
Discount super avana 160 mg visa
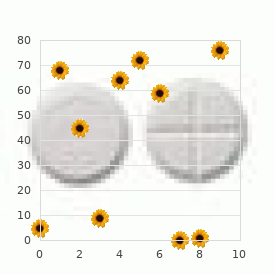
The sensitivity of a test is the percentage of all patients with the condition who have a positive test erectile dysfunction in teens discount super avana 160mg. Thus, the specificity and sensitivity can be calculated as follows: Specificity (%) = True Negatives *100 True Negatives + False Positives In an ideal setting, there would be no overlap between a normal and a disease population. Often there is a compromise between sensitivity and specificity when setting a cutoff value. Take the example of a normal and a disease population in which there is significant overlap between the populations for the value of a test. Left, When a test is applied to a population of normal patients, the test will correctly identify all normal patients who are below the cutoff value as normal (true negative [green]); however, it will misidentify a small number of normal patients who are above the cutoff value as abnormal (false positive [yellow]). Right, When a test is applied to a disease population, the test will correctly identify all abnormal patients who exceed the cutoff value (true positive [red]); however, it will misidentify a small number of abnormal patients who are below the cutoff value as normal (false negative [dark blue]). Left, Ideally, there would be no overlap between a normal (green) and a disease (red) population, and the cutoff value could be placed between the two populations, yielding 100% sensitivity and 100% specificity. Right, In biologic populations, there is always some overlap between normal and disease populations. Left, If the cutoff value is set low (high sensitivity), the test will correctly diagnose nearly all the abnormals correctly (true positives [red]) and will misidentify only a few as normal (false negatives [dark blue]). In this case, some normals will be identified as normal (true positives [green]), but a high number of normal patients will be classified as abnormal (false positives [light blue]). Left, If the cutoff value is set high (high specificity), the test will correctly identify nearly all of the normals correctly (true negatives [green]) and will misidentify only a few normals as abnormal (false positives [light blue]). Here, some abnormal patients will be identified as abnormal (true positives [red]), but a high number of abnormal patients will be classified as normal (false negatives [dark blue]). Although both are important, type I errors are generally considered more unacceptable. Thus, the specificity of a test should take precedence over the sensitivity, unless the test is being used as a screening tool alone. Asthecutoffvalueis lowered, the sensitivity increases but at a significant cost to the specificity. The graph demonstrates the tradeoff between sensitivity and specificity for various test values of the D4 study. A Bayesian argument against rigid cutoffs in electrodiagnosis of median neuropathy at the wrist. The chance of a positive test being a true positive is markedly higher in a population with a high prevalence of the disease. In contrast, if a very sensitive and specific test is applied to a population with a very low prevalence of the disease, most positive tests will actually be false positives. In both examples, the same test with a 95% sensitivity and a 95% specificity is applied toapopulationof1000patients. The predictive value of a positive test is defined as the number of true positives divided by the number of total positives. Thus,inthisexample, in which the disease prevalence in the population is high, a positive test is extremely helpful in correctly identifying the patient as having the disease. In this setting, in which the disease prevalence in the population is low, a highly sensitive and specific test is of absolutely no value. If the patient has pain in the wrist and hand, paresthesias of the first four fingers, and symptoms provoked by sleep, driving, and holding a phone, the prevalence of carpal tunnel syndrome in patients with such symptoms would be extremely high. However, if the same tests are performed on a patient with back pain and no symptoms in the hands and fingers, the prevalence of carpal tunnel syndrome would be low in such a population. In this situation, any positive finding would have a high likelihood of being a false positive and would likely not be of any clinical significance. Less well appreciated is that the problem of a false positive in a population with a low prevalence of disease can be overcome by making the cutoff value more stringent. For this nerve conduction study, the latency for the ulnar palm-to-wrist segment is subtracted from the latency for the median palm-to-wrist segment, using identical distances. In patients with carpal tunnel syndrome, the median latency is expected to be longer than the ulnar latency. When the appropriate tests are applied for the appropriate reason, any positive test is likely to be a true positive and of clinical significance. After your history and examination, youthinkthereisabouta50%probabilitythattheyhave anulnarneuropathyattheelbow(50%isthepre- est t probability). With a positive test, the probability that the patient truly has the diagnosis of ulnar neuropathy at the elbow rises to 95% (this is the post-test probability). After your history and examination, youthinkthereisabouta50%probabilitythatthey have an ulnar neuropathy at the elbow. You then perform a diagnostic test that has a different sensitivity and specificity than the example above, and it is positive for ulnar neuropathy. However, with this particular diagnostic test, the probability that the patient truly has the diagnosis of ulnar neuropathy at the elbow now only rises to 55%. Why does one positive test increase the likelihood (posttest probability) that the patient has the disease to 95% and theothertoonly55% When a diagnostic test is performed, the reason that it is done is to help determine if the disease or condition is truly present. Conversely, if one thinks the probability that the patient has the condition is extremely low. Thus, testing is usually done when one thinks the diagnosis is possible but not certain. The Fagan nomogram is a powerful tool in assessing the value of a positive test when the likelihood ratio is known. The pre-test probability is estimated, and a point placed on the left y-axis; the likelihood ratio is plotted on the middle y-axis. A line is then drawn connecting these two points and carried over to where it intersects the right y-axis. The most common situation occurs in the electrodiagnosis of median neuropathy at the wrist. Itisnotuncommon that a single test is above or below the cutoff range and, in nearly every case, represents a false positive. Fortunately, there is a relatively simple remedy to this problem of multiple tests and the increasing risk of false positives. In the graph to the left, the cumulative false-positive rate is calculated based on the assumption that only one test needs to be abnormal to diagnose the condition. Incontrast,thestatisticschange significantly if two or more tests are required to be abnormal to diagnose the condition. In the graph to the right, if 10 tests are done, each with an individual false-positive test rateof2. Right, If two or more tests are required to be abnormal before a diagnosis is reached, the statistics change. Be very cautious about making any diagnosis based on onlyonepieceofdata;ifthatpieceofdataisinerror,it will be a false-positive. A Bayesian argument against rigid cut-offs in electrodiagnosis of median neuropathy at the wrist. Incarpaltunnelsyndrome,thereisareversal of this pattern, with relative slowing of the wrist-topalm segment (see Chapter 20). Agoodruleofthumb:thecurrentneeded above the elbow is typically about one-half of that neededatthebelow- lbowsite. Ifpalm stimulation results in baseline distortion due to stimulus artifact, the anode should be rotated until a suitable baselineisobtained. Ifonlythewristandabove- lbowstimulae tions are performed, one can miss ulnar slowing across theelbow. Inrarepatients,there is an anomalous innervation wherein the entire dorsum of the hand is supplied by the superficial radial nerve instead of a combination of the superficial radial and dorsalulnarcutaneousnerves. Stimulation site slightly proximal to the ulnar styloid, recording in the web space between the fourth and fifth fingers. Recording the first dorsal interosseous muscle (stimulation sites are the same as the routine ulnar motor studies recording the abductor digiti minimi muscle). Ifonlythewristandabove- lbow e stimulations are performed, one can miss ulnar slowing acrosstheelbow. Ifthisisseen,marktheonset latency after this mixed potential at the onset of the motorpotential.
160mg super avana with visa
For example erectile dysfunction herbal treatment effective super avana 160mg, when you see a bolt of lightning and then hear the thunder 5 seconds later, you can use this simple formula to calculate how far away the lightening is from you. One knows that the lightening was approximately 1 mile away as 1 mile is 1609 meters. In some cases, it simply continues through that tissue and is eventually absorbed as heat. Indeed, there are therapeutic (as opposed to diagnostic) ultrasound devices that are purposely used to create heat deep in tissues, for therapeutic purposes. These echoes are then transmitted back to the piezoelectric elements in the probe to be converted back to electrical energy. Thus, echoes are created when sound waves encounter a boundary of two dissimilar tissues. The strength of the echo increases as the difference between the two acoustic impedances increases. Accordingly, if there is a marked difference in impedance between two tissues, very strong echoes occur. Conversely, if there is little difference between two adjacent tissues, very weak or no echoes occur. If the echoes are directed back toward the probe, they will reach the probe and can be recorded. Information from both the location (depth) of the tissue creating the echoes and the intensity (brightness) of the returning echoes helps create the ultrasound image. Because the sound wave must travel to the tissue that created the echo and back, the time at which the echo occurs represents twice the distance to the tissue. Again, this is important as the ultrasound image is created based on the distance traveled and the intensity of the echo. However, if the tissue is at an angle to the sound wave, it can reflect the echo back in a different direction and may never reach the probe. If the boundary where the echo is created is irregular, echoes can scatter in many different directions. This back scattering results in "speckle" of the ultrasound image, which can interfere with echoes of interest. The height of the spike corresponds to the strength of the echo, and the time of the spike correlates to the depth of the tissue that creates the echo. To create an image, ultrasound probes contain hundreds of piezoelectric elements that are arranged in a row. Thus, hundreds of individual lines of ultrasound information are recorded simultaneously, which can be stitched together digitally to create a grayscale image. Top, Ultrasound transmitting a single pulse through a hypothetical structure that contains several different tissues. Bottom, the signal recorded from the returning echoes formed when the ultrasound pulse encounters a boundary between two different tissues. The fundamental building block of ultrasound is one piezoelectric element transmitting and recording information. This results in a single line of ultrasound information displayed on an oscilloscope, known as amplitude mode (A-mode) ultrasound. The height of the spike corresponds to the strength of the echo, and the time of the spike correlates to the depth of the tissue that created the echo. In this figure, the first large spike corresponds to the echo created by the tissue represented by the curved black line in the top figure; the second and third spikes represent the green boundaries; echoes in between represent the intervening tissues. One specific index line of ultrasound is selected (line designated by the green arrow). The bright line behind the liver is the echo created from the diaphragm (red arrow). To create an image, ultrasound probes contain hundreds of piezoelectric elements that are arranged in a row (blue elements). These elements record individual lines of ultrasound information that are stitched together digitally to create a grayscale image. Probes contain other layers and materials that couple (orange layer) and focus (green layer) the ultrasound beam in addition to dampening undue vibrations (yellow layer). The cable coming from the ultrasound probe is very large because of all the individual wires needed for the many piezoelectric elements. They are continually sending out sound waves and then turning off, waiting to receive echoes back. Indeed, most of an ultrasound cycle is spent with the elements in the receiver mode. M-mode is most useful in looking at tissue movement (as in cardiac function, or in movement of the diaphragm). In the M-mode trace (bottom image), it is actually A-mode information from the index line (amplitude and depth) that is recorded over time. The bright line in the bottom image is the echo created from the diaphragm, in this case showing its movement over time (bottom image, red arrow). M-mode is most helpful in neuromuscular ultrasound when assessing muscle movement over time. For example, a useful measure of diaphragmatic function is to use M-mode neuromuscular ultrasound to measure diaphragmatic excursion over time during inspiration and expiration. In contrast, the curvilinear probe has a lower resolution but is able to visualize deeper tissues. This probe is used to look at small structures, especially those very close to the surface. Because of its small footprint, it is also very useful around body areas that are uneven or have bony protuberances. Curvilinear probes are used when studying very deep structures, such as the sciatic nerve at the gluteal fold and especially the diaphragm behind the liver. Note that there are fairly significant differences in the frequencies of these different probes. The higher the frequency, the greater the attenuation of the image as the wave travels through tissue. At greater depths, one needs to lower the frequency of the probe being used or use a probe with a lower frequency such as the curvilinear probe. Hence, for example, abdominal ultrasound is done with curvilinear probes (which have much lower frequencies), as much greater depths are needed. The most common include the linear probe, the high-frequency "hockey-stick" probe, and the curvilinear probe. Much of the bottom image is taken up by black areas below the area of interest, where the ultrasound beam has been completely attenuated. The ultrasound beam can be focused at a particular depth (focal point) to best see images at that depth. It does not change the power of the ultrasound waves sent out but more or less amplifies the returning echoes. The brightness setting should be adjusted so that the image is neither washed out (middle image) nor too dark (bottom image) such that important details cannot be seen. When the correct adjustment is reached, all the important details are best seen (top image). Air has an incredibly high acoustic impedance through which ultrasound waves cannot travel. The probe should be held lightly against the skin, as too much pressure will displace the underlying gel. Similar to a camera, the ultrasound machine can focus the sound waves at a particular depth, called the focal depth, to best see images at that depth. However, the downside of setting increased numbers of focal depths is that it decreases the frame rate (the rate at which the image refreshes itself). The brightness setting does not change the power of the ultrasound waves sent out, but more or less amplifies the returning echoes. The brightness setting should be adjusted so that the image is neither washed out nor too dark such that important details cannot be seen.

Super avana 160 mg sale
In addition to the peroneal motor and sensory studies erectile dysfunction from adderall purchase super avana visa, tibial motor, F response, and sural sensory studies must be performed. Because lesions of the sciatic nerve and lumbosacral plexus can present in a similar manner to peroneal neuropathy, excluding a more widespread lesion is imperative. Of course, if any motor or sensory study is borderline, comparing it with the contralateral asymptomatic side often is useful. In such cases, interpretation of the nerve conduction studies can be more difficult. The sensory response, which is mediated by the superficial branch of the peroneal nerve, will be normal. If peroneal motor studies show evidence of axonal loss only, without focal slowing or conduction block across the fibular neck, the nerve conduction studies in an isolated deep peroneal neuropathy may appear identical to those seen in a severe L5 radiculopathy associated with axonal loss. When performing peroneal motor studies, recording the tibialis anterior often is more informative than routine studies recording the extensor digitorum brevis. In some cases of peroneal neuropathy at the fibular neck, conduction block may be seen recording the tibialis anterior but not the extensor digitorum brevis. In the traces shown here, the tibialis anterior and extensor digitorum brevis are corecorded while the peroneal nerve is stimulated below the fibular head and at the lateral popliteal fossa. Note the conduction block pattern recording the tibialis anterior but not the extensor digitorum brevis. The studies are from a patient with an occupational peroneal palsy across the fibular neck due to repetitive squatting. If any of the peroneal-innervated muscles are abnormal, non-peroneal-innervated muscles supplied by the L5 root must be sampled to exclude a sciatic neuropathy, lumbosacral plexopathy, or radiculopathy. Note that even if the conduction studies localize the lesion to the peroneal nerve at the fibular neck (focal slowing or conduction block), a few critical non-peroneal L5-innervated muscles still should be sampled to confirm that the lesion is restricted to the peroneal nerve and to exclude a superimposed lesion. Tibialinnervated muscles are sampled next, especially the tibialis posterior, which is an L5-innervated muscle that mediates ankle inversion. If any abnormalities are found in these muscles, an isolated lesion of the common peroneal nerve has been excluded. The short head of the biceps femoris has an important role in suspected peroneal neuropathy at the fibular neck. It is the only muscle supplied by the peroneal division of the sciatic nerve that originates above the fibular neck. Abnormalities in this muscle or in any of the hamstring muscles imply a lesion proximal to the peroneal nerve, in the sciatic nerve or higher. The short head of the biceps femoris can easily be sampled four fingerbreadths above the lateral knee, just medial to the tendon to the long head of the biceps femoris. The peroneal F responses are generally prolonged or absent on the symptomatic side, with normal peroneal F responses contralaterally and in the tibial nerve. Tibial- and sciatic-innervated muscles are spared, especially the tibialis posterior, flexor digitorum longus, and the short head of the biceps femoris. The presence of a predominantly demyelinating lesion has important prognostic implications. Because the underlying axons remain intact, the prognosis for full recovery over a relatively short period is excellent, provided that the cause of the entrapment is no longer present. Despite being quite large, it is deep and often ill-defined on short axis imaging. To visualize the peroneal nerve, the patient can either lie prone on the bed with their lower legs propped up on a pillow or they can lie on their side facing away from the examiner, with the abnormal side up, and with their knees and ankles together (lateral decubitus position). The prone position is easier for the ultrasonographer and allows for an easy comparison to the contralateral side. However, it is not as comfortable for the patient, and patients who are disabled may have difficulty getting into this position. The lateral decubitus position is much easier for the patient but does not allow for sideto-side comparison unless the patient changes position, and it may be more difficult to visualize structures in the popliteal fossa. The popliteal fossa is behind the knee and has a diamond shape, bordered by the medial and lateral hamstrings (superiorly) and the medial and lateral gastrocnemius muscles (inferiorly). Near the superior apex of the popliteal fossa, it joins the popliteal vein and artery. Bottom, Same image with the peroneal nerve in yellow and bony margin of the fibular head in green. Past the knee joint, the bony shadow of the large fibular head is seen, immediately adjacent to the peroneal nerve. Bottom, Same image with the peroneal (P) and tibial (T) nerves in yellow, the popliteal vein in blue, and the popliteal artery in red. The distal sciatic nerve, despite being quite large, is often ill-defined on short axis imaging in the popliteal fossa. However, when it divides into the common peroneal and tibial nerves, this can usually be well seen on ultrasound. To bring the common peroneal and tibial nerves into view at the popliteal fossa, one should repetitively move the probe back and forth (distal and proximal). Indeed, any time the common peroneal nerve is larger than the tibial nerve in the popliteal fossa, it is abnormal. Just after its origin from the sciatic nerve, the common peroneal nerve immediately moves laterally and more superficially. The tibial nerve continues on a more or less straight course into the distal popliteal fossa accompanied by the popliteal vein and artery below it. In the very proximal calf, the medial sural cutaneous nerve can sometimes be seen arising from the tibial nerve. The common peroneal nerve continues to move laterally, under the tendon of the long head of the biceps femoris and the short head of the biceps femoris muscle. As it passes the fibular neck, the nerve moves anterior to wrap around the fibular neck in the "fibular tunnel" (the tunnel created by the peroneus longus muscle and its tendon originating from the fibular head). As it moves anterior, the common peroneal nerve divides into its superficial and deep branches. The deep branch, as its name implies, quickly moves deep to join the anterior tibial artery next to the interosseous membrane to innervate the ankle and toe dorsiflexor muscles. It is very difficult to visualize the deep peroneal nerve with ultrasound past the fibular neck. Back at the mid-popliteal fossa, the lateral sural cutaneous nerve can sometimes be seen arising from the common peroneal nerve. The medial and lateral sural cutaneous nerves merge and run in the calf as the sural nerve between the medial and lateral heads of the gastrocnemius muscle, usually accompanied by the lesser saphenous vein. Using this protocol, a useful starting position is to place the probe in long axis directly over the proximal fibula with the patient in the lateral decubitus position. Bottom, Same image with the superficial peroneal nerve in yellow and extensor digitorum longus (left side) and peroneus longus/brevis (right side) in red. The superficial peroneal nerve becomes subcutaneous distally in the lower leg in the groove between the extensor digitorum longus and the peroneus longus/brevis muscles. Bottom, Same image with the sural nerve in yellow, lesser saphenous vein in blue, and medial and lateral heads of the gastrocnemius in red. With the probe placed in the midline between the bellies of the medial and lateral gastrocnemius muscles, the sural nerve can be seen. It is small and contains only a few fascicles and is usually accompanied by the lesser saphenous vein nearby. Bottom, Same images with the bony outline of the fibular head and neck in green, the peroneal nerve in yellow, and the peroneus longus muscle in red. Proximally, the fibular neck enlarges into the fibular head with the peroneus longus muscle directly above. The fibular head/neck is easily seen, with the common peroneal nerve directly behind. As noted earlier, external compression at the fibular neck is the most common cause of peroneal neuropathy. Similar to other entrapments, the common peroneal nerve may be large and hypoechoic with loss of its normal fascicular architecture proximal to the entrapment site. Interestingly, when this group of patients with a pure demyelinating lesion is studied with ultrasound, many are normal! Indeed, ultrasound abnormalities of the peroneal nerve at the fibular neck, including an enlarged cross-sectional area and abnormal fascicular structure, correspond more to axonal loss lesions, or demyelination with secondary axonal loss.
Order 160mg super avana free shipping
Providing every child in the world with clean drinking water and food free from bacteria is a primary goal in prevention erectile dysfunction devices diabetes order 160 mg super avana amex. X Description Rubeola (formerly known as hard or red measles) is a highly communicable respiratory infection. The disease is most common in school-age children, with outbreaks occurring in the winter and spring. The disease is less common in the United States, but from January to May 2014, 187 cases were reported in 15 outbreaks. Infectious and Communicable Diseases 71 Etiology Rubeola is caused by the Morbillivirus rubeola virus through direct contact with infectious droplets and occasionally through the air. Small red spots with bluish white centers, called Koplik spots, appear on the oral mucosa by the second or third day. The rash first appears on the face as tiny maculopapular lesions that contain both discolored spots of skin called macules and red, raised areas of skin called papules. The lesions may be so densely clustered in certain areas that the skin surface appears generally swollen and red. Diagnostic Procedures the clinical picture of symptoms is usually a sufficient basis for a diagnosis of rubeola. Blood testing may reveal an abnormal decrease in the number of circulating white blood cells, or leukopenia, and antibody titers are used to detect the presence of measles antibody in both the acute and convalescent phases. Bed rest is indicated, sometimes in a darkened room to alleviate the discomfort of photophobia. Prevention Active immunization can be produced by administration of a vaccine, preferably containing the live attenuated virus. The increase in incidence in the past few years is the result of children not receiving vaccinations as well as increased international travel, which is increasing the rate of exposure. Rubeola can be prevented within 5 days of exposure by administration of gamma globulin, a protein formed in blood that functions as an antibody to provide rapid, temporary immunity to the disease. Hand washing and discarding tissues contaminated with respiratory secretions may help prevent the spread of measles within a family. It closely resembles rubeola, but it differs in its short course, mild fever, and relative freedom from complications. Educate caregivers about the incubation period, the spread of infection, and how to handle bedding, discarded tissues, and dishes. Prognosis Rubeola is usually a benign disease, running its course in about 5 days after the rash appears. Signs and Symptoms the onset of the disease is sometimes characterized by malaise, headache, slight fever, and sore throat. It may be composed of pale red, slightly elevated, discrete papules, or the rash may be highly diffuse and bright red. The rash begins on the face, spreads rapidly to other portions of the body, and usually fades so rapidly that the face may clear before the extremities are affected. Diagnostic Procedures Because rubella can be easily confused with other diseases, a definitive diagnosis can be reached with cultures of the throat, blood, and urine or with antibody titers. A culture of urine with antibody titers is generally done in the acute and convalescent phases. Prevention Lasting immunization can be conferred through use of a live rubella vaccine. Administration of gamma globulin shortly after exposure may prevent development of the disease, but it still may not prevent transfer of the virus to the fetus if exposure occurs during pregnancy. Prevention includes good hand washing and disposing of tissues contaminated with respiratory secretions. X Description Mumps is an acute contagious disease characterized by fever and inflammation of the parotid salivary glands. The disease is most common among children and young adults in late winter and spring. Etiology the disease is caused by the mumps paramyxovirus, which has an incubation period of 18 days. Signs and Symptoms the classic symptoms of mumps are unilateral or bilateral swollen parotid glands. Headache, malaise, fever, and earache may occur, and other salivary glands may become swollen. Diagnostic Procedures the clinical picture of mumps and a history of recent exposure usually are sufficient for diagnosis. Because many clients are asymptomatic, teaching opportunities may be limited; however, it is a good idea to encourage clients to eat a balanced diet and drink ample fluids. The disease is benign, seldom produces complications, and runs its course in 3 days. Rubella is dangerous, however, when it occurs in pregnant Infectious and Communicable Diseases 73 Complementary Therapy No significant complementary therapy is indicated. Complications can occur, however, and include orchitis, pancreatitis, and various central nervous system manifestations. Orchitis, which causes swelling of the testes in adult men, is extremely uncomfortable but rarely causes sterility, as is often feared. Good hand washing and proper disposal of contaminated tissues is essential for prevention. Etiology the disease is caused by the varicella-zoster virus, which is a herpesvirus. Its incubation period is 2 to 3 weeks, usually between 13 and 17 days, and is spread via respiratory secretion and direct contact. Signs and Symptoms the sign of chickenpox is a pruritic rash, which begins as erythematous macules that produce papules and then clear vesicles. The rash usually contains a combination of papules, vesicles, and scabs in all stages. Diagnostic Procedures the clinical signs are usually sufficient for the diagnosis. Treatment Isolation is important during the infectious period- usually until all the scabs disappear. Calamine lotion, cool bicarbonate of soda, or colloidal oatmeal baths can be very helpful. Complementary Therapy No significant complementary therapy is indicated other than oatmeal baths, as suggested previously. The disease occurs most commonly among children and may occur in epidemic outbreaks. Chickenpox requires strict adherence to proper hand washing, disposal of tissues, and proper cleaning of bedding and clothing. Teach clients or caregivers how to apply any lotions or medications to alleviate itching. Do not give children aspirin-containing products because of its link to Reye syndrome. Complications may include secondary bacterial infections of the skin as a result of scratching open lesions, thrombocytopenia, arthritis, hepatitis, and Reye syndrome. After a varicella infection, the virus can remain inactive in nerve cells near the spinal cord and reactivate later as shingles. Shingles can cause tingling, itching, and pain followed by a rash of red bumps and blisters. Anyone who has not had chickenpox can catch it from someone with shingles, but they cannot catch shingles. In certain situations, varicella-zoster immune globulin may be administered within 72 hours of exposure to stop the development of the disease. Good hygiene, including proper disposal of tissues contaminated with respiratory secretions, is important. It is called fifth disease because it was classified in the late 19th century as the fifth in a series of six childhood exanthems- rashes that occur on the skin as opposed to rashes that occur on the mucous membranes (or enanthems). Etiology Fifth disease is caused by the human parvovirus B19 (this not the same parvovirus pets may get) and is transmitted through respiratory secretions or direct contact. Parvovirus B19 can be transmitted during therapy with clotting factor concentrate. It is most prevalent in elementary and junior high school children during winter and spring.
Best order super avana
InsuspectedC8 radiculopathy erectile dysfunction estrogen proven 160 mg super avana, these should be performed bilaterally if the results are abnormal or borderline on the symptomatic side. Be sure to exclude peroneal palsy at the fibular neck, especially in suspected L5 radiculopathy. It is best to perform these studies bilaterally if the amplitude on the symptomatic side is low or borderline. Itisbesttoperform these studies bilaterally if the results are abnormal or borderline on the symptomatic side. The distal latency prolongation and conduction velocity slowing, however, should never drop into the demyelinating range. Sensory studies are the most important part of the nerve conduction studies in the assessment of radiculopathy. For instance, if a patient has pain down the arm with tingling and paresthesias of the middle finger, the median sensory response to the middle finger should be checked. In axonal loss lesions, both proximal and distal to the dorsal root ganglion, degeneration of motor fibers results in decreased compound motor action potential amplitudes. If larger motor fibers are lost, conduction velocities and distal latencies also may slow slightly. Lesions proximal to the dorsal root ganglion result only in degeneration of sensory fibers proximally into the spinal cord. Because the dorsal root ganglion is a bipolar cell, it remains in continuity with the distal sensory fibers. In axonal loss lesions at or distal to the dorsal root ganglion, distal sensory fibers degenerate, as do the motor fibers. Herniated intervertebral discs are a common cause of cervical and lumbosacral radiculopathy. Herniated discs are most often lateral and posterior, with the dorsal root ganglion located distal to the herniation. In disc herniations, this anatomic relationship results in injury to the roots but sparing of the dorsal root ganglion and the peripheral sensory nerves. This discrepancy may be explained by the fact that in cadaver studies, some L5 dorsal root ganglia are found indented by the superior facet. In contrast, there is no facet joint that frames the intervertebral foramen for the S1 root. If possible, sample at least two muscles in each of the following areas: paraspinal, proximal, and distal limb. In each limb area, try to use muscles with similar root innervation but different peripheral nerve innervation. If abnormalities are found, examine muscles in adjacent myotomes, above and below the suspected lesion level, to exclude a more widespread or diffuse lesion. If findings are mild or equivocal, compare with a contralateral asymptomatic muscle. In the post-spinal surgery setting, fibrillation potentials in the paraspinal muscles do not necessarily have diagnostic significance; thus, they are not helpful to sample. It is important to exclude a mononeuropathy, polyneuropathy, or more diffuse process that might account for the signs and symptoms. Muscles innervated by the same myotome but by different nerves must be sampled to exclude a mononeuropathy. However, because each of these muscles is also innervated by the radial nerve, one could not differentiate between a radial neuropathy and a C7 radiculopathy by sampling only these muscles. Since all these muscles have C7 innervation in common, despite different peripheral nerve innervations, this pattern of abnormalities points toward a radiculopathy as the lesion. Note that while nearly all muscles are innervated by multiple myotomes, certain muscles are predominantly innervated by one myotome, and these muscles are the most useful in the electrodiagnosis of radiculopathy (Tables 32. Proximal and distal muscles that are innervated by the same myotome should be sampled to exclude a distalto-proximal pattern of abnormalities such as occurs in polyneuropathy. However, because these are all distal muscles, one could not exclude a typical distal polyneuropathy, especially if the sural sensory potential is borderline low. Muscles innervated by myotomes above and below the suspected lesion level must be sampled to exclude a more widespread or diffuse process. Examination of the paraspinal muscles is crucial in the evaluation of radiculopathy. The paraspinal muscles are innervated by the dorsal rami, which arise directly from the spinal nerves. Neuropathic abnormalities in these muscles nearly always imply a lesion at or proximal to the nerve roots. Other than the presence of normal sensory nerve conduction studies, abnormalities in the paraspinal muscles are the only other finding that can conclusively differentiate radiculopathy from plexopathy. Unfortunately, the paraspinal muscles are affected in only about 50% of cases of radiculopathy. Thus, the absence of paraspinal abnormalities cannot exclude a radiculopathy; however, the presence of paraspinal abnormalities clearly localizes the lesion to the root or anterior horn cell level. C5 Dorsal scapular nerve Rhomboid major/minor Suprascapular nerve Supraspinatus Infraspinatus Axillary nerve Deltoid Musculocutaneous nerve Biceps brachii Median nerve Pronator teres Flexor carpi radialis Flexor pollicis longus Abductor pollicis brevis Ulnar nerve Flexor carpi ulnaris Flexor digitorum profundus (V) Abductor digiti minimi First dorsal interosseous Radial nerve Triceps Brachioradialis Extensor carpi radialis Extensor digitorum communis Extensor carpi ulnaris Extensor indicis proprius Note: Green squares indicate "marker" muscles that are most often abnormal for that root in an isolated radiculopathy. Blue squares indicate muscles that may be involved but are abnormal less frequently. This chart shows those muscles that are most helpful in making the electrodiagnosis of radiculopathy but does not indicate the entire myotomal representation of the individual muscle (see Table 32. C6 C7 C8 T1 patient has had previous neck or back surgery, the paraspinal muscles in the area of previous surgery may remain abnormal for years after the surgery, and any abnormal findings in these muscles would not help differentiate a new lesion from a remote effect of previous surgery. Thus, paraspinal muscles in the area of previous surgery are generally not sampled (see later). In all neuropathic lesions resulting in axonal loss, the time that elapses before a muscle begins to show fibrillation potentials. As the normal process of reinnervation then follows, it usually is quite slow and prolonged. He develops immediate pain in the back that radiates down the buttock and into the leg, along with numbness over the dorsum of the foot and weakness of hip abduction and ankle dorsiflexion. Decreased recruitment occurs because some of the L5 motor units have been blocked or lost. L2 Inferior gluteal nerve Gluteus maximus Superior gluteal nerve Gluteus medius Tensor fascia latae Obturator nerve Adductor longus Femoral nerve Iliopsoas Rectus femoris Vastus lateralis/medialis Sciatic nerve Medial hamstrings Lateral hamstrings Deep peroneal nerve Tibialis anterior Extensor hallucis longus Superficial peroneal nerve Peroneus longus Tibial nerve Medial gastrocnemius Soleus Flexor digitorum longus Tibialis posterior Abductor hallucis brevis Abductor digiti minimi pedis Note: Green squares indicate "marker" muscles that are most often abnormal for that root in an isolated radiculopathy. It is not until week 3 or 4 that fibrillation potentials develop in the lower leg L5-innervated muscles. Note that the biceps has bursts of activity that correlate to when the intercostal muscles are firing with breathing. This recording was from a patient who sustained a stab wound and microsurgical repair of the C5 and C6 nerve roots. Aberrant reinnervation can take one of two forms: (1) an axon that previously innervated a particular muscle grows down a different fascicle and innervates a different muscle than the original one, or (2) a single axon branches into two or more axons that go on to innervate two or more different muscles. The diaphragm is normally innervated by the phrenic nerve, which is derived principally from the C5 root with contributions from C3 and C4. During regeneration of C5 axons originally destined for the phrenic nerve, aberrant regrowth can occur into limb muscles that are normally partially supplied by the C5 root. In such a case, one can be certain that the lesion is not due to a single peripheral nerve injury because abnormalities are present in muscles innervated by the dorsal rami as well as by the musculocutaneous, axillary, and suprascapular nerves. However, in such a case, it is more challenging and sometimes impossible to differentiate between a C5 and C6 radiculopathy.
Cheap super avana 160 mg overnight delivery
Corrected cryptorchidism generally does not cause sexual dysfunction later in life erectile dysfunction journal articles cheap super avana online mastercard. Testes that have not descended by the time of adolescence will atrophy, causing sterility, but testosterone levels remain normal. A child with undescended testes has a 20% to 44% increase in risk for developing a malignant testicular tumor in adulthood. X Description the March of Dimes reports that birth defects of the ureter, bladder, and urethra are common, affecting as many as 1 in 10 infants. Some abnormalities cause few if any symptoms; others are painful and may cause urinary tract infections and kidney disease. Etiology the causes of congenital defects of the ureter, bladder, and urethra are unknown. Some of the problems are obvious at birth; others are not apparent until later, when they produce symptoms. The following is a brief discussion of the most common congenital urinary tract anomalies, together with their symptoms and possible treatments. The common symptoms may include frequent urinary infections, urinary frequency and urgency, diminished urine output, and flank pain. Retrocaval ureter occurs when the right ureter passes behind the inferior vena cava before entering the urinary bladder. The symptoms may include hydroureter (swelling of the ureter with urine), right flank pain, urinary tract infection, renal calculi, and hematuria (blood in the urine). Surgical resection and formation of a connection called anastomosis of the ureter constitute the treatment of choice. Ectopic orifice of the ureter occurs when the ureteral opening inserts into the vagina in females or into the prostate or vas deferens in males. The symptoms may include urinary obstruction, reflux of urine, incontinence, flank pain, and urinary urgency. Resection and ureteral reimplantation into the bladder are necessary for correction. Stricture or stenosis of the ureter means that one of the ureters is tightened or partially closed. The affected ureter may become enlarged, and hydronephrosis (swelling of the renal pelvis of the kidney with urine) may result. Nephrectomy may be required if severe renal damage has occurred as a result of hydronephrosis. Ureterocele is the bulging of the ureter into the urinary bladder, sometimes almost filling the bladder. Exstrophy of the bladder is a congenital malformation in which the lower portion of the abdominal wall and the anterior wall of the bladder are missing. Consequently, the inner surface of the posterior wall of the bladder is everted through the opening in the abdominal wall. The skin covering the hole in the abdominal wall is easily excoriated, or roughened by accumulating urine, and infection typically results. Reconstruction of the bladder and abdominal wall is required, and urinary diversion may be necessary. Congenital bladder diverticulum is caused by a diverticulum or pouching out of the bladder wall. Hypospadias is an abnormal opening of the male urethra onto the undersurface of the penis or of the female urethra into the vagina. Epispadias is an abnormal opening of the male urethra onto the upper surface of the penis or of the female urethra through a fissure in the labia minora and clitoris. Diagnostic Procedures Diagnostic tests include an x-ray of the urinary tract after the introduction of a contrast medium, or excretory urography; voiding cystoscopy; cystourethrography; urethroscopy; and ultrasonography. Congenital Diseases and Disorders 113 Prognosis With prompt treatment and surgical repair, most individuals live a normal life with little or no long-term complications. Treatment Treatment is aimed at correcting the deformity and maintaining the corrected position. Maintenance treatment includes special exercises, night splints, and orthopedic shoes. An individual also may have a combination of these basic forms: for example, talipes equinovarus, in which the toes point downward and the body of the foot bends inward. Etiology the exact cause is unknown, but a combination of genetic and environmental factors in utero has been implicated. Parents can be taught how to care for an infant with casts, splints, or orthopedic shoes. Hip dislocation may result if the fetus is not positioned correctly within the uterus before and during birth. Signs and Symptoms Physical examination shows asymmetric folds in the thigh of neonates with limited abduction of the affected hip. A shortening of the femur is noted when the knees and hips are flexed at right angles. The signs are typically quite obvious when children attempt to walk, if the condition has not been discovered before that time. Ortolani sign is the "clunk" felt when an examiner abducts (draws away from the body) and lifts the femurs of a supine infant. Before 3 months of age, treatment requires closed reduction of the dislocation, followed by the use of a splint-brace or cast for 2 to 3 months. Because the inheritance of one faulty X chromosome results in the absence of dystrophin, males rather than females have the disease. The exact mechanism by which the genetic defect produces muscle wasting is not known. Signs and Symptoms Manifestations of Duchenne muscular dystrophy begin between ages 3 and 5. The disease affects the leg and pelvic muscles before spreading to involuntary muscles. The affected child may have a characteristic waddling gait, may engage in toe-walking, and may have lordosis or other spinal deformities. The child may have difficulty running and climbing stairs and may tend to fall easily. Diagnostic Procedures A family history of the disease together with the clinical picture of characteristic symptoms suggests the diagnosis. A muscle biopsy showing characteristic connective tissue and fat deposits will confirm the diagnosis. Treatment No known treatment is successful in curing Duchenne muscular dystrophy, but procedures to correct or preserve mobility are helpful. Children with this condition are usually confined to a wheelchair by ages 9 to 12. Formerly it was believed that within 10 to 15 years of the onset of the disease, death commonly resulted from cardiac or respiratory complications or infections. Thanks to advances in both cardiac and respiratory care, men with the disease are living much longer lives-some even into their 40s and 50s-and are married and have families. Prevention Carriers of the genetic defect known to cause muscular dystrophy may receive genetic counseling regarding the risks of transmitting the disease. Families will need support and teaching on how to care for an infant or a child with a cast or splint, if necessary. If not treated promptly, abnormal development of the hip and permanent disability may result. It generally strikes during early childhood and can cause death within 10 to 15 years of onset. Because of the way the disease is inherited, far more males than females develop symptoms. Etiology the disease is the result of an X-linked recessive disorder, which is usually inherited but may also be due to mutation. The mucus clogs the pancreas, stopping the important enzymes that help the body break down and absorb food. Etiology the disease is caused by an underlying biochemical defect transmitted as an autosomal-recessive trait. If both parents are carriers of the recessive gene, the offspring have a 25% chance of having the disease. Respiratory symptoms may include wheezy respirations, a dry cough, dyspnea, tachypnea, and frequent lung infections, all stemming from accumulations of thick secretions in the smaller passages conveying air within the lung (bronchioles) and the air sacs (alveoli) of the lungs.
Order super avana from india
The infected child needs to maintain a high caloric intake and should avoid foods high in sugar; however erectile dysfunction frequency age discount super avana 160mg online, food may have to be offered slowly and in small amounts at first. Complementary Therapy Complementary therapy includes dietary limitations and appropriate nutritional therapy to replace fluid and electrolytes. Prognosis In the United States, the prognosis is good if detected early, if hydration is started immediately, and if antimicrobial treatment is begun. Some children, especially those under age 2, may die from such complications as dehydration, shock, and bacteremia. Prevention the importance of good hygiene cannot be overstressed, especially good hand washing when changing diapers or feeding children. Signs and Symptoms the child has a low-grade fever, coldlike symptoms, and a red facial rash that looks like a "slapped cheek. Between 20% and 60% of the children in outbreaks are symptomatic, and many are asymptomatically infected. The B19-specific antibodies can be detected with commercially available immunoassay kits. Treatment Generally, no treatment is needed; however, it is important to manage any fever. Although the exact route of transmission is essentially unknown, it is important to discard any used tissues appropriately and to encourage clients to drink ample fluids and practice good hand washing. Prevention Good hygiene and proper disposal of tissues with contaminated respiratory secretions are necessary. X Description Pertussis is an acute, highly infectious respiratory tract disease characterized by a repetitious, paroxysmal cough and a prolonged, harsh, or shrill sound during inspiration (the "whoop"). Pertussis affects infants and children more frequently and more severely than it does adults. It induces a mucopurulent secretion and hampers the natural ability of the respiratory tract to clear such secretions. The route of transmission for the disease is direct contact with any discharge from the mucous membrane of an infected person. Signs and Symptoms the signs and symptoms of pertussis can be divided into three stages. The catarrhal stage is marked by the gradual onset of coldlike symptoms-mild fever, running nose, dry cough, irritability, and anorexia. This stage lasts from 1 to 2 weeks, during which the disease is highly communicable. The paroxysmal stage is marked by the onset of the classic cough, consisting of a series of several short, severe coughs in rapid succession followed by a slow, strained inspiration, during which a "whoop" (stridor) may be heard. This stage, lasting 3 to 4 weeks, may be accompanied by weight loss, dehydration, vomiting, epistaxis, and hypoxia. After several weeks, a period of decline begins, marked by the gradual diminishment of coughing. Diagnostic Procedures A history of exposure to another infected individual and the presence of the classic cough may be sufficient to establish the diagnosis. A very high white blood cell count is another distinguishing feature of pertussis. Treatment Antibiotics administered during the catarrhal stage may check the development of the disease; if administration is delayed past this stage, antibiotics have little effect. The individual with pertussis requires meticulous care to ensure adequate nutrition, hydration, and clearance of mucous secretions. Fruits, vegetables, brown rice, clear vegetable soups, potatoes, and whole grain toast may be tried. Aromatherapy with basil, chamomile, eucalyptus, peppermint, and lavender in a cool mist vaporizer may be useful. Educate clients about the necessity of following the treatment plan, including taking all of the prescribed medication. Prognosis the prognosis for an individual with pertussis varies from case to case. Complications can occur as a result of seizures, apnea, encephalopathy, and pneumonia. Fifteen infants younger than 3 months died before they were old enough for the vaccination. Prevention A child can be rendered less susceptible to pertussis by receiving a series of immunizations with pertussis vaccine. Good hand washing and proper disposal of contaminated tissue from respiratory secretions are essential. It is characterized by a gray to black membrane-like coating that forms over mucous membrane surfaces, particularly along the respiratory tract, which can block airways. It can cause a toxic reaction that primarily affects the heart and peripheral nerves. Most cases 76 Diseases of the Human Body occur in children under age 10, but older children and adults also may be affected. Transmission is through contact with discharge from the nose, throat, eye, and skin lesions. There may be a strong, foul odor to the breath; bluish skin color; bloody, watery nasal drainage; and breathing problems. Diagnostic Procedures the appearance of the characteristic membrane may be sufficient to establish a diagnosis of diphtheria. A definitive diagnosis can be made only by identifying the bacterium in nose and throat cultures. Treatment the only specific treatment is administration of sufficient quantities of diphtheria antitoxin as early in the course of the disease as possible followed by antibiotic therapy. Emergency measures may be required to maintain an airway or to control cardiac complications. Booster doses should be administered at appropriate intervals during early childhood. While today the incidence of diphtheria has greatly decreased, with only five cases reported in the United States in the last 10 years, it is a disease that must be recognized for its serious potential. Also, acknowledging the diseases prevented by the vaccination makes the public more aware of the consequences of refusing vaccinations. The disease may affect any person at any time-the elderly, migrant workers, children, and injection drug users. Puncture wounds are particularly prone to tetanus, but sores can become infected by the bacteria. Etiology the disease is caused by Clostridium tetani, a bacterium commonly found in soil. The bacillus becomes pathogenic when its spores enter the body through a puncture wound. Burns, surgical incisions, and chronic skin ulcers may also provide opportunities for C. The spores produce a powerful toxin that attacks the central nervous system and that also acts directly on voluntary muscles to produce contraction. Stiffness of the jaw, esophageal muscles, and some neck muscles is often the first sign of the disease. Finally, the muscles of the back and the extremities may become rigid, or the individual may experience extremely severe convulsive muscle spasms. Hospitalization of the infected child is often necessary for proper treatment and observation for complications. Prognosis the prognosis for an individual with diphtheria varies according to the severity of the disease. Complications include myocarditis (the most common complication), thrombocytopenia, and vocal cord paralysis. Infectious and Communicable Diseases 77 phase of the disease often is accompanied by high fever, profuse sweating, tachycardia, dysphagia, and intense pain. Diagnostic Procedures Tetanus is diagnosed on the basis of its classic symptomatology.
Order generic super avana on-line
Note in the trace erectile dysfunction vs impotence super avana 160 mg fast delivery, the sweep speed of 10 ms allows one to appreciate the sinusoidal waveform. However, if the sweep speed is set at 1 or 2 ms and the sensitivity increased to 10 V, as is done for sensory nerve conduction studies, the 60-Hz waveform can saturate the amplifier. If the impedances of the active and reference electrodes are similar, the same electrical noise is seen at the G1 and G2 inputs and subsequently is removed by differential amplification (common mode rejection). Electrode impedance mismatch can be reduced by proper skin cleaning and use of conducting electrode jelly. With differential amplification, the difference between the signals at the active (G1) and reference (G2) electrodes is amplified and then displayed. Thus, if the same electrical noise is present at both the active and reference electrodes, it will be subtracted out, and only the signal of interest will be amplified (this is known as common mode rejection). However, if the electrical noise is larger at one of the electrodes than the other, the noise will not be subtracted out. This waveform makes little sense until one changes the sensitivity to a much lower level. The best way to achieve identical electrical noise at each electrode is to ensure that the impedance at each electrode is the same. In this example, the resistance at one electrode is higher because of insufficient electrode gel. Because the electrical noise is not the same at the two electrodes, it will not be subtracted out when amplified. Sometimes, the resulting artifact is so large that it saturates the amplifier, resulting in a repeating waveform consisting of large vertical lines (top). This waveform is not recognizable until one changes the sensitivity to a much lower level (from 20 V/div [top] to 10 mV/div [bottom]), which discloses the source of the waveform: a 60-Hz sinusoidal alternating current waveform. All signals recorded in nerve conduction studies and electromyography result from differential amplification. Top, the signal present at the reference electrode (G2) is subtracted from the signal seen at the active electrode (G1) and amplified. Each recording electrode has its own impedance or resistance, modeled as R1 and R2, for the active and reference electrodes, respectively. Middle, If R1 and R2 are identical, any 60-Hz interference will induce a similar electrical noise at both inputs. The noise will then be subtracted out, and only the signal of interest will be amplified. Bottom, If electrode impedances are mismatched (R1 < R2), the amount of electrical noise will be different at the two inputs. Some of the electrical noise will then be amplified, often obliterating or obscuring the signal of interest. The voltage (E), in this case the voltage from electrical noise, equals the current (I) induced from the electrical noise multiplied by the resistance (R), or impedance. If the resistance, or impedance, is different at the two electrodes, the same electrical noise will induce a different voltage at each electrode input. This difference will then be amplified and displayed, often obscuring the signal of interest. The best way to eliminate 60-Hz interference is to ensure that each electrode appears identical to the amplifier (Box 8. Next, the skin preparation should be thorough, using either alcohol or acetone to remove dirt and oil. Conducting electrode jelly is then applied to the electrode before it is attached to the skin. The recording electrodes should be held firmly against the skin with tape or a Velcro band. Finally, the closer the electrodes are to each other, the more likely any associated electrical noise will appear identical to a differential amplifier. The role of the filters is to faithfully reproduce the signal of interest while trying to exclude both low- and high-frequency electrical noise. Low-frequency (high-pass) filters exclude signals below a set frequency while allowing higher-frequency signals to pass through. High-frequency (low-pass) filters exclude signals above a certain frequency while allowing lower-frequency signals to pass through. For motor conduction studies, the low- and high-frequency filters typically are set at 10 and 10 kHz, respectively. For sensory conduction studies, the low- and high-frequency filters typically are set at 20 and 2 kHz, respectively. Note that the high-frequency filter is set lower for sensory than for motor nerve conduction studies. No filter, whether analog or digital, results in a sharp cutoff with complete exclusion of all signals above the high-frequency settings or below the low-frequency settings. It is essential to recognize that filtering also results in some loss or alteration of the signal of interest. For instance, as the lowfrequency filter is reduced, more low-frequency signals pass through. This results in the duration of the recorded potential increasing slightly because the duration is primarily a lower frequency response. Likewise, as the high-frequency filter is lowered, more high-frequency signals are excluded. It is often assumed that the electrodes and their connections are in working order. However, with prolonged use, wires and connections may fray and break, especially at points where cables end. To add to the confusion, frayed wires can lead to intermittent artifacts depending on the position of the wire and whether the connection is temporarily intact, partially broken, or completely separated. All waveforms recorded in electrodiagnostics are composed of a spectrum of frequencies. By allowing the signal to pass through a certain "passband," some unwanted electrical noise can be attenuated. In this example for motor conduction studies, the low- and high-frequency filters typically are set at 10 and 10 kHz, respectively. This improves the quality of the recorded waveform by excluding low- and high-frequency noise. However, there is a tradeoff as some of the actual response is attenuated as well. Accordingly, all potentials should be obtained with standardized filter settings and should be compared only with normal values based on studies using the same filter settings. Ulnar sensory study, stimulating elbow, recording digit 5, with varying high-frequency filters. Note that as the higher frequencies are filtered out (bottom trace), the amplitude of the sensory potential markedly decreases. Most often this occurs when recording small potentials in the microvolt range, typically during sensory and mixed nerve studies. In this situation, the electrical noise can be reduced or eliminated by using electronic averaging. With electronic averaging, serial stimulations are digitized and then mathematically averaged. Because electrical noise is random, the positive and negative phases of electrical noise will cancel each other out as a greater number of stimulations are averaged, thereby leaving the potential of interest. Stimulus Artifact During routine nerve conduction studies, the current from the stimulator depolarizes the underlying nerve, but it also spreads via volume conduction through the tissues within the limb and is seen at the recording electrodes. This stimulus artifact occurs in every nerve conduction study and serves a useful purpose by indicating when the shock occurred and from which point latencies should be measured. The stimulus artifact becomes problematic, however, if its trailing edge overlaps with the potential being recorded. With the averaged trace, the noise is much improved, and the signal of the sensory response is more clearly seen, allowing the onset latency and amplitude to be more accurately measured.
