion. In strangulation using the forearm, obstruction of arterial blood flow to the brain is the major pathophysiological mechanism resulting in a rapid loss of consciousness. The potentially life-threatening effects of neck compression are essentially due to occlusion of the cervical Survived injuries from manual and/or ligature strangulation are a common issue in clinical forensic medicine, whereas abortive attempts of hanging are rare. Manual and ligature strangulation In neck compressions by an offender, most victims are female, whereas the perpetrators are mainly males [15]. Statistically, the number of manual strangulations is higher than that of ligature strangulations. In a large percentage of survived strangulations, both the offender and the victim are intoxicated [12]. The perpetrator is often somebody close to the victim (husband, life partner, ex-boyfriend, neighbour, colleague, etc. Local injuries on the neck range from vague reddening via different forms of abrasion to intra- and subcutaneous haematomas. It is often associated with superficial epidermal defects and intracutaneous bleeding. Mere reddening of the skin remains visible for about 2 days after the incident at the most [20]. Consequently, victims of assaults to the neck should be examined as soon as possible. The same applies to suspects, as strangling perpetrators may be injured themselves when they meet resistance. Usually the ligature mark more or less encircles the neck, presenting as streak-like reddening, which is sometimes accompanied by excoriations [29]. The victim was strangled with both hands in a supine position and lost consciousness. Medicolegal examination and photo-documentation took place about 5 hours after the offence. In the more recent literature, many authors are of the opinion that sudden death due to a short grip to the neck is possible only in individuals with a respective disposition and does not occur under normal circumstances [19]. In this context it is interesting that articles dealing with sports medicine do not report on carotid sinus reflex deaths, although considerable pressure is applied to the lateral cervical region in some forms of martial art [24]. Apart from local findings on the neck and signs of venous congestion [28], a high percentage of strangulation victims also show concomitant injuries in other body regions. Survived attempts of hanging Cases of survived hanging are rare in forensic medicine. As these are predominantly suicide attempts, which are not subject to punishment as such, no forensic investigation is ordered in most instances.
Generic clarinex 5mg line
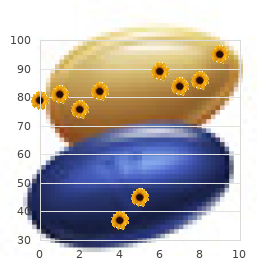
In this case allergy medicine no drowsiness buy generic clarinex from india, the protocol is based on the T2 water Dixon sequence and may also be T1-weighted, with and without fat saturation, lasting less than 30 minutes. Note the fluid level in the trachea with liquid (thin arrow) and a hyperdense sand-like material (thick arrow) with a horizontal limit between both structures. However, the study also warns that this sign cannot be interpreted as specific, since it is also present in near-drowning cases or even in any other types of case, such as natural death. Liquid is, however, present in both the paranasal sinuses and in the trachea and bronchi [22]. Again, these diagnostic criteria may be criticised since their specificity is considered low (8% according to one study [22]). Some authors have investigated the presence of pulmonary emphysema by looking for the level of the right hemidiaphragm dome. According to one study [31], its position is significantly lower in cases of drowning than in other cases. These results should, however, be treated with caution, because of the very low number of studies (30 cases only). This finding seemed to be related to drowning, according to those results, but, so far, no studies have been performed to validate the results on a larger collective. Other studies indicate pulmonary oedema in cases of drowning, but none of them describes this finding as a specific finding [4,31,36]. Air-fluid levels with the paranasal cavities: frontal (thin arrows), maxillary (thick arrows) and sphenoid sinuses (asterisk). These cases usually also show slight pleural effusion and no pulmonary consolidation. Radiologically, it can be detected by a decrease in the mean attenuation of the blood that is notable in the heart cavities. It is therefore recommended to measure the density of the blood in the left cardiac chambers [1]. Suffocation due to an obstruction of the airways is regularly seen in cases of accidental death, especially in small children, in the elderly, and in cases of homicide by way of voluntary occlusion of mouth and nose. As already mentioned, imaging is not the method of choice to investigate the most important findings in cases of asphyxia, such as petechiae and small lesions in the soft tissue. This is why it would be impossible to detect haemorrhages in the mucosa of the mouth or small haemorrhages in facial muscles. So, imaging methods have only limited application in such cases, which should be investigated with a detailed external and internal examination, with dissection of the soft tissue, layer by layer. It has several advantages, but medical examiners using this technique need also to be aware of its limits (see Table 9. Bronchoaspiration is important in cases of asphyxia as well as being a vital sign. In fact, the presence of nodular infiltrations in pulmonary parenchyma indicates peripheral aspiration Also, it is extremely sensitive in detecting gas and air [9,24], so even the smallest quantities of pneumothorax, air embolism, etc. Cases of traumatic mechanical asphyxia are therefore an excellent example of the complementary nature of conventional autopsy and modern cross-sectional imaging. No rib fracture was noted, although significant compression of the chest was evident. Conclusion Although forensic conventional examination of the body (external and internal) remains the gold standard for examining victims of asphyxia, forensic imaging has a role in the investigations of those cases. Its major weakness is the low sensitivity in detecting small lesions in the soft tissue, especially petechiae and haemorrhages in the cervical or facial muscles. It is also sensitive enough to detect hypoxic and ischaemic cerebral lesions, which will increase its importance in investigating cases of asphyxia in the future. Virtual autopsy using multislice computed tomography in forensic medical diagnosis of drowning. Chevallier C, Doenz F, Vaucher P, Palmiere C, Dominguez A, Binaghi S, Mangin P, Grabherr S. Clinical radiology and post-mortem imaging (Virtopsy) are not the same: Specific and unspecific post-mortem signs. The Virtopsy Approach: 3D Optical and Radiological Scanning and Reconstruction in Forensic Medicine. Egger C, Bize P, Vaucher P, Mosimann P, Schneider B, Dominguez A, Meuli R, Mangin P, Grabherr S. Delayed postanoxic encephalopathy with visual field disturbance after strangulation: A case report. Assessment of the relationship between drowning and fluid accumulation in the paranasal sinuses on post mortem computed tomography. Kawasumi Y, Kawabata T, Sugai Y, Usui A, Hosokai Y, Sato M, Saito H, Ishibashi T, Hayashizaki Y, Funayama M. Diagnosis of drowning using post-mortem computed tomography based on the volume and density of fluid accumulation in the maxillary and sphenoid sinuses. Post-mortem imaging of laryngohyoid fractures in strangulation incidents: First results. Injuries to the hyoid bone and laryngeal cartilages: effectiveness of different methods of medico-legal investigation. Delayed bilateral internal carotid artery thrombosis following accidental strangulation. Massive gas embolism revealed by two consecutive post-mortem computed-tomography examinations. Patient presentation, angiographic features and treatment of strangulation-induced bilateral dissection of the cervical internal carotid artery. Delayed left anterior and middle cerebral artery haemorrhagic infarctions after attempted strangulation: A case report. Evaluation and management for carotid dissection in patients presenting after choking or strangulation. Neuropsychological profile following suicide attempt by hanging: Two adolescent case reports. It is also important to find out whether any objects were surrounding the body and/ or underneath the neck structures at the scene. It is also useful to note the position of the clothing in relation to the neck at the primary scene. The forensic practitioner can instruct the police officers for necessary photographs to be obtained at the scene. Depending on the time of the body is discovered at the scene and the time interval before the autopsy, the postmortem findings and artefacts are varied. As a result, it is important to take good photographs at the scene even prior to the arrival of the forensic pathologist. It is essential to perform a comprehensive autopsy in deaths due to asphyxiation, suffocation and neck pressure. The forensic practitioner and the prosecutor performing the autopsy should be aware of the circumstances of the death prior to dissection and should possess a sound knowledge of the neck anatomy. All forensic pathology training programmes and pathology assistant or autopsy technician training programmes train forensic professionals to perform this task well. One of the major challenges for forensic pathologists is the correct interpretation of observational findings made during external and internal examination of the neck. Often postmortem neck injuries provide considerable difficulties due to anatomical variations of the neck and difficulty in differentiating artefacts from real pathological findings. Sometimes it is difficult to establish the diagnosis of neck injuries as the primary or the contributing cause of death. Often the range of haemorrhage associated with neck compression can overlap with artefacts, giving difficulty in diagnosis in neck injury. That is why it is essential to perform a systemic examination of the neck structures and integrate findings with caution when you provide the final diagnosis. Postmortem examination As a systemic approach is necessary for postmortem examination, we recommend that the following steps are followed during the autopsy. We recommend enlisting the help of a technician who is capable of operating the device being used in case the operator is not familiar with it. Prerequisites and systematic approach for the autopsy In case of neck injury, a systemic approach for autopsy including the history and circumstances, external examination findings, internal examination findings, ancillary studies and evidence-based opinion is essential. As prerequisites, it is necessary to have the history and scene information and we recommend carrying out a scene visit before the start of the autopsy.
Purchase 5mg clarinex mastercard
The underlying histological changes constituted vacuolation of the basal mucosal cells allergy medicine 3 year old order clarinex 5 mg, basal cell dissolution, desquamation of surface epithelial cells, and discrete inflammatory infiltration of the submucosa. In keeping with the literature, the cases reported here emphasize that the diagnosis of cyanide intoxication cannot reliably be established at autopsy because the indicative morphological findings are difficult to recognize unequivocally or may even be missing. Injuries ex post attributable to a fall during agony, as in Case 1, have been reported in approximately 15 per cent of cases [129]. At autopsy, considerable caution should be exercised in an attempt to smell cyanide, because this procedure is associated with the risk of inhaling cyanide fumes [4]. In a retrospective survey of 36 fatalities in the bathtub in Ghent from 1934 to 1983, Devos et al. In a series of 42 deaths in the bath in Copenhagen and Gothenburg from 1961 to 1969, Geertinger and Voigt [63] encountered one homicide. Retrospective analysis of 245 fatalities in the bathtub in Hamburg from 1971 to 1988 revealed 13 homicides (5. Several cases of homicidal electrocution in the bathtub have been reported in detail [134,153,179]. There is, however, a lack of more comprehensive analysis covering the variety in the range from homicides actually occurring in the bathtub to mere deposition of the corpse to cover traces. In a case of manual strangulation with subsequent submersion of the corpse in a bathtub described by Spitz [161], however, initial examination of the body at the scene had only revealed two small whitish areas on the side of the neck while autopsy of the dried body showed unequivocal nail marks. Our own retrospective analysis of the fatalities investigated in the Institute of Forensic Medicine, University of Cologne, from 1980 to 1993 revealed 215 fatalities in the bath, i. In six of these cases, the bathtub was filled with water and empty in four when the corpse was encountered. In one case the circumstances indicated that the bathtub had originally been filled with water that had been let out before the discovery of the corpse. Although the mouth and nose were found without exception to be beneath the surface of the water, the autopsy revealed signs of drowning in only four fatalities (one of them coming out of an empty bathtub). The diagnosis of lethal drowning was made in two cases based on the circumstances of death, complete autopsy and negative toxicological screening. In five cases, death was attributed to strangulation and in four cases to sharp violence. In eight cases, findings of severe miscellaneous violence were encountered at the autopsy, leaving no doubt as to the manner of death. In contrast, two fatalities showing only discrete signs of injury on external examination were not recognized as homicides at the scene. Four corpses had merely been deposited in the bathtub, and waterlogging had not actually influenced the lethal outcome. Four homicides were committed partly or completely in the bathtub (drowning, strangulation, ligature strangulation with the tube of the shower). In two cases the scenario raised the question of whether the victim had been put into the bathtub after manual strangulation to ensure death by electrocution. Case 2 In the second case, a 37-year-old woman was found dead in her bathtub with her mouth and nose submerged in water and abundant white foam escaping from the mouth. In addition, haemorrhages of the skin were found in the sacral region and over both elbows as well as haemorrhages of the soft tissues covering the thoracic and lumbar spinal column and the left clavicula. The lungs were large and bulky and on cut sections had a brick-red appearance with large quantities of foamy oedema fluid flowing from the cut surfaces. Case 1 In this case, a 32-year-old woman was found dead by her husband in the bathtub, lying undressed, face down, with her mouth and nose beneath the surface of the water. On the floor of the living room a pool of blood was encountered with a trace of dragging leading in the direction of the bathroom. The autopsy revealed a ligature mark of the neck, corresponding paleness of the mucous membrane of the gullet and multiple petechiae of the conjunctivae. In addition, a deep incised wound of the throat was found, but there were no signs of blood aspiration, air embolism or marked anaemia of the internal organs due to haemorrhage. In court the perpetrator confessed that, in the course of a fight with a sexual background, he had first strangled the woman with the electric cord, inflicted the incised wound of the neck and then submerged the corpse in the bathtub. The analysis of our autopsy material, however, is intended to give a survey of the entire spectrum encountered and to elucidate the problems in establishing the diagnosis of cause and manner of death apart from drowning and electrocution. In our material comprising only homicides, autopsy revealed evidence of aspirating, respectively swallowing water in 36 per cent of the cases. In every case they indicated that the victim was still alive when entering or being put into the bathtub. In one case the autopsy findings of drowning brought about the suspicion of homicide, and in two cases drowning was the cause of death. In comparison, analysis of the literature cited in the tables above renders the following distribution: 14 by strangulation, 10 by drowning, 6 by electrocution, 5 by blunt force and 5 by sharp force. The lack of homicidal electrocution in our material is due to the fact that this cause of death was not proved beyond doubt in any case. Although findings of severe miscellaneous violence allowed the unequivocal diagnosis of homicide in eight cases, one case of drowning and one case of manual strangulation were not recognized before the autopsy (possible reasons are discussed below). Case 3 In the third case, a 55-year-old woman was found by her son face down submerged in her bathtub, with her mouth and nose beneath the water. Faint haemorrhages and scratches of the skin and the neck recognized on external examination at the scene were supposed to be related to a necklace. Looking at the case reports, in Case 1 the autopsy findings were in good agreement with the later confession of the perpetrator. According to the classification of Kruger and colleagues [90], the corpse had merely been deposited in the bathtub and this was of no importance for the occurrence of death. In another case the perpetrator explained that he had stabbed his wife and then given her a shower to remove the traces [90]. In a further case in our material, the perpetrators described stabbing their victim and then submerging them in the bathtub to ensure death. Considering the circumstances at the scene, the severe injuries of the neck as well as the haemorrhages in the skin and the soft tissues of the neck may have been related to a blunt force pushing the body against the front side of the bathtub, and they leave no doubt as to the diagnosis of homicide. Particularly in cases of ligature or manual strangulation, the police and the forensic pathologist may encounter serious difficulties in establishing the cause of death (as observed by Spitz [161]). Mueller [121] has emphasized that abrasions of the skin due to manual strangulation or other causes may be barely visible on wet skin but become more obvious some hours later. In particular, the surface pattern reflecting the nature of the ligature may disappear. Bode and Kampmann [28] succeeded in making an experimentally produced strangulation furrow completely disappear by combined treatment with ointments and exposure to water. These observations and experimental results underline the belief that a thorough autopsy should be carried out on every suspicious fatality in the bathtub, even if first examination at the scene does not reveal any severe injury. About 65 per cent of the child homicides were committed by the mother in the parental flat, predominantly in the early hours of the evening during the weekend. The modes of death were 9 blunt injury, 6 sharp violence, 6 strangulation, 3 smothering, 2 drowning, 2 gunshot and 5 neglect (starvation) (Table 18. The defenseless, helpless and immobile condition of the infant particularly favours a homicide by manual assault, smothering or neglect (starvation). With the exception of one case with a deep incised wound of the neck, external injuries such as ligature mark, abrasions, contusions and fingernail marks were unequivocally visible, and the same was true for petechiae of the conjunctivae, sclerae and face. Haemorrhages of the soft tissues surrounding the thyroid cartilage and the hyoid bone were frequently encountered but, due to minor calcification in the child, no fracture was found.
Buy clarinex master card
Side effects include an elevated risk of heart attack or stroke in smokers and in women with a history of diabetes allergy forecast lawton ok cheap clarinex 5 mg online, hypertension, or clotting disorders. Also available is a soft, flexible vaginal ring that releases estrogen and progestin for absorption through the vaginal mucosa. It must be worn continually for 3 weeks and removed for the fourth week of each cycle. It provides highly reliable, long-term contraception, although in some women it causes headaches, nausea, or weight gain, and fertility may not return immediately when its use is discontinued. Some drugs can be taken orally after intercourse to prevent implantation of a conceptus. It can be taken up to 120 hours after intercourse and induces menstruation within 2 weeks. It is used less as a contraceptive than as an abortifacient; in high doses, it induces abortion up to 2 months into pregnancy. But at a dose of 2 mg/day, it prevents ovulation like other steroidal contraceptives, and a single 10 mg dose can also be used as an emergency "morning-after" contraceptive if taken after intercourse but before ovulation. Issues in Choosing a Contraceptive Many issues enter into the appropriate choice of a contraceptive, including personal preference, pattern of sexual activity, medical history, religious views, convenience, initial and ongoing costs, and disease prevention. Each column shows the number of sexually active women who typically become pregnant within 1 year while they or their partners are using the indicated contraceptives. The lowest rate (perfect use) is for those who use the method correctly and consistently, whereas the higher rate (typical use) is based on random surveys of users and takes human error (lapses and incorrect usage) into account. We have not considered all the currently available methods of contraception or all the issues important to the choice of a contraceptive. Further information necessary to a sound choice and proper use of contraceptives should be sought from a health department, college health service, physician, Planned Parenthood, or other such sources. Sexual arousal constricts the male internal urinary sphincter, which prevents reflux of semen into the male urinary bladder; prostatic hyperplasia can impede urine flow; pregnancy crowds the bladder, reduces its capacity, and may cause incontinence; pregnancy promotes salt and water reabsorption by the kidneys and increases glomerular filtration rate and urine output. Thelarche, pubarche, and menarche as signs of female puberty; their hormonal causes; and the hormonal basis of the libido 4. Ovarian and hormonal changes that bring on female climacteric and menopause; effects commonly experienced by perimenopausal women; and differences between female and male climacteric 7. The criterion for determining that a woman has passed through menopause, and the reason one cannot identify the exact time of menopause 10. The process of ovulation, the day on which it occurs in a typical cycle, and how the egg gets into the uterine tube 12. Production, structure, function, and eventual involution of the corpus luteum; why days 15 through 28 of a typical cycle are called the luteal phase; what remains after a corpus luteum has fully involuted 13. Four phases of the menstrual cycle; what happens histologically to the endometrium in each phase; what days of the cycle are spanned by each phase; and what hormones regulate these changes Assess Your Learning Outcomes To test your knowledge, discuss the following topics with a study partner or in writing, ideally from memory. What mature female structures arise from the embryonic genital tubercle, urogenital folds, and labioscrotal folds 3. Internal structure of the ovary; its supportive ligaments; and its blood and nerve supplies 4. Gross anatomy of the uterine (fallopian) tube; its three segments; its supportive ligament; and the structure of its mucosa and relationship of that structure to its function 6. Gross anatomy of the uterus; its supportive ligaments; its relationship to the vesicouterine and rectouterine pouches; its blood supply; and function of the cervical glands 7. Tissue layers of the uterine wall; histology of the endometrium; functions of the endometrial sublayers 8. The tilt of the vagina and its relationship to adjacent organs; histology of its mucosa in childhood and adulthood; significance of its dendritic cells; sources of its lubrication; and anatomy of the hymen 9. Anatomy of the vulva including the mons pubis, labia majora and minora, clitoris and prepuce, vaginal and urethral orifices, accessory glands, and erectile tissues 10. The prevalence of breast cancer; its diagnostic signs; genetic and other risk factors for breast cancer; preventive breast care; and treatment options 28. Meanings of and distinctions between the female sexual cycle, ovarian cycle, and menstrual cycle 2. Prenatal development of oogonia and primary oocytes; the peak number of oogonia typically attained in the fetus; why this number is so much less at the time of birth and again by the onset of puberty; and the name for the prenatal and childhood degeneration of female germ cells 4. Ways in which meiosis in the female differs from that in the male; why male gametogenesis produces four functional gametes per stem cell and female gametogenesis produces only one; what happens to the other three meiotic daughter cells in the female 5. How far meiosis has progressed by the time the egg is ovulated, and what must happen thereafter for meiosis to be completed 6. Development of a follicle from primary to mature (graafian) types; the structural differences between the stages; and how folliculogenesis is correlated with oogenesis 7. The timetable of oogenesis and folliculogenesis; why the ovarian cycle is considered to average 28 days long whereas any given egg and follicle take much longer to mature; and what event marks day 1 of a cycle 9. How many follicles begin to develop in each cycle of folliculogenesis; how many of them normally ovulate; what happens to the rest, and what that fate is called 28. Physiological responses of orgasm and resolution in the female and how they differ from those of the male; absence of a refractory period and potential for multiple orgasms 28. Sources and effects of estrogen, progesterone, and human chorionic gonadotropin in pregnancy 5. Effects of thyroid hormone, parathyroid hormone, glucocorticoids, aldosterone, and relaxin in pregnancy 6. Causes of morning sickness, constipation, and heartburn in pregnancy; the change in basal metabolic rate and the related nutritional needs of pregnancy 7. Effects of pregnancy on blood volume and cardiac output; how pregnancy can cause edema, hemorrhoids, and varicose veins 8. Effects of pregnancy on respiratory function; the mechanism for enhancing diffusion of carbon dioxide from the fetal blood into the maternal blood of the placenta 28. The neuroendocrine reflex stimulated by the suckling of an infant, and the roles of oxytocin and prolactin in breast-feeding 5. How breast milk varies in composition from one time to another; which components of the milk are released early, and which are released nearer the end, of a single feeding 7. The daily quantity of breast milk typically produced (eventually) and its nutritional demands on the mother 9. Effects of pregnancy on glomerular filtration, urine output, and the capacity of the bladder 10. Effects of pregnancy on the skin; causes of striae (stretch marks), the linea nigra, and chloasma 11. The vertex position and the developmental age at which the fetus typically assumes it 12. The nature and possible cause of Braxton Hicks contractions, when they occur, and how they differ from true labor contractions 13. Factors that stimulate the onset of labor contractions; the roles of oxytocin, positive feedback, and the voluntary abdominal muscles in labor 28. Influences of estrogen, growth hormone, insulin, glucocorticoids, and prolactin on mammary gland development during pregnancy 2. The fluid secreted by the mammary glands for the first few days postpartum, how it differs from breast milk, and its benefits to the neonate Testing Your Recall 1. Of the following organs, the one(s) most comparable to the penis in structure is/are a. The hormone that most directly influences the secretory phase of the menstrual cycle is a. Smooth muscle cells of the myometrium and myoepithelial cells of the mammary glands are the target cells for a. A yellowish structure called the secretes progesterone during the secretory phase of the menstrual cycle. A tertiary follicle differs from a primary follicle in having a cavity called the. All the products of fertilization, including the embryo or fetus, the placenta, and the embryonic membranes, are collectively called the. The funnel-like distal end of the uterine tube is called the and has feathery processes called. A slim girl who is active in dance and gymnastics is likely to begin menstruating at a younger age than an overweight inactive girl. Women do not lactate while they are pregnant because prolactin is not secreted until after birth. Colostrum contains more fat than mature milk, ensuring the neonate of adequate Answers in Appendix A caloric intake in its first month of separation from placental nutrition.
Clarinex 5mg
During chewing allergy shots dosage schedule buy clarinex 5 mg with mastercard, the tongue collects food, presses it against the palate to form a bolus, and pushes it posteriorly. When the bolus reaches a critical size, the epiglottis tips posteriorly and the bolus slides around it, through a space on each side, into the laryngopharynx. The soft palate and root of the tongue block food and drink from entering the nasal cavity or reentering the mouth. To prevent choking, breathing is automatically suspended, the infrahyoid muscles pull the larynx up to meet the epiglottis and cover the laryngeal opening, and the vocal cords adduct to close the airway. The pharyngeal constrictors contract in order from superior to middle to inferior, driving the bolus downward into the esophagus. The esophageal phase is a wave of involuntary contractions called peristalsis, controlled jointly by the brainstem swallowing center and the myenteric plexus in the esophageal wall. The bolus stimulates stretch receptors that feed into the plexus, which transmits signals to the muscularis externa above and below the bolus. The circular muscle layer above the bolus constricts and pushes the food downward. Below the bolus, the circular muscle relaxes while the longitudinal muscle contracts. The latter action pulls the wall of the esophagus slightly upward, making it a little shorter and dilating it to receive the descending food. When one is standing or sitting upright, most food and liquid drop through the esophagus by gravity faster than the peristaltic wave can keep up with them. Liquid normally reaches the stomach in 1 to 2 seconds and a food bolus in 4 to 8 seconds. As a bolus reaches the lower end of the esophagus, the lower esophageal sphincter relaxes to let it pass into the stomach. The palate, tongue, vocal cords, and epiglottis block the oral and nasal cavities and airway while pharyngeal constrictors push the bolus into the esophagus. Peristalsis drives the bolus downward, and relaxation of the lower esophageal sphincter admits it into the stomach. Imagine a line from the root canal of a tooth to the adjacent bone of the mandible. What is the difference in function and location between intrinsic and extrinsic salivary glands Identify at least two histological features of the esophagus that are especially tied to its role in swallowing. Describe the mechanisms that prevent food from entering the nasal cavity and larynx during swallowing. It is divided into four regions: (1) the cardial part (cardia) is a small area within about 3 cm of the cardial orifice. The pylorus is surrounded by a thick ring of smooth muscle, the pyloric sphincter, which regulates the passage of chyme into the duodenum. Between the esophagus and duodenum, the stomach has two margins called the greater and lesser curvatures. The greater curvature is the long way around, about 40 cm, along the inferolateral surface. The greater omentum, overhanging the small intestine, is suspended from the greater curvature. The lesser curvature is the shorter distance from esophagus to duodenum, about 10 cm, along the superomedial margin facing the liver. The lesser omentum spans the space between the liver and lesser curvature (see fig. All blood drained from the stomach and intestines enters the hepatic portal circulation and filters through the liver before returning to the heart. The stomach is a muscular sac in the upper left abdominal cavity immediately inferior to the diaphragm. It functions primarily as a food storage organ, with an internal volume of about 50 mL when empty and 1. When extremely full, it may hold up to 4 L and extend nearly as far as the pelvis. Well into the nineteenth century, authorities regarded the stomach as essentially a grinding chamber, fermentation vat, or cooking pot. We now know that it mechanically breaks up food particles, liquefies the food, and begins the chemical digestion of proteins and fat. This produces an acidic, soupy or pasty mixture of semidigested food called chyme9 (pronounced 25. The apical regions of its cells are filled with mucin; after it is secreted, mucin swells with water and becomes mucus. The lamina propria is almost entirely occupied by tubular glands, to be described shortly. The muscularis externa has three layers, rather than two: outer longitudinal, middle circular, and inner oblique layers (fig. Note d: Steve Gschmeissner/Science Source the absence of chief cells and relatively few parietal cells. Two or three tubular glands open into the bottom of each gastric pit and span the rest of the lamina propria. In the cardial and pyloric regions, they are called cardial glands and pyloric glands, respectively. In gastric glands, they are called mucous neck cells and are concentrated in the narrow neck of the gland, where it opens into the gastric pit. Regenerative (stem) cells, found in the base of the pit and neck of the gland, divide rapidly and produce a continual supply of new cells. Newly generated cells migrate upward to the gastric surface as well as downward into the glands to replace cells that die. Parietal cells, found mostly in the upper half of the gland, secrete hydrochloric acid, intrinsic factor, and an appetite-stimulating hormone called ghrelin. They are found mostly in the gastric glands, but a few occur in the pyloric glands. Chief cells, so named because they are the most numerous, secrete the enzymes gastric lipase and pepsinogen. They dominate the lower half of the gastric glands but are absent from cardial and pyloric glands. Enteroendocrine cells, concentrated especially in the lower end of a gland, secrete hormones and paracrine messengers that regulate digestion. They occur in all regions of the stomach, but are most abundant in the gastric and pyloric glands. There are at least eight kinds of enteroendocrine cells in the stomach, each of which produces a different chemical messenger. Because of the bicarbonate, blood leaving the stomach has a higher pH when digestion is occurring than when the stomach is empty. Stomach acid has several functions: (1) It activates the enzymes pepsin and lingual lipase, as discussed shortly. This is more acidic than the battery acid of a car and low enough to dissolve tooth enamel or cause a chemical burn on the skin. Since pepsin digests protein, and pepsinogen itself is a protein, pepsin has an autocatalytic effect-as some pepsin is formed, it converts pepsinogen into more pepsin (fig. The ultimate function of pepsin, however, is to digest dietary proteins to shorter peptide chains, which then pass to the small intestine, where their digestion is completed. As we age, the gastric mucosa atrophies and less intrinsic factor is secreted, increasing the risk of anemia. Some people, especially in old age, develop pernicious anemia, the result of an autoimmune disease that destroys gastric mucosa and reduces intrinsic factor secretion. Chemical Messengers the gastric and pyloric glands have various kinds of enteroendocrine cells that collectively produce as many as 20 hormones and paracrine signals. The functions of some of these peptides in digestion will be explained in the following sections, and their roles in appetite regulation are discussed in the next chapter (section 26. This enzyme and lingual lipase, which plays a minor role, digest 10% to 15% of the dietary fat in the stomach. Intrinsic Factor Parietal cells secrete a glycoprotein called intrinsic factor that is essential for the absorption of vitamin B12 by the small intestine. Intrinsic factor binds vitamin B12 and the intestinal cells then absorb this complex by receptor-mediated endocytosis.
Buy clarinex 5mg otc
Female sexual response allergy symptoms pollen sore throat generic 5 mg clarinex overnight delivery, the physiological changes that occur during intercourse, may be viewed in terms of the four phases identified by Masters and Johnson and discussed in section 27. The neurological and vascular controls of the female response are essentially the same as in the male and need not be repeated here. Both have a pair of corpora cavernosa with deep arteries and become engorged by the same mechanism. The glans and shaft of the clitoris swell to two or three times their unstimulated size, but since the clitoris cannot swing upward away from the body like the penis, it tends to withdraw beneath the prepuce. Thrusting of the penis in the vagina tugs on the labia minora and, by extension, pulls on the prepuce and stimulates the clitoris. The clitoris may also be stimulated by pressure between the pubic symphyses of the partners. The breasts also become congested and swollen during the excitement phase, and the nipples become erect. Orgasm is commonly described as an intense sensation spreading from the clitoris through the pelvis, sometimes with pelvic throbbing and a spreading sense of warmth. The uterus exhibits peristaltic waves of contraction, which may help to draw semen from the vagina. The anal and urethral sphincters constrict, and the paraurethral glands, homologous to the prostate, sometimes expel fluid similar to prostatic fluid. Tachycardia and hyperventilation occur; the breasts enlarge still more and the areolae often become engorged; and in many women, a reddish, rashlike flush appears on the lower abdomen, chest, neck, and face. The orgasmic platform quickly relaxes, while the inner end of the vagina returns more slowly to its normal dimensions. The flush disappears quickly and the areolae and nipples undergo rapid detumescence (loss of vascular congestion), but it may take 5 to 10 minutes for the breasts to return to their normal size. Unlike men, women do not have a refractory period and may quickly experience additional orgasms. Although vasocongestion works by the same mechanism in both sexes, its effects are quite different in females. The labia majora redden and enlarge, then flatten and spread away from the vaginal orifice. The lower one-third of the vagina constricts to form a narrow passage called the orgasmic platform, owing partly to vasocongestion of the vestibular bulbs that bracket the vaginal orifice (see fig. The narrower canal and the vaginal rugae (friction ridges) enhance stimulation and help induce orgasm in both partners. Increased blood flow in the vaginal wall turns it purple and produces a serous fluid, the vaginal transudate, that seeps through the wall into the canal. Along with secretions of the greater vestibular glands, this moistens the vestibule and provides lubrication. The uterus, which normally tilts forward over the urinary bladder, stands more erect during excitement and the cervix withdraws from the vagina. Although the vagina is the female copulatory organ, the clitoris is more comparable to the penis in structure, physiology, and importance as the primary focus of sexual stimulation. It has a high concentration of sensory nerve endings, which, by contrast, are relatively scanty in the vagina. All the products of conception-the embryo or fetus as well as the placenta and membranes associated with it-are collectively called the conceptus. The developing individual is a hollow ball called a blastocyst for much of the first 2 weeks, an embryo from day 16 through week 8, and a fetus from the beginning of week 9 until birth. The fetus is attached by way of an umbilical cord to a disc-shaped placenta on the uterine wall. The placenta provides fetal nutrition and waste disposal, and secretes hormones that regulate pregnancy, mammary development, and fetal development. The levels of these hormones in the maternal blood over the course of the pregnancy provide a good indicator of the well-being of the fetus. They are secreted primarily by the placenta, but the corpus luteum is an important source of hormones in the first several weeks. If the corpus luteum is removed before week 7, the pregnancy almost always miscarries (aborts). From weeks 7 to 17, the corpus luteum degenerates and the placenta takes over its endocrine functions. How does the changing ratio of estradiol to progesterone relate to the onset of labor contractions Its presence in the urine is the basis of pregnancy tests and can be detected with home testing kits as early as 8 or 9 days after conception. The most abundant estrogen of pregnancy is estriol, but its effects are relatively weak; estradiol is less abundant but 100 times as potent. It makes the pubic symphysis more elastic and the sacroiliac joints more limber, so the pelvis widens during pregnancy and the pelvic outlet expands during childbirth. Progesterone the placenta secretes a great deal of progesterone, and early in the pregnancy, so does the corpus luteum. It prevents menstruation and promotes the proliferation of decidual cells of the endometrium, on which the blastocyst feeds. Once estrogen has stimulated growth of the mammary ducts, progesterone stimulates development of the secretory acini-another step toward lactation. Estrogens Estrogen secretion increases to about 30 times the usual amount by the end of gestation. The corpus luteum is an important source of estrogen for the first 12 weeks; after that, it comes mainly from the placenta. Digestive System, Nutrition, and Metabolism For many women, one of the first signs of pregnancy is morning sickness-nausea, especially after rising from bed-in the first few months of gestation. One hypothesis is that it stems from the reduced intestinal motility caused by the steroids of pregnancy. The fetus is most vulnerable to toxins at the same time that morning sickness peaks. Women with morning sickness tend to prefer bland foods and avoid spicy and pungent foods, which are highest in compounds that could be toxic to the fetus. Occasionally, this is severe enough to require hospitalization (see hyperemesis gravidarum in table 28. The latter is due to the enlarging uterus pressing upward on the stomach, causing the reflux of gastric contents into the esophagus. Pregnant women often feel overheated because of this and the effort of carrying the extra weight. The appetite may be Other Hormones Many other hormones induce additional bodily changes in pregnancy (table 28. Elevated thyroid hormone secretion increases the metabolic rate of the mother and fetus. In humans, it synergizes progesterone in stimulating the multiplication of decidual cells in early pregnancy and promotes the growth of blood vessels in the pregnant uterus. Some women overeat, however, and gain as much as 34 kg (75 lb) of weight compared with a healthy average of 11 kg (24 lb). In preparation for this, the placenta stores nutrients early in gestation and releases them in the final trimester. A pregnant woman needs an extra 600 mg/day of iron for her own added hematopoiesis and 375 mg/day for the fetus. Supplemental vitamin K is often given late in pregnancy to promote prothrombin synthesis in the fetus. In the United States, newborns are routinely given an injection of vitamin K to minimize the risk of neonatal hemorrhage, especially in the brain, caused by the stresses of birth. A vitamin D supplement helps to ensure adequate calcium absorption to meet fetal demands. Supplemental folic acid reduces the risk of neurological disorders in the fetus, such as spina bifida and anencephaly (failure of the cerebrum, cerebellum, and calvaria to develop), but it is effective only if taken habitually prior to conception. Urinary System Aldosterone and the steroids of pregnancy promote water and salt retention by the kidneys. Nevertheless, the glomerular filtration rate increases by 50% and urine output is slightly elevated. As the pregnant uterus compresses the bladder and reduces its capacity, urination becomes more frequent and some women experience uncontrollable leakage of urine (incontinence). Integumentary System the skin grows to accommodate expansion of the abdomen and breasts and the added fat deposition in the hips and thighs. Melanocyte activity increases in some areas and darkens the areolae and linea alba. Cardiac output rises about 30% to 40% above normal by 27 weeks, but for unknown reasons, it falls almost to the nonpregnant level in the last 8 weeks.
Generic clarinex 5 mg fast delivery
Sympathomimetic agents include substances such as cocaine allergy testing no antihistamines safe 5 mg clarinex, methamphetamine, epinephrine and dopamine. There is a subset of ExD-affected people who have sympathomimetic poisoning with malignant hyperthermia sometimes associated with elevated serotonin levels [4]. These cases have a grim prognosis and are at high risk of death regardless of police actions or method of subdual. This correlates well with published observations that mortality is about 67 per cent for those with a temperature above 41. Of course, if there is reasonable evidence that one or more specific forms of subdual or restraint did cause death, such cases can be so certified. In general, in these cases, any form of subdual should be considered a stress of a magnitude that is comparable to other components of subdual. Heat shock proteins are measured directly in frozen brain tissue taken from Brodmann area 22. The problem with these biomarkers is that they can only be measured in fresh or rapidly frozen brain. The restrainer uses both hands to pull backwards, and may injure the airway and compress the carotid arteries. The forearm of the restrainer is flexed at the antecubital fossa over the anterior neck; designed to compress the carotid arteries, not the airway. Bar hold (also known as the bar arm hold or choke hold) Carotid sleeper hold (also called variously the sleeper hold, carotid restraint or later vascular neck restraint) Shoulder pin restraint Neck holds Neck holds, commonly and incorrectly called choke holds, in various applications may cause lethal asphyxia by that form of restraint, rarely by airway constriction or by carotid artery compression [30,39]. In the context of neck compression, the critical structures are the airway, arteries and veins, bones (hyoid and cervical spine), nerves (vagus, spinal cord), tongue and cartilages. Carotid sinuses measure blood pressure; with hypotension, these receptors may increase cardiac output and cerebral blood flow via the autonomic nervous system. Compression of the carotid artery may cause stroke, and potentially death, particularly in the elderly, by interruption of adequate blood flow to the brain (in spite of the contribution from the vertebral arteries) or dislodgement of atherosclerotic plaques that embolize. Compression of one or both carotid sinuses may trigger either bradycardia or asystole. In view of these potentially lifethreatening hazards, Dick [7] and emergency medical specialists recommend use of the jaw thrust airway manoeuvre, which hyperextends the neck by using the hands on the jaws and is incapable of causing airway occlusion or vagal stimulation. Various types of neck hold have been used by police during attempted subdual, but most have fallen into desuetude because of the associated risks (Table 32. Because the risk of injury or death from the carotid sleeper is deemed by police to be less than the application of fists and batons, this form of restraint is considered appropriate for younger people. The theory of carotid sinus stimulation inducing bradycardia and asystole to date has rested on a matter of exclusion [15,16], as there is no anatomical expression at autopsy to support this pathophysiology, and there are no reports of death [30]. On a form of disease resembling some advanced stages of mania and fever, but so contradistinguished from any ordinary observed or described combination of symptoms, as to render it probable that it may be an overlooked and hitherto unrecorded malady. Frequency of signs of excited delirium syndrome in subjects undergoing police use of force: Descriptive evaluation of a prospective, consecutive cohort. Fatal excited delirium following cocaine use: Epidemiologic findings provide new evidence for mechanisms of cocaine toxicity. Cocaine-associated rhabdomyolysis and excited delirium: Different stages of the same syndrome. Factors associated with sudden death of individuals requiring restraint for excited delirium. Ventilatory and metabolic demands during aggressive physical restraint in healthy adults. Optimizing prone cardiopulmonary resuscitation identifying the vertebral level correlating with the largest left ventricle cross-sectional area via computed tomography scan. On the weight force used in chest compression in the prone position (Letter to editor). The effect of the prone maximal restraint position with and without weight force on cardiac output and other hemodynamic measures. The forensic pathologist has mainly to rely on the findings of the death scene investigation in conjunction with the external and internal findings of the body. In most cases the original scene has already been altered by the caretakers or other persons who recovered the child, thus demanding a careful reconstruction. It must be taken into consideration that a reconstruction can be stressful and traumatizing for the caretakers and therefore must be undertaken with empathy and thoughtfulness. External findings on the body may be subtle but are nonetheless of great importance. Petechial haemorrhages, abrasions, bruises, skin reddening (sometimes patterned) and distribution of postmortem lividity can guide the forensic pathologist to the reconstruction of the posture and to the cause of the asphyxia. Petechiae make it possible not only to deduce venous congestion but, by their topographic distribution, also to reconstruct the level in which the congestion occurred. However, like most findings in asphyxiation cases, facial petechiae are not specific for asphyxiation as such. They occur in different circumstances, some of which are not associated with accidents or violence Since mechanisms involved in suffocation do not necessarily lead to venous congestion, the absence of petechiae does not exclude asphyxiation. Autopsy findings in cases of asphyxiation depend largely on the underlying mechanism. Internal findings such as petechial haemorrhages of the serous layers, fluid blood, dilation of the right heart, cyanosis and congestion are also non-specific [6] and therefore must be evaluated taking into account the external findings and circumstantial evidence. Especially in cases of sudden and unexpected deaths of infants, the clear-cut differentiation between natural and non-natural death poses great difficulties for medicolegal experts. In contrast to older children, who often display the same physical signs of violent asphyxiation as adults One of the reasons is that it does not take a great physical effort to effectively close the breathing orifices of an infant, thus leading to no or minor external and internal injuries. Asphyxiation In principal, those mechanisms leading to asphyxiation in infants and children are the same as in adults. Causes of asphyxiation include obstruction of arterial blood supply to the brain Besides those mechanically influenced causes, sometimes referred to as external asphyxiation (although the nomenclature is not unambiguous, see Chapter 21), there are non-mechanical or internal causes, which occur in the young Even though there are no fundamental pathophysiological differences between the various forms of asphyxiation between children and adults, children are more prone to the risk of asphyxiation due to their relative physical weakness and the underdeveloped competence in recognizing potential hazards and acting properly. By detecting injury patterns, reconstructing individual accidents, and identifying previously unrecognized dangers, the forensic pathologist can be an important player in preventive medicine [4,13]. In England and Wales in a 2-yearperiod, 136 children died of mechanical asphyxia, 65 per cent of whom were under 3 years of age [23]. In an Australian study the annual rate of accidental asphyxiation in children under the age of 15 due to upper airway interference such as facial occlusion, head and neck entrapment, rope or cord strangulation or foreign body aspiration was 0. The most frequent cause of death in this study was strangulation due to ropes and cords. However, there have been other proposals on how to implement asphyxiation in the classification of sudden unexpected deaths in infancy [26]. A baby cannot oppose the perpetrator and therefore defensive injuries are frequently absent. Finally, even macroscopic and microscopic autopsy findings are often of minor value due to their limited specificity. Inevitably, these diagnostic challenges lead to a certain dark field of unrecognized infanticides, even if all sudden deaths in infancy undergo a meticulous autopsy (which is not the case in many jurisdictions). There are also fatalities of small children that are clearly attributable to accidental strangulation or positional asphyxia, sometimes raising the question of legal responsibility and consumer safety when transportation devices or restraint systems are involved. Obviously, any babies in potentially hazardous sleeping conditions remain at risk despite the success of prevention campaigns. The surroundings in which the infant is recovered often suggests a mechanical asphyxia. In these cases, it is not always possible to reconstruct the original situation accurately, because the original scene has often been changed by the person recovering the baby. Often it remains unclear whether the mouth and nose were covered or closed by the body of a co-sleeping person, bed clothing or the back rest of the sofa. Arrangement and blanching of postmortem lividity can be helpful in cases with a postmortem interval of at least several hours before discovery of the dead baby, thus leaving enough time for the lividity to be fixed in adjacent body parts.
Cheap clarinex online visa
With regard to the circumstances elucidated by the police investigation allergy shots better than pills purchase clarinex cheap, the manner of death was determined to be suicide. Toxicological analysis of the blood demonstrated therapeutic concentrations of oxazepam. It was concluded from the toxicological findings that the deceased had access to cyanide, had ingested the substance orally, and had died of cyanide intoxication. Case 5 the deceased was a 29-year-old woman who worked as a laboratory technician in a metal-processing factory. After having a cappuccino with her colleagues, she experienced seizures and collapsed. Because no organic disease that could have caused the seizures was diagnosed, the workplace was taken into consideration, and the suspicion of intoxication arose. Four hours after the woman was admitted to hospital, specimens of blood and stomach contents were obtained for toxicological examination. The police investigation disclosed that a male colleague had fetched the cappuccino from an automated buffet in the factory. According to witnesses, the drink had had a pungent putrid odour resembling ammonia and a bitter disgusting taste. Because the deceased was reported to have drunk only a sip of the cappuccino, and furthermore had access to cyanide in her professional work, the manner of death was assumed to be suicide. Several months later, the colleague who had passed the cappuccino to the deceased was suspected of having poisoned the woman by means of a lethal dose of cyanide. He was convicted of murder and sentenced to long-term imprisonment on the basis of circumstantial evidence, i. Case 4 According to the report of the police investigation, the 70-year-old wife of a chemist had experienced depression, had had serious financial problems in the family, and had several times announced the intent to commit suicide. When she was found a few minutes later and admitted to having consumed the powder, her husband instantly suspected sodium cyanide. The woman experienced convulsions and, despite immediate attempts at resuscitation, died approximately 2 hours later. Autopsy showed severe coronary atherosclerosis with significant luminal narrowing caused by fibrofatty plaques and two surgically implanted aortocoronary bypass vessels, but no complete occlusion and no recent myocardial infarction. The gastric mucosa did not show a striking haemorrhagic appearance, erosions or ulcers. The cause and manner of death could not be determined unequivocally at gross examination. Thus, cases have been reported in which patients experienced the symptoms of cyanide poisoning hours after the ingestion of acetonitrile-based artificial nail polish remover [35,118,171]. Cyanide compounds have a faint, bitter almond odour, detectable at a threshold of 0. The ability to smell cyanide is a genetically determined trait that is absent in up to 50 per cent of the population. Cyanide may be released from various compounds by chemical reactions or by pyrolysis. Significant blood cyanide levels have been found in many fatal and non-fatal cases of fire-related smoke inhalation [17,104], and the risk of cyanide intoxication due to smoke inhalation injury is probably underestimated. As for other sources of cyanide, cigarette smokers have been found to have mean whole blood cyanide levels of approximately 0. Natural sources of cyanide include amygdalin and similar cyanogenic substances found in a wide variety of plants [70,126]. After absorption, cyanide is rapidly distributed by the blood circulation throughout the body. The blockade of the cytochrome oxidase system causes anaerobic metabolism, which results in lactate production and severe metabolic acidosis. Cyanide also inhibits other enzymes and can combine with certain metabolic intermediates. Eighty per cent of absorbed cyanide is detoxified in the liver by the mitochondrial enzyme rhodanese, which catalyzes the transfer of sulfur from a sulfate donor to cyanide, forming less toxic thiocyanate, which is rapidly excreted in urine. Other detoxification pathways include reaction with hydroxycobalamin (vitamin B12b) to form cyanocobalamin (vitamin B12). Acute cyanide poisoning results primarily in central nervous system effects with early stimulation, which is quickly followed by depression. Early symptoms include lightheadedness, giddiness, tachypnoea, nausea, vomiting, suffocation, confusion, restlessness and anxiety. These changes may be followed by hypoventilation, progressing to apnoea and myocardial depression. The predominance of anaerobic metabolism induces a decrease in the adenosine triphosphate/adenosine diphosphate ratio and alters energy-dependent processes such as calcium homeostasis. The onset of symptoms may be delayed up to 12 hours after the ingestion of cyanogenic glycosides, nitriles or thiocyanates. In summary, the signs and symptoms of acute cyanide toxicity reflect cellular hypoxia and may initially be non-specific, generalized and nondiagnostic. Cyanide should be included in the differential diagnosis of rapid onset of coma and, in particular, when coma and metabolic acidosis appear together. The treatment of cyanide poisoning begins with removing the patient from exposure, administering 100 per cent oxygen, and giving aggressive cardiorespiratory support and an antidote. Inhalation of amyl nitrite has been recommended as a first-aid measure, followed by the intravenous administration of sodium nitrite and/or sodium thiosulfate. Nitrites induce methaemoglobinaemia, which detoxifies cyanide by forming cyanomethaemoglobin. Thiosulfate serves as a sulfur donor in the rhodanesecatalyzed conversion of cyanide to less toxic thiocyanate. Blood cyanide levels are useful in confirming the diagnosis of intoxication, but therapeutic interventions must usually be initiated before the results of analysis are available. Especially in forensic cases, an accurate assessment of the duration of the ability to act after lethal cyanide poisoning can be of crucial importance in reconstructing the cause of poisoning. Subjects with cyanide intoxication may be able to give a report about the incident, remove a poison container, or walk for a few hundred metres. Nevertheless, factors such as age, body mass, state of health, and mode of ingestion may influence these values, and survival after the ingestion of larger quantities has been reported. In comparison with these published data, the blood cyanide levels in our cases (3. Important for the interpretation of toxicological findings is the fact that cyanide levels may drop as a result of degradation of cyanides into less toxic components if the postmortem interval prior to autopsy is too long [15,16]. Thus, in fatalities suspected to result from cyanide poisoning, the autopsy and toxicological analysis should be performed as soon as possible after death. Postmortem endogenous cyanide formation in tissue is less important, because the amounts formed are not significant. Indicative circumstances of cyanide poisoning Most cases of occupational cyanide poisoning are easily recognized because of the known circumstances. In professional persons having access to cyanide, the history often indicates the correct direction of the investigation. Recent reviews concerning cyanide-related deaths have suggested that the suicidal use of substances is usually limited to specific occupational groups (Table 18. In Case 1 here, however, the circumstances of the scene and in particular the initial death certificate had focused attention on the evidence that suggested an accidental fall, so that investigation of the history and examination of the locus with regard to intoxication was neglected. Nevertheless, the autopsy findings and laboratory tests in association with the evidence discovered subsequently were in keeping with one another and left no reasonable doubt that the manner of death was suicide. In agreement with the literature, the individuals involved in these five fatalities, without exception, had cyanide at their disposal. The goldsmith in Case 1 and the accused in the homicide Case 5 had professional access, as evidenced by the special ingredients found at their workplace. The double suicide using so-called suicide pills was committed by a physician and his wife. Toxicological findings Whole blood cyanide levels are higher than plasma levels because of the concentration of cyanide in the red blood cells. Correlation of symptoms to whole blood levels is misleading because the effect of cyanide depends on the intracellular concentration at the cytochrome oxidase binding sites and the duration of poisoning. According to Baselt and Cravey [18], the minimal lethal dose has been estimated to be 100 mg for 18 Homicide Table 18. Unlike the characteristic and easily detectable pink hypostasis of carbon monoxide poisoning, the bright pink or lilac colouration ascribed to cyanide poisoning is difficult or impossible to detect at autopsy.
