
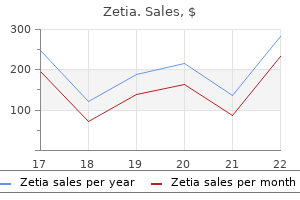
Buy genuine zetia online
Radiation therapy has been used concurrently with chemotherapy in an attempt to limit acute hemorrhagic complications from these metastases cholesterol eggs or bacon discount zetia 10 mg visa. Brain irradiation combined with systemic chemotherapy is successful in controlling brain metastases, with cure rates up to 75% in patients who initially present with brain metastases. However, a similar primary remission rate has also been reported among patients treated with combination regimens that incorporated high-dose systemic methotrexate combined with intrathecal methotrexate infusions without brain irradiation. The best treatment for liver or other high-risk sites of metastases has not been established. Even with intense chemotherapy, additional surgery may be necessary to control hemorrhage from metastases, remove chemoresistant disease, or treat other complications to stabilize high-risk patients during therapy. Myelosuppression is more severe in patients receiving regimens for salvage than when they are used as primary therapy. Ifosfamide-containing chemotherapy produced responses in four of five patients reported by Sutton and colleagues, but only one patient 7. Surgery Brewer and associates reported that survival of patients treated with hysterectomy was only 40% for women with nonmetastatic choriocarcinoma and only 19% for those with metastatic choriocarcinoma before effective chemotherapy was developed. The majority of their patients died of progressive disease within 2 years of surgery. However, many procedures remain useful adjuncts when integrated into the management of these patients. Primary or delayed hysterectomy can be integrated into management to remove central disease, and surgical extirpation of metastases may cure highly selected patients with drug-resistant disease. At Duke University Medical Center, extirpative procedures such as hysterectomy were usually performed during a course of chemotherapy to minimize the possibility of inducing metastases by surgical manipulation of tissues. There did not appear to be an increase in surgical morbidity using this combined modality approach. Surgical procedures are often required during therapy of patients with high-risk disease to treat complications of the disease, such as hemorrhage or abscess, and allow stabilization during chemotherapy. Percutaneous angiographic embolization can allow relatively noninvasive control of hemorrhagic complications of pelvic tumors or metastatic lesions. Furthermore, the majority can be cured with chemotherapy alone, especially women with nonmetastatic or low-risk metastatic disease. Of these, 162 wished to retain childbearing capacity and 89% were able to avoid hysterectomy. All 32 women treated with primary hysterectomy combined with methotrexate or actinomycin-D single-agent chemotherapy regimens entered sustained remission. When compared to similar patients who had low-risk disease and were treated with chemotherapy alone, patients receiving primary hysterectomy had shorter duration of chemotherapy and lower total dosage of chemotherapy, roughly equivalent to one cycle of chemotherapy. They found that the total dosage of etoposide was decreased in women with nonmetastatic disease treated with adjuvant hysterectomy compared to those who were treated with chemotherapy alone, again roughly equivalent to a single cycle of chemotherapy. This effect was not observed among their patients with low-risk metastatic disease, where similar total dosages of etoposide were given to patients treated with adjuvant hysterectomy or chemotherapy alone. Therefore, the major role of primary hysterectomy should be as part of primary treatment for women with nonmetastatic disease or with limited 212 7. Delayed hysterectomy is often considered for patients who fail to respond to primary chemotherapy. Others have reported that salvage hysterectomy is effective in producing remissions in most patients with nonmetastatic or low-risk metastatic disease. Control of extrauterine disease is central in the success of salvage hysterectomy for these patients. The majority of these patients had no radiographic evidence of extrauterine disease, and 10 (83%) had sustained remissions. All patients had lesions localized in the myometrium and defined by pelvic angiography, ultrasound, and computerized tomography techniques. Pregnancies have been documented after conservative resections of invasive moles; Kanazawa and colleagues observed that reproductive performance was similar to that of patients treated with chemotherapy alone. Because of the high cure rates reported following chemotherapy alone in similar patients, it is more rational to consider these as salvage procedures in women with localized chemoresistant disease. Although this can safely be performed in conjunction with chemotherapy, it is not necessary to resect lung metastases in the majority of patients. As in the case of brain, liver, or renal metastases, any woman of reproductive age who presents with an apparent metastatic malignancy of unknown primary site should be 7. Resection of pulmonary nodules in highly selected patients with drug-resistant disease may successfully induce remission. Immediately before performing pulmonary resection, it is important to exclude the possibility of active disease elsewhere by performing a comprehensive metastatic survey. Highly selected patients will require more than one pulmonary resection during the course of treatment in order to achieve a durable remission. However, Rustin and colleagues recommended an approach using early craniotomy with excision of isolated lesions combined with high-dose systemic and intrathecal chemotherapy to treat patients with brain metastases. Both primary radiation therapy combined with chemotherapy and the approach emphasizing early surgical intervention appear to have similar efficacy in previously untreated patients. She is in remission following surgical resection of this brain lesion during her first cycle of chemotherapy followed by multiple cycles of chemotherapy with high-dose methotrexate combinations, platin-taxane, and hysterectomy. In these patients, it is important to exclude active disease elsewhere before attempting surgical resection. Sometimes craniotomy is required for women who require acute decompression of central nervous system hemorrhagic lesions to allow stabilization and institution of therapy. In general, resection of distant metastases is unlikely to be successful if there is evidence of disseminated disease resistant to chemotherapy. These should not be biopsied or resected unless they represent the only site of drug-resistant disease. They are usually associated with other high-risk factors and disseminated disease. Survivors had limited metastatic involvement elsewhere when compared to patients with renal metastases who died. Liver metastases, although prone to catastrophic intra-abdominal hemorrhage, are less likely to be successfully controlled with surgical resection. Selective angiographic embolization techniques should be considered as an option if possible. Only rarely will resection of isolated liver metastases be feasible for treatment of drug-resistant disease because most patients will have other sites of active disease or diffuse involvement of the liver. These patients often require prolonged courses of chemotherapy, transfusion of blood products, nutritional support, and antibiotics during the course of their treatment. Vaginal metastases are the site of active disease most often treated with selective angiographic embolization, when simple packing or suturing techniques have failed to control hemorrhage. Two of the patients with liver metastases achieved long-term remissions, with minimal hematologic toxicity recorded during treatment. Lim and colleagues reported 14 patients treated over a 20-year interval with selective angiographic embolization for this indication. Hemorrhage was initially controlled with the first procedure in 11 (78%) and 6 (45%) patients required a second embolization for treatment of recurrent bleeding, while only 2 (15%) patients required hysterectomy. Radiation is used most frequently to treat patients with brain or liver metastases in an effort to minimize hemorrhagic complications from disease at these sites. Whole brain irradiation has been used in the majority of series of patients with brain metastases reported from the United States. Most series report administration of between 2000 and 4000 cGy in 10 to 20 equal fractions that are given concurrently with combination chemotherapy, with reduced field boosts given in selected patients. Schecter and colleagues reported that the 5-year actuarial local control for patients given doses less than 2200 cGy was only 24%, significantly worse than 91% local control among patients given 2200 to 6000 cGy. Survival rates of 50% to 75% are reported in series of patients who initially presented with brain metastases and received combined chemoradiation. Survival of these patients is influenced in part by the extent and subsequent control of extracranial disease, in addition to the extent of central nervous system involvement. Small and colleagues reported that women who were asymptomatic at presentation had a 100% survival rate compared to only 38% survival rate in those who presented with symptoms from brain metastases, a significant difference. Evans and associates reported that patients with new brain metastases diagnosed at the time of recurrence or who developed brain metastases during chemotherapy had survival rates of only 38% and 0%, respectively. These groups had significantly worse survival than the 75% survival rates of their patients, who presented with brain metastases for primary therapy.
Order zetia now
Pregnancy-derived hormonal influences on the development and clinical behavior of breast cancer In total cholesterol lowering foods nuts purchase cheap zetia online, 50,302 women with invasive breast cancer were compared with 96,973 control subjects. The investigators noted that women with breast cancer had fewer births than did control subjects (2. Thus the longer women breast fed, the more they were protected against breast cancer. The lack of or short lifetime duration of breast feeding typical of women in developed countries may contribute greatly to the high incidence of breast cancer in industrialized nations. Hormonal Considerations: Pregnancy Coincident with Breast Cancer Although there is no clear evidence that pregnancy adversely affects the course of this disease, the suspicion persists. It has been established that once the diagnosis is made, stage for stage, the pregnant patient does as well as the nonpregnant patient. However, the low incidence of stage I lesions in pregnancy strongly suggests an acceleration of the disease process in the preclinical period. Many cell kinetic studies of breast cancer suggest that lesions are harbored within the breast for 5 to 8 years before becoming clinical entities. Because the period of gestation is no longer than 9 months, it is difficult to believe that the sole explanation for the high incidence of advanced disease in pregnancy is related to late diagnosis caused by the engorged breast. The massive endogenous hormone production in pregnancy may adversely affect the course of breast cancer. Urinary excretion of all three major fractions, estrone, estradiol, and estriol, rises progressively after the eighth week of gestation, although there is a disproportionate rise in estriol production by the placenta. Whether the stimulatory effect of increased estrogen production has an adverse effect on prognosis or whether the disproportionate rise of estriol, a relatively weak estrogen and a possible antagonist of estrone and estradiol, confers some measure of protection is unknown. Additional hormone substances secreted in increased quantities in pregnancy that might influence neoplastic growths in the breast include the glucocorticoids and prolactin. Elevated corticosteroid levels are a regular accompaniment of pregnancy and might influence the outcome of breast cancer. Mean production of 17-hydroxycorticosteroids increases from 12 mg/24 hours to approximately 18 mg/24 hours in late pregnancy. Because glucocorticoids can reduce cellular immunity and perhaps promote the implantation and growth of malignant neoplasms, this increased production has grave clinical implications. Prolactin promotes the growth of dimethyleneanthracene-induced mammary tumors in mice. Its role is not established in humans, but it is a subject of current investigation. The levels of prolactin in patients with breast cancer are not appreciably different from those in control subjects, and prolactin suppression with ergot compounds or with l-dopa has not proved to be of therapeutic value. However, the observation that women with bone pain from metastatic breast cancer sometimes obtain relief from prolactin suppression implicates prolactin as a possible promoter of breast cancer in humans. Pregnancy Termination Historically, pregnancy was of concern to surgeons primarily because the risk of excess hemorrhage and shock with mastectomy was increased greatly in the gravid state. Billroth advocated premature induction of labor for this reason but did not find that abortion contributed to cure. More contemporary commentators have argued that the striking rise in estrogen production during pregnancy is of sufficient concern to warrant pregnancy termination and that future pregnancy avoidance should be an important principle of continuing care. Indeed, although many clinicians think that localized breast cancer in the first trimester is a valid reason to 438 15. Similarly, therapy for localized disease in later pregnancy can be carried out when the diagnosis is made without pregnancy termination. Therapeutic abortion is not currently believed to be an essential component of effective treatment of early disease, despite the theoretic advantage of removing the source of massive estrogen production. It is critically important to emphasize that treatment of breast cancer should not be delayed provided there are no major obstetric issues. In advanced breast cancer, therapeutic abortion is usually a necessity to achieve effective palliation. In the first trimester of pregnancy, the termination can be accomplished by suction curettage of the uterus; later in pregnancy, termination is accomplished by dinoprostone (Prostin) suppositories, oxytocin (Pitocin) administration, hysterotomy, or hysterectomy. A short wait until a viable fetus can be obtained might not be accompanied by significant progress of the neoplasm. Continued gestation represents no threat to the fetus, and the risk of transplacental metastases to the fetus is negligible. Tamoxifen Tamoxifen citrate is a nonsteroidal weak estrogen that has found successful applications for each stage of breast cancer in the treatment of selected patients. The long-term effects of tamoxifen use and whether it may increase gynecologic cancers in daughters are unknown. In pregnant rats, tamoxifen administration has been associated with breast cancer in the female offspring. Cunha and colleagues examined 54 genital tracts isolated from 4- to 19-week-old human female fetuses and grown for 1 to 2 months in untreated athymic nude mice or host mice treated by subcutaneous pellet with the antiestrogen clomiphene, tamoxifen, or the synthetic estrogen diethylstilbestrol. The investigators noted that condensation and segregation of the uterine mesenchyme was greatly impaired and that the fallopian tube epithelium was hyperplastic and disorganized with distortion of the complex mucosal plications in drug-treated specimens as compared with untreated age-matched control subjects. In 1997 Tewari and colleagues described the first patient to have given birth to a child with congenital anomalies following systemic tamoxifen therapy through 20 weeks of gestation. Another fetus exposed to tamoxifen during all the first, second, and early part of the third trimesters was born at 26 weeks with oculoauriculovertebral dysplasia. A third case appeared in 2001 and involved a fetus delivered at 31 weeks of gestation whose mother was given tamoxifen as sole systemic therapy and locoregional irradiation before pregnancy was determined. In addition to moderate hyaline membrane disease and necrotizing enterocolitis that was attributable to prematurity, the child had preauricular skin tags, but an appropriate birth weight and no major malformations. Hormonal Considerations: Pregnancy Following Breast Cancer It has been estimated that only 7% of fertile women go on to conceive following the diagnosis and treatment of breast cancer. Nevertheless, a patient with breast cancer may have several concerns regarding future fertility, not least of which is whether she will remain fertile following treatment. In addition, the risk of recurrence conferred by subsequent pregnancy needs to be addressed because several authors have postulated that the immunosuppressant and hormonal effects of pregnancy so close to diagnosis may have a significant deleterious effect. The recommendations given to such patients should be influenced by two major considerations: 1. For those who continue to ovulate and who are desirous of future childbearing, it has been common practice to recommend a waiting period of 2 years following the diagnosis of breast cancer before attempting to conceive because most recurrences occur within the first 2 years of diagnosis. Of note, women who have a subsequent pregnancy have equivalent or possibly better survival when matched for stage. Gelber and colleagues evaluated 94 patients from the International Breast Cancer Study Group who became pregnant after the diagnosis of early-stage breast cancer and compared them to 188 control subjects. The overall 5- and 10-year survival rates from the diagnosis of early-stage breast cancer among the study group was 92% and 86%, respectively, whereas that of the comparison group was 85% and 74%, respectively. Some have speculated an antitumor effect of the pregnancy, but of course this could reflect the "healthy mother" bias, in that only those select women who feel healthy will go on to conceive. Although it may be presumptuous to conclude on the basis of retrospective studies that pregnancy protects against recurrence after mastectomy, it is reasonably safe to conclude that it does not promote it. The converse, that pregnancy with recurrence should be terminated in most instances and that an uneventful pregnancy in no way guarantees against a subsequent recurrence, is also true. Indeed, there are cases on record in which multiple pregnancies have eventually been followed by recurrence. Prophylactic Oophorectomy Surgical castration for patients with early-stage breast cancer has been advocated to prevent further pregnancy, which might cause recrudescence of the disease through hormone stimulation. Oophorectomy also serves to eliminate the ovarian source of estrogen production, ideally preventing or delaying subsequent recurrence. Neither argument is substantiated by data to support a role for "prophylactic castration. As discussed earlier, pregnancy after treatment for breast cancer has no influence on the disease, and a few reports even suggest that future pregnancies might be protective. The rationale for eliminating the ovarian source of estrogens in the primary treatment of early disease is based on an observation that castration in the presence of observable recurrent disease results in partial or complete temporary tumor regression in approximately one third of cases. This argument has been refuted by two large clinical trials conducted in the United States that failed to demonstrate a significant benefit from castration and adjuvant therapy. After an observation period of 10 years, there was no evidence that those who were castrated derived any benefit from the procedure.
Discount 10mg zetia otc
Zanetta and colleagues evaluated 138 women with germ cell malignancies of all stages treated with fertility-sparing surgery cholesterol definition for biology cheap generic zetia uk, 81 of who received postoperative chemotherapy. Survival was comparable between patients treated with radical surgery and fertility-sparing surgery after a mean follow-up period of 67 months. Low and colleagues retrospectively reviewed 74 patients with germ cell malignancies of all cell types treated with 12. After 52 months of follow-up, patients with advanced disease had a 94% survival, comparable to historical survival rates. The value of secondary cytoreduction procedures in patients with germ cell malignancies has not been studied. Given the sensitivity of these malignancies to combination chemotherapy regimens, it is highly likely that metastatic lesions will respond to subsequent chemotherapy, making the value of secondary cytoreduction questionable. Limited cytoreduction remains an effective management option for isolated lesions. In summary, patients with germ cell malignancies should undergo operative evaluation, staging, and cytoreduction. If future fertility is not desired, surgical treatment should be identical to that for epithelial ovarian cancers. If preservation of fertility is desired, conservative management should be used with conservation of the uterus and contralateral ovary and cytoreduction to optimal residual disease should be performed if possible. In spite of the success of surgical management, surgeons should recognize the excellent response of these tumors to chemotherapy when aggressive and potentially morbid resections of metastatic and retroperitoneal disease are considered. Surveillance for Stage I Tumors As previously noted, historically in the gynecologic oncology literature only patients with stage Ia dysgerminoma or stage Ia grade I immature teratoma of the ovary have been treated conservatively without adjuvant chemotherapy. Similarly, male patients with stage I germ cell tumors are followed with observation only as standard practice. Rustin and Patterson published provocative data on their 37-year experience with a liberal surveillance policy for patients with stage I germ cell tumors of the ovary. In their first report, 24 patients with stage Ia germ cell tumor (9 dysgerminoma, 9 pure immature teratoma, and 6 endodermal sinus tumor with or without immature teratoma) were followed without chemotherapy after surgery. Eight patients had a recurrence or developed a second primary germ cell tumor and required chemotherapy. In their second publication, 37 patients with stage Ia germ cell malignancies were followed with surveillance only after surgery. Twenty-two percent of dysgerminoma and 36% of nondysgerminoma patients had a recurrence. All but one of these patients were successfully salvaged and cured with cisplatin-based chemotherapy at the time of recurrence. It is unlikely that randomized trials addressing the safety of this approach in ovarian germ cell tumors will be performed. Of 48 patients who did not have teratomatous lesions in their primary surgery, 45 had no tumor. The 3 patients who had persistent tumors died of their disease despite aggressive therapy. Fourteen of the 16 with residual teratoma and 6 of the 7 with bulky disease remained tumor free after secondary cytoreduction. Radiation Therapy In the past, radiation therapy was traditionally used as adjuvant therapy for patients with germ cell malignancies and dysgerminomas in particular. However, with the recent advances and success rates seen with combination chemotherapy, radiation therapy is rarely used today. Chemotherapy Tremendous advances have been made in the chemotherapeutic management of germ cell malignancies, such that current management strategies offer even advanced malignancies an excellent chance at long-term control or cure. This transition resulted in an improvement in overall survival; however, failures still occurred even in patients with good prognosis at the conclusion of primary surgery. Although successful, concern exists over potential long-term pulmonary toxicity of bleomycin and the risk of secondary malignancies associated with etoposide. Traditionally, cisplatin and etoposide are administered over 5 days, whereas bleomycin is administered weekly. Several adult trials in testicular germ cell malignancies have suggested an improvement in efficacy compared to standard-dose cisplatin, whereas other studies have not seen this association. These studies have not been replicated in adults with ovarian germ cell malignancies. Currently, there is no established role of high-dose therapy in ovarian germ cell tumors. Current management strategies for germ cell malignancies utilize chemotherapy in an adjuvant setting and to treat recurrent disease. Completely resected disease treated in this fashion can be cured nearly 100% of the time. Metastatic or incompletely resected tumors, however, may fare worse but still have excellent long-term survival rates and should be treated aggressively with adjuvant chemotherapy. Recurrences in Germ Cell Cancer Even in cases of advanced-stage disease, the majority of patients with germ cell malignancies are cured with a combination of primary surgery and adjuvant combination platinum-based chemotherapy. All patients with germ cell malignancies, especially early-stage disease treated with conservative therapy for curative intent, warrant close follow-up. Patients with early-stage dysgerminoma treated with salpingooophorectomy alone can be expected to experience recurrence in 15% to 25% of cases. For all germ cell malignancies, recurrences in many cases can be treated successfully. Recurrences after chemotherapy are defined as platinum resistant or platinum sensitive, a classification with clinical significance because platinum-resistant disease is not thought to be curable. Using different chemotherapeutic regimens, 12 of 42 (29%) patients are currently disease free. In this study, 24 patients had surgery and 12 are alive, all with less than 2 cm of residual disease. More recently, male patients with platinumresistant or platinum-refractory disease germ cell tumors have been treated with combination chemotherapy consisting of gemcitabine, oxaliplatin, and paclitaxel. This regimen has an acceptable toxicity profile, a 51% overall response rate, and a 39% complete or tumor marker negative response rate. For patients with platinum-resistant or platinum-refractory disease, optimal treatment has not been defined and prognosis overall is poor. Treatment Toxicity Given the favorable long-term outcomes associated with modern surgical management and combination platinum-based chemotherapy for women with germ cell malignancies, the long-term effects of treatment toxicity cannot be ignored. Because many of these patients desire future fertility and undergo conservative surgery for their disease, meticulous surgical technique is essential to avoid future infertility related to surgically induced pelvic adhesive disease. A thorough understanding of the natural history and management options of these tumors is essential. Women with fertility-sparing surgery can be expected to have the same survival outcome as those patients treated with standard surgery. This study revealed that the use of fertility-sparing surgery also had increased over the study period. The most common histologic subtype was immature teratoma (55%) followed by dysgerminoma (32%). The long-term effect of combination chemotherapy in germ cell malignancies is less clear. The most significant risk factor for impaired fertility is age and type of treatment administered. Although ovarian failure is a risk associated with chemotherapy, factors such as older age at treatment, higher drug doses, and long duration of therapy appear to confer higher risk. Although normal menstrual cycles will likely resume in reproductive-age women, data suggest that diminished ovarian reserve resulting in a significant reduction in the probability of pregnancy by 50% is present in these patients as determined by reduced ovarian volume compared to controls, fewer antral follicles on ultrasonography, and lower levels of inhibin B and estradiol on cycle days 2 to 5. Alkylating agents such as cyclophosphamide are far more likely to cause toxicity to the gonads than other chemotherapeutic agents. Ninety percent of study patients resumed menses and 70% resumed spontaneous ovulation within 8 months of completing therapy, compared to 33% and 26% of control patients, respectively. In the setting of germ cell malignancies, in which younger age at diagnosis is the norm, these patients tolerate therapy quite well. The stroma is almost always infiltrated with lymphocytes and often contains granulomas similar to those of sarcoid. Occasionally, dysgerminoma contains isolated gonadotropin-producing syncytiotrophoblastic giant cells. In such cases, the dysgerminoma often develops in a previously existing gonadoblastoma. The symptoms of dysgerminoma are not distinctive, and they are similar to those observed in patients with other solid ovarian neoplasms.
Order zetia 10mg with visa
Clearly cachexia is related to nutritional status because the cancer itself causes metabolic alterations such as increased muscle protein breakdown and glucose metabolism and the treatment of cancer affects appetite and food intake cholesterol mayo clinic buy zetia in united states online. Furthermore, it is evident that malnutrition contributes to poor outcome in gynecologic oncology patients. However, of note, Megace is thought to be more effective than either eicosapentaenoic acid (alpha 3-omega fatty acid) or marijuana derivatives, and only corticosteroids may perform as effectively as Megace. Unfortunately, Megace carries the risk of venous thromboembolism, perhaps as high as a sixfold increase, and this might limit its use in the gynecologic oncology patient population. It is well recognized that physical and psychological symptoms are intertwined and patients can benefit from a multidisciplinary approach to care. Strategies for Breaking Bad News and Preserving Hope Perhaps the most important tool in caring for patients and their families is effective communication. Transferring information about the diagnosis, prognosis, risks, and benefits of treatment and progression of disease is a difficult and unavoidable responsibility. Sharing bad news and responding to the questions presented by the patient and family require compassion, empathy, and skill. The absence of an integrated formal palliative care curriculum throughout medical training continues to promote a skill set gap. Significantly, patients do vary in the degree of information that they are able to assimilate at one time. Traditionally, men with advanced disease, older patients, and individuals from lower socioeconomic backgrounds are likely to want to hear fewer details and may comfortably defer to the physician and/or family with regard to decision-making. In most cases, patients want to hear the diagnosis from the physician who will be responsible for their care. Despite the most sensitive and effective communication style, patients are left with major concerns about their situation as it relates to their physical, social, psychological, and spiritual well-being. Excessive concern about the need to preserve hope can lead to false optimism or less than full disclosure over time. Lending strength does not require that the physician be less than honest but that the truth be disclosed over a period of time, in a setting in which the patient has the support required, and with repetition so that information can be assimilated and understood in small amounts. Patients should be encouraged and nurtured to develop their own coping strategies and defense mechanisms in dealing with their illness. Conveying a balance of honesty and maintaining hope can sometimes seem impossible, often because physicians tend to project their own concerns onto patients and assume that they will give up hope. In reality, hope is an innate characteristic that is rarely abandoned by open and compassionate discussion of the prognosis and treatment options. When there are no remaining viable cytotoxic treatment options, there are still many palliative options that can achieve meaningful therapeutic ends, thus preserving hope and avoiding a sense of helplessness. It is useful for patients to hear such optimism in the face of a generally poor prognosis. Unfortunately, doctors and other staff tend to spend less time with patients as the disease progresses and patients deteriorate into a terminal condition. This is presumably because the health care professionals feel helpless (and perhaps even threatened) when confronted with the imminence of death. Many health care professionals fail to realize the importance of compassion and active palliative care. Although most patients know when they are dying and can verbalize this realization, they also retain hope. One study that focused on end-of-life preferences of gynecologic cancer patients reported that only 622 20. Most (70%) of these patients expressed their resolve to continue fighting against their disease, even under the poorest prognostic circumstances. Proper management involves directing resources to assist with this fight and fostering this hope among dying patients. The involvement of other professionals familiar with care for the dying can relieve the physician of being the sole provider of hope with sensitive attention to incurable problems. A cancer diagnosis creates a profound sense of loss of control and fear for many individuals. Changes in physical function and the effect on psychosocial issues may further compound this sense. Stressors commonly experienced by patients undergoing cancer treatment may be as problematic for the patient as the physical decline. Patients are often reluctant to disclose struggles, including feelings of depression, and anxiety if they do not perceive this disclosure to be relevant to their physical care. Recent research has shown that many individuals are fearful of burdening their family members emotionally, physically, and financially during their final days. This information heightens our awareness to formally evaluate depression in terminally ill cancer patients and provide timely intervention as indicated. Discussions about resources available to assist patients and families, including the role and function of community agencies, support groups, and hospice programs, are critical. As noted earlier, pharmacologic interventions are often necessary but should be considered in combination with psychological counseling, supportive interventions, and education for the patient and family. Determination of the appropriate referral depends in large part on the type and magnitude of the psychosocial or psychological disruption and the extent to which this diagnosis interfaces with physical symptomatology such as pain or fatigue. Optimal programs include a team consisting of psychiatry, psychology, social work, and chaplain services. Bereavement follow-up is typically a part of hospice services, and institutions may successfully partner with local hospices to make this service accessible for these families. Dyspnea may result from a combination of three different complications: first, obstructive pathology such as pleural effusions; second, cancer cachexia or malnutrition and weakness; and, third, an increase in ventilator requirements such as metabolic acidosis or anemia. For symptomatic control and/or when mechanical control of the pleural effusion is not an option, most advocate opioids and/or oxygen therapy. Benzodiazepines and oxygen therapy may also have a role in control of dyspnea, although evidence is lacking. Finally, some have advocated activity modifications to prevent the onset of dyspnea, which may involve caregiver instruction to tailor activities of daily living. Psychosocial care must continue to address the needs of the family as death imminently approaches and after death occurs. Table 20-19 illustrates the range of bereavement services that may be available for family members. Although epithelial ovarian cancer is a surface-spreading disease that rarely invades vital organs, partial or complete bowel obstruction is often seen at the time of initial diagnosis or, more frequently, in association with recurrent disease. Obstruction may be secondary to extrinsic compression of the small bowel or hypoperistalsis as a result of mesenteric and bowel surface implants. The symptoms, which are almost always present, are intestinal colic, continuous abdominal pain, nausea, and vomiting. In most cases, nausea and vomiting can be relieved by conservative measures, and intestinal symptoms usually resolve after primary cytoreductive surgery and multiagent cisplatin-based cytotoxic chemotherapy. Despite the high objective response rate of primary epithelial ovarian cancer to several platinum-based combination chemotherapeutic regimens, most patients with advanced disease often develop intraperitoneal recurrences and require a salvage regimen for palliation of symptoms. Several therapeutic strategies have been used in these patients, such as including re-treatment with cisplatin or carboplatin or the use of paclitaxel, hexamethylmelamine, oral etoposide, tamoxifen, gemcitabine, liposomal doxorubicin, vinorelbine, or topotecan. Multiple clinical factors must be considered when selecting the most appropriate salvage therapy. Unfortunately, in patients previously treated with cisplatin, other therapeutic agents are not likely to be effective in relieving symptoms of bowel obstruction or ascites. A recent retrospective study found that surgery carries a higher morbidity, although chemotherapy and surgery had similar outcomes in terms of reobstruction. However, palliative surgery is usually considered in almost every patient at some time before disease progression and death. When surgery is indicated, the type of surgery depends on the extent of the disease and on the number and location of obstructions. If the obstruction is mainly contained in one area, this area can be either resected (if secondary cytoreduction is indicated) or bypassed. Because the success of secondary cytoreduction depends on the chemosensitivity of the residual disease present after debulking surgery, intestinal bypass is generally preferable rather than resection because most patients present after multiple failed attempts at cytotoxic therapy resulting in chemotherapyresistant cancer. In addition, intestinal bypass surgeries such as enterocolostomy are usually associated with reduced morbidity when compared with a radical resection. At the time of operation, the balloon at the end of a long intestinal tube can often be palpated and used to identify the small bowel proximal to the obstruction. This small bowel can then be anastomosed in a side-toside fashion to the most appropriate area of colon, thus bypassing the site of obstruction.

Cheap zetia 10 mg on-line
This is an uncertain result ldl cholesterol levels chart australia purchase zetia australia, and this patient also needs to be followed should it be revealed in the future that this mutation is actually a deleterious mutation. This is a more common result in minority patients than in white patients because of the lack of information available on minority patients. It is important to maintain records on these patients and continually update them with new information as it becomes available. The impact of genetic information on patients and their families can be tremendous. This accounts for around 40,000 cancers per year, around 5% of which are inherited. Lynch syndrome is a hereditary cancer predisposition syndrome that predisposes individuals to a variety of cancers. As stated previously, endometrial cancer can be inherited in other syndromes and counseling will need to reflect this. The average age of onset of endometrial cancers in women with Lynch syndrome varies but is usually thought to be around 45 to 55 years of age. It is important to identify women with Lynch syndrome so that they can be screened for other cancers. Identification of this syndrome within the family will also allow for increased awareness, diagnosis, screening, and early treatment of other members of the family. One can look for several features that would suggest the likelihood that an inherited problem is present. One of these features is the presence of multiple primary tumors in a single individual. Any woman with both colon and endometrial cancer should undergo evaluation for Lynch syndrome regardless of age. The risk of ovarian cancer in Lynch syndrome may be as high as 12%, although most reports estimate it to be around 5%. Women with both endometrial and ovarian cancer may have a risk of Lynch syndrome in the 7% to 10% range. Therefore women with both ovarian and endometrial cancer should also be considered for evaluation for Lynch syndrome. Negative result Genetic testing for susceptibility in unaffected patients Positive result Test at-risk individual, preferably from a family with a known mutation High-risk screening and intervention Definitive negative Emphasize continued risk of sporadic cancer General population screening for appropriate cancers 592 19. The prevalence of the disease markedly increases if the cancer presents before the age of 50. However, one must be careful in this setting because obesity also increases the likelihood of developing endometrial cancer. Cancer family history in conjunction with personal history of cancer can help assess risk of predisposition for the development of a cancer. This follows the rule of 3,2,1: (1) three relatives with a Lynch-associated cancer (at least one first-degree relative); (2) two successive generations; and (3) one diagnosis under the age of 50. Obviously, the greater and more complete the family history, the more accurate the model. Family history is a valuable tool in identifying individuals and families at risk. However, one must consider that families are now smaller than in the past, there may be poor communication between parts of families, and misattributed paternity, to name a few. If testing is undertaken on the basis of family history alone, then complete molecular evaluation is necessary to assure that that individual is not at risk. Lynch syndrome is interesting among inherited diseases in that it has some very characteristic molecular features that are useful in determining risk of disease and can help in the screening process. More research needs to be undertaken to determine the most cost-effective way to evaluate patients for inherited disease. Some institutions evaluate all patients for inherited disease but recently some reasonable guidelines were established for screening the general population. Patients with synchronous primary endometrial and colon cancer should be screened and screening should be considered if a firstdegree relative has any Lynch-associated cancers. Also, one should consider screening and hysterectomy with bilateral salpingo-oophorectomy should be considered. Even with direct sequencing some types of mutations such as large rearrangements can still go undetected, but this technology is improving. Once a mutation is identified, then site-specific analysis can be performed on the relatives. It is expensive to test each gene, around $1000 per gene, but sitespecific testing is only about $300 to $400. If a negative or variant of uncertain significance occurs, the family history must always be considered and those patients should always have follow-up screening when there is suspicion of Lynch syndrome. Both pre-test and post-test counseling and ongoing counseling should be routinely offered as more data become available. Counseling should include discussion of risks of testing, interpretation of the results, and interpretation of risk based on family history alone irrespective of the results of any tests. Remember that one cannot forget the impact on the rest of the family and counseling should also focus on this group with regard to testing, screening, surveillance, testing, and risk-reducing surgery. There is fear over genetic discrimination in health insurance, life insurance, and disability insurance procurement and even discrimination with regard to employment. These fears include the individual but also affect other family members and are a major reason for not undergoing recommended testing. Almost all states have passed legislation preventing discrimination on the basis of genetic information. Unfortunately, there is wide opinion as to what constitutes genetic information and this opinion varies from state to state. Some states consider family history as "genetic information," whereas others narrow this definition to include only information from genetic testing. This law offers protection of those who are members of group insurance plans, including the federal group plans Medicare and Medicaid. However, the insurance company can raise the rate of an entire group if there is enough risk within that group. Hence, federal law offers some important protection for patients, but this area still needs to be better defined by the courts. Despite the ambiguities in the law, incidents of health care discrimination are very few. There is currently proposed legislation that would broaden protection of individuals with increased genetic risk. Many argue against the legislation as unnecessary because there are currently no data to suggest that any discrimination exists. Again, the actual impact of these laws need to be tested in court and it is therefore difficult to predict exactly what effect these laws will ultimately have on genetic discrimination. Several important points should be considered here: (1) the actual incidence of genetic discrimination is exceedingly small, with few cases nationwide that address this issue, and (2) national sympathy clearly sides with those with the possibility of genetic disease. Nonetheless, part of counseling should include the possibility of discrimination with information gained from the test. It is the duty and obligation of the physician to inform the patient of the risks of a positive genetic test. However, there is also a duty of the physician to inform other family members who are at risk for the disease. However, there is a case litigated in 1996, Safer v Estate of Pack, in which an individual with familial adenomatous polyposis died from colon cancer. Genetic tests are unique in that they affect not only the individual, but may also affect the offspring and other relatives. This further confuses the issue of patient confidentiality and is an issue that will continue to be sorted out as time progresses and other genetic issues are defined by scientific discovery. This is an important part of the counseling process and is one of the reasons most centers recommend counseling before testing. This is defined as what is reasonable or what a reasonable physician should do for his or her patient. Genetic testing and counseling is quite new, and therefore clear standards have not been established.
Ren Shen (Ginseng, American). Zetia.
- How does Ginseng, American work?
- Is Ginseng, American effective?
- What is Ginseng, American?
- Dosing considerations for Ginseng, American.
- What other names is Ginseng, American known by?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96929
Discount 10 mg zetia with visa
Adults not enrolled in monitoring program: subjective change in hearing in the absence of documented hearing loss cholesterol levels reduce naturally order zetia 10mg. Pediatric (on a 1, 2, 3, 4, 6, and 8 kHz audiogram): Threshold shift >20 dB at 8 kHz in at least one ear. Adults enrolled in monitoring program (on a 1, 2, 3, 4, 6 and 8 kHz audiogram): Threshold shift of >25 dB averaged at 2 contiguous test frequencies in at least one ear. Pediatric (on a 1, 2, 3, 4, 6, and 8 kHz audiogram): Threshold shift >20 dB at 4 kHz and above in at least one ear. Adults enrolled in monitoring program (on a 1, 2, 3, 4, 6 and 8 kHz audiogram): Threshold shift of >25 dB averaged at 3 contiguous test frequencies in at least one ear; therapeutic intervention indicated. Endocrine Disorders Grade Adverse Event Adrenal insufficiency 1 Asymptomatic; clinical or diagnostic observations only; intervention not indicated 2 Moderate symptoms; medical intervention indicated 3 Severe symptoms; hospitalization indicated 4 Life-threatening consequences; urgent intervention indicated 5 Death Definition: A disorder that occurs when the adrenal cortex does not produce enough of the hormone cortisol and in some cases, the hormone aldosterone. Delayed puberty - No breast development by age 13 yr for females; testes volume of <3 cc or no Tanner Stage 2 development by age 14. Hyperparathyroidism Mild symptoms; intervention not indicated Moderate symptoms; medical intervention indicated - - - Definition: A disorder characterized by an increase in production of parathyroid hormone by the parathyroid glands. Hypoparathyroidism Asymptomatic; clinical or diagnostic observations only; intervention not indicated Moderate symptoms; medical intervention indicated Severe symptoms; medical intervention or hospitalization indicated Life-threatening consequences; urgent intervention indicated Death Definition: A disorder characterized by a decrease in production of parathyroid hormone by the parathyroid glands. Precocious puberty Physical signs of puberty with no biochemical markers for females <8 yr and males <9 yr Physical signs and biochemical markers of puberty for females <8 yr and males <9 yr - - - Definition: A disorder characterized by unusually early development of secondary sexual features; the onset of sexual maturation begins usually before age 8 yr for girls and before age 9 yr for boys. Virilization Mild symptoms; intervention not indicated Moderate symptoms; medical intervention indicated - - - Definition: A disorder characterized by inappropriate masculinization occurring in a female or prepubertal male. Cataract Asymptomatic; clinical or diagnostic observations only; intervention not indicated Symptomatic; moderate decrease in visual acuity (20/40 or better) Symptomatic with marked decrease in visual acuity (worse than 20/40 but better than 20/200); operative intervention indicated. Conjunctivitis Asymptomatic or mild symptoms; intervention not indicated Symptomatic; topical intervention indicated. Optic nerve disorder Asymptomatic; clinical or diagnostic observations only Limiting vision of the affected eye (20/40 or better) Limiting vision in the affected eye (worse than 20/40 but better than 20/200) Blindness (20/200 or worse) in the affected eye - Definition: A disorder characterized by involvement of the optic nerve (second cranial nerve). Papilledema Asymptomatic; no visual field defects Symptomatic decline in vision; visual field defect present sparing the central 20 degrees Marked visual field Blindness (20/200 or defect (worse than 20/40 worse) in the affected but better than 20/200) eye - Definition: A disorder characterized by swelling around the optic disc. Retinal detachment Asymptomatic Exudative and visual acuity 20/40 or better Rhegmatogenous or exudative detachment; operative intervention indicated; decline in vision (worse than 20/40 but better than 20/200) Blindness (20/200 or worse) in the affected eye - Definition: A disorder characterized by the separation of the inner retina layers from the underlying pigment epithelium. Retinal tear - Laser therapy or pneumopexy indicated Vitroretinal surgical repair indicated Blindness (20/200 or worse) in the affected eye - Definition: A disorder characterized by a small laceration of the retina, this occurs when the vitreous separates from the retina. Retinal vascular disorder - Topical medication indicated Intravitreal medication; operative intervention indicated - - Definition: A disorder characterized by pathologic retinal blood vessels that adversely affects vision. Uveitis Asymptomatic; clinical or diagnostic observations only Anterior uveitis; medical intervention indicated Posterior or pan-uveitis Blindness (20/200 or worse) in the affected eye - Definition: A disorder characterized by inflammation to the uvea of the eye. Watering eyes Intervention not indicated Intervention indicated Operative intervention indicated - - Definition: A disorder of excessive tearing in the eyes; it can be caused by overproduction of tears or impaired drainage of the tear duct. Anal hemorrhage Mild; intervention not indicated Moderate symptoms; medical intervention or minor cauterization indicated Transfusion, radiologic, endoscopic, or elective operative intervention indicated Life-threatening consequences; urgent intervention indicated Death Definition: A disorder characterized by bleeding from the anal region. Ascites Asymptomatic; clinical or diagnostic observations only; intervention not indicated Symptomatic; medical intervention indicated Severe symptoms; invasive intervention indicated Life-threatening consequences; urgent operative intervention indicated Death Definition: A disorder characterized by accumulation of serous or hemorrhagic fluid in the peritoneal cavity. Bloating No change in bowel function or oral intake Symptomatic, decreased oral intake; change in bowel function - - - Definition: A disorder characterized by subject-reported feeling of uncomfortable fullness of the abdomen. Colitis Asymptomatic; clinical or diagnostic observations only; intervention not indicated Abdominal pain; mucus or blood in stool Severe abdominal pain; change in bowel habits; medical intervention indicated; peritoneal signs Life-threatening consequences; urgent intervention indicated Death Definition: A disorder characterized by inflammation of the colon. Colonic hemorrhage Mild; intervention not indicated Moderate symptoms; medical intervention or minor cauterization indicated Transfusion, radiologic, endoscopic, or elective operative intervention indicated Life-threatening consequences; urgent intervention indicated Death Definition: A disorder characterized by bleeding from the colon. Colonic perforation - Symptomatic; medical intervention indicated Severe symptoms; elective operative intervention indicated Life-threatening consequences; urgent intervention indicated Death Definition: A disorder characterized by a rupture in the colonic wall. Diarrhea Increase of <4 stools per day over baseline; mild increase in ostomy output compared to baseline Increase of 4-6 stools per day over baseline; moderate increase in ostomy output compared to baseline Life-threatening consequences; urgent intervention indicated Death Definition: A disorder characterized by frequent and watery bowel movements. Duodenal hemorrhage Mild; intervention not indicated Moderate symptoms; medical intervention or minor cauterization indicated Transfusion, radiologic, endoscopic, or elective operative intervention indicated Life-threatening consequences; urgent intervention indicated Death Definition: A disorder characterized by bleeding from the duodenum. Duodenal perforation - Symptomatic; medical intervention indicated Severe symptoms; elective operative intervention indicated Life-threatening consequences; urgent operative intervention indicated Death Definition: A disorder characterized by a rupture in the duodenal wall. Dyspepsia Mild symptoms; intervention not indicated Moderate symptoms; medical intervention indicated Severe symptoms; surgical intervention indicated - - Definition: A disorder characterized by an uncomfortable, often painful feeling in the stomach, resulting from impaired digestion. Enterocolitis Asymptomatic; clinical or diagnostic observations only; intervention not indicated Abdominal pain; mucus or blood in stool Severe or persistent abdominal pain; fever; ileus; peritoneal signs Life-threatening consequences; urgent intervention indicated Death Definition: A disorder characterized by inflammation of the small and large intestines. Enterovesical fistula Asymptomatic; clinical or diagnostic observations only; intervention not indicated Symptomatic; noninvasive intervention indicated Severe, medically significant; medical intervention indicated Life-threatening consequences; urgent intervention indicated Death Definition: A disorder characterized by an abnormal communication between the urinary bladder and the intestine. Esophageal hemorrhage Mild; intervention not indicated Moderate symptoms; medical intervention or minor cauterization indicated Transfusion, radiologic, endoscopic, or elective operative intervention indicated Life-threatening consequences; urgent intervention indicated Death Definition: A disorder characterized by bleeding from the esophagus. Esophageal perforation - Symptomatic; medical intervention indicated Severe symptoms; elective operative intervention indicated Life-threatening consequences; urgent operative intervention indicated Death Definition: A disorder characterized by a rupture in the wall of the esophagus. Esophageal varices hemorrhage - Self-limited; intervention not indicated Transfusion, radiologic, endoscopic, or elective operative intervention indicated Life-threatening consequences; urgent intervention indicated Death Definition: A disorder characterized by bleeding from esophageal varices. Fecal incontinence Occasional use of pads required Daily use of pads required Severe symptoms; elective operative intervention indicated - - Definition: A disorder characterized by inability to control the escape of stool from the rectum. Gastric hemorrhage Mild; intervention not indicated Moderate symptoms; medical intervention or minor cauterization indicated Transfusion, radiologic, endoscopic, or elective operative intervention indicated Life-threatening consequences; urgent intervention indicated Death Definition: A disorder characterized by bleeding from the gastric wall. Gastric perforation - Symptomatic; medical intervention indicated Severe symptoms; elective operative intervention indicated Life-threatening consequences; urgent operative intervention indicated Death Definition: A disorder characterized by a rupture in the stomach wall. It is chronic in nature and usually caused by incompetence of the lower esophageal sphincter, and may result in injury to the esophageal mucosal. Gastroparesis Mild nausea, early satiety and bloating, able to maintain caloric intake on regular diet Moderate symptoms; able to maintain nutrition with dietary and lifestyle modifications; may need pharmacologic intervention Weight loss; refractory to medical intervention; unable to maintain nutrition orally - - Definition: A disorder characterized by an incomplete paralysis of the muscles of the stomach wall resulting in delayed emptying of the gastric contents into the small intestine. Gingival pain Mild pain Moderate pain interfering with oral intake Severe pain; inability to aliment orally - - Definition: A disorder characterized by a sensation of marked discomfort in the gingival region. Hemorrhoidal hemorrhage Mild; intervention not indicated Moderate symptoms; medical intervention or minor cauterization indicated Transfusion, radiologic, endoscopic, or elective operative intervention indicated Life-threatening consequences; urgent intervention indicated Death Definition: A disorder characterized by bleeding from the hemorrhoids. Hemorrhoids Asymptomatic; clinical or diagnostic observations only; intervention not indicated Symptomatic; banding or medical intervention indicated Severe symptoms; radiologic, endoscopic or elective operative intervention indicated - - Definition: A disorder characterized by the presence of dilated veins in the rectum and surrounding area. Ileal hemorrhage Mild; intervention not indicated Moderate symptoms; medical intervention or minor cauterization indicated Transfusion, radiologic, endoscopic, or elective operative intervention indicated Life-threatening consequences; urgent intervention indicated Death Definition: A disorder characterized by bleeding from the ileal wall. Ileal perforation - Symptomatic; medical intervention indicated Severe symptoms; elective operative intervention indicated Life-threatening consequences; urgent operative intervention indicated Death Definition: A disorder characterized by a rupture in the ileal wall. Intra-abdominal hemorrhage - Medical intervention or minor cauterization indicated Transfusion, radiologic, endoscopic, or elective operative intervention indicated Life-threatening consequences; urgent intervention indicated Death Definition: A disorder characterized by bleeding in the abdominal cavity. Jejunal hemorrhage Mild; intervention not indicated Moderate symptoms; medical intervention or minor cauterization indicated Transfusion, radiologic, endoscopic, or elective operative intervention indicated Life-threatening consequences; urgent intervention indicated Death Definition: A disorder characterized by bleeding from the jejunal wall. Lower gastrointestinal hemorrhage Mild; intervention not indicated Moderate symptoms; medical intervention or minor cauterization indicated Transfusion, radiologic, endoscopic, or elective operative intervention indicated Life-threatening consequences; urgent intervention indicated Death Definition: A disorder characterized by bleeding from the lower gastrointestinal tract (small intestine, large intestine, and anus). Mucositis oral Asymptomatic or mild symptoms; intervention not indicated Moderate pain; not interfering with oral intake; modified diet indicated Severe pain; interfering with oral intake Life-threatening consequences; urgent intervention indicated Death Definition: A disorder characterized by inflammation of the oral mucosal. Oral hemorrhage Mild; intervention not indicated Moderate symptoms; medical intervention or minor cauterization indicated Transfusion, radiologic, endoscopic, or elective operative intervention indicated Life-threatening consequences; urgent intervention indicated Death Definition: A disorder characterized by bleeding from the mouth. Pancreatic hemorrhage Mild; intervention not indicated Moderate symptoms; medical intervention or minor cauterization indicated Transfusion, radiologic, endoscopic, or elective operative intervention indicated Life-threatening consequences; urgent intervention indicated Death Definition: A disorder characterized by bleeding from the pancreas. Pancreatitis - Enzyme elevation or radiologic findings only Severe pain; vomiting; medical intervention indicated. Rectal hemorrhage Mild; intervention not indicated Moderate symptoms; medical intervention or minor cauterization indicated Transfusion, radiologic, endoscopic, or elective operative intervention indicated Life-threatening consequences; urgent intervention indicated Death Definition: A disorder characterized by bleeding from the rectal wall and discharged from the anus. Retroperitoneal hemorrhage - Self-limited; intervention indicated Transfusion, medical, radiologic, endoscopic, or elective operative intervention indicated Life-threatening consequences; urgent intervention indicated Death Definition: A disorder characterized by bleeding from the retroperitoneal area. Salivary duct inflammation Slightly thickened saliva; Thick, ropy, sticky slightly altered taste saliva; markedly altered. Tooth development disorder Asymptomatic; hypoplasia of tooth or enamel Impairment correctable with oral surgery Maldevelopment with impairment not surgically correctable; disabling - - Definition: A disorder characterized by a pathologic process of the teeth occurring during tooth development. Tooth discoloration Surface stains - - - - Definition: A disorder characterized by a change in tooth hue or tint. Vomiting 1-2 episodes (separated by 5 min) in 24 hr 3-5 episodes (separated by 5 min) in 24 hr Life-threatening consequences; urgent intervention indicated Death Definition: A disorder characterized by the reflexive act of ejecting the contents of the stomach through the mouth.
Syndromes
- Coma
- Failure to thrive (lack of normal growth in children)
- Chronic pulmonary coccidioidomycosis
- X-ray
- You have had unprotected intercourse or method failure (for example, a broken condom) within the past 72 hours, and you do not want to become pregnant
- Blood culture to determine the bacteria causing the infection
- Pregnancy
- Lack of head control when baby is pulled from a lying to a sitting position (head lag)
- Blood clot in the lung
- Miscarriage
Discount zetia 10mg with amex
Cholinesterase measurements are also useful in the diagnosis of poisoning with pesticides that are cholinesterase inhibitors cholesterol test south africa buy generic zetia 10 mg on-line. Case history 19 Eight months after an attack of acute glomerulonephritis, a 38-year-old woman was hospitalized for investigation of progressive bilateral leg oedema. On examination, she was normotensive and exhibited pitting oedema of both ankles and dullness over her lung bases. Her face was pale and puffy and she admitted to frequent minor intercurrent infections. Isoenzyme determination Some enzymes are present in the plasma in two or more molecular forms. These variants are known as isoenzymes and, although they have different structures, they perform the same catalytic function. Different isoenzymes may arise from different tissues and their specific detection may give clues to the site of pathology. Alkaline phosphatase isoenzymes may distinguish between bone and liver disease, especially in patients in whom metastases of bone or liver are suspected. A specific isoenzyme of Proteins and enzymes n An increase in total protein concentration in a serum specimen is usually due to an increase in the globulin fraction and may indicate the presence of a paraprotein. Increased enzyme activities in serum indicate either cell damage or increased cell proliferation. Isoenzymes are forms of an enzyme that are structurally different but have similar catalytic properties. Measurement of the isoenzymes of alkaline phosphatase and creatine kinase is of clinical value. The plasma cells are B lymphocytes transformed after exposure to a foreign (or occasionally an endogenous) antigen. The immunoglobulins are named after their heavy chain type, as IgA, IgG, IgD, IgE and IgM. The Fc end is responsible for interaction with other components of the immune system. Electrophoresis of serum proteins Electrophoresis may be carried out to study a number of protein abnormalities. Immunoglobulins are detected primarily in the gamma globulin area on electrophoresis. Serum should be used for electrophoresis, as the fibrinogen of plasma (consumed during clotting) gives a discrete band that can easily be mistaken for a paraprotein. As the cells multiply the immunoglobulin production becomes large enough to be observed on electrophoresis as a single discrete band. Monoclonal light chains are produced in excess of heavy chains in 50% of cases of myeloma, and in 15% of cases only light chains are found. These light chains are small enough to spill into the urine where they are known as Bence Jones protein. Serum electrophoresis may not show the presence of light chains, and urine electrophoresis after concentration may be required to demonstrate the paraprotein. In the face of increasing synthesis of abnormal immunoglobulins, other bone marrow functions are reduced, and there is a decline in red and white cell and platelet formation and decreased production of normal immunoglobulins. Occasionally, paraproteins are found in patients in whom there is no associated pathology. If an abnormality is detected, then the particular type of immunoglobulin, or indeed of light or heavy chains where these are produced alone, may be confirmed by immunofixation or quantitatively by other means. Increased immunoglobulins Immunoglobulins may be increased non-specifically in a wide variety of infections and also in autoimmune disease. This increased synthesis comes from a number of cell lines, each producing its own specific immunoglobulin. This is because the immunoglobulins produced by individual cell lines are slightly different from each other in terms of size and charge, and so do not migrate to the same place on electrophoresis. Analysis of concentrated urine revealed an excess of free monoclonal light chains. Deficiencies or absence of immunoglobulins Deficiencies or absence of immunoglobulins can occur as a result of infection, genetic abnormalities or the effects of therapy (Table 26. Where the situation is irreversible, replacement therapy has been used, either by addition of immunoglobulin-rich plasma or by the transplantation of bone-marrow-containing competent plasma cells. Skull X-ray showing osteolytic lesions of Immunoglobulins n Electrophoresis of serum may confirm the presence of a paraprotein in a specimen from a patient with a raised globulin fraction. Immunoglobulin measurements can give information on immune deficiency and response to infection Serial study of immunoglobulin levels can be of help in following the progression of disease or in monitoring of treatment. Criteria for prior myocardial infarction Any one of the following criteria meets the diagnosis for prior myocardial infarction: n Development of new pathological Q waves* with or without symptoms; n Imaging evidence of a region of viable myocardium that is thinned and fails to contract, in the absence of a non-ischaemic cause; n Pathological findings of a healed or healing myocardial infarction. These cause narrowing of the arterial lumen, resulting in reduced coronary perfusion, the clinical manifestation of which is chest pain (angina pectoris). If an unstable plaque ruptures, the released contents precipitate the formation of a clot. This process, known as thrombosis, may result in sudden complete occlusion of the affected artery and infarction of the area of myocardium it supplies. Pathologically, it is almost always associ ated with rupture of an atherosclerotic plaque and partial or complete throm bosis of a coronary artery. Pointofcare devices are also available, which allow onsite measurement of tro ponin, but these tests are still relatively expensive. Cardiac biomarkers When myocardial cells die, they break up and release their contents. Troponin is a complex contractile protein comprising of three subunits: C, T and I. The diagnostic sensitivity of troponin reaches 100% 12 hours after onset of symptoms, i. He had previously attended the chest pain clinic and had a 2-year history of angina of effort. The cardiac enzymes historically were creatine kinase, aspartate aminotransferase and lactate dehydrogenase. The metabolic pathways of glycolysis, the Krebs cycle, amino acid synthesis and degradation, and the processes of oxidative phosphorylation are all carried out in the hepatocytes, which are well endowed with mitochondria. The liver contains an extensive reticuloendothelial system for the synthesis and breakdown of blood cells. Liver cells metabolize, detoxify and excrete both endogenous and exogenous compounds. Excretion of water-soluble end products from the metabolism of both nutrients and toxins, and of digestive aids such as bile acids, occurs into the biliary tree. Knowledge of the serum albumin concentration may also be of some value in the investigation of liver disease. It is insoluble in water and is transported in plasma almost totally bound to albumin. It is taken up by liver cells and conjugated to form mono- and diglucuronides, which are much more soluble in water than unconjugated bilirubin. Normal bile contains bilirubin monoglucuronide as 25% and the diglucuronide as 75% of the total, accompanied by traces of unconjugated bilirubin. The main functional constituents of the bile are the bile salts, which are involved in fat digestion and absorption from the small intestine. Serum bile acid concentrations are more sensitive indices of hepatic transport function than are total bilirubin measurements. In the terminal ileum and colon the bilirubin conjugates are attacked by bacteria to form a group of compounds that are known collectively as stercobilinogen, most of which are excreted in faeces. Some are absorbed and eventually re-excreted from the body by way of bile (the enterohepatic circulation). Small amounts of these tetrapyrroles are found in urine in which they are known as urobilinogen. They do not assess quantitatively the capacity of the Canaliculus Serum total bilirubin concentration and serum alkaline phosphatase activity are indices of cholestasis, a blockage of bile flow; the former is also a marker of parenchymal liver disease.
10 mg zetia
Anecdotally cholesterol risk factor generic 10 mg zetia, transfusion therapy for severe anemia has often been associated with substantial improvement in fatigue. As compared to other cancers, gynecologic cancers are especially known for being associated with severe anemia, with hemoglobin levels less than 9. Not only does anemia have a significant correlation with poor performance status, but it also may be implicated in tumor sensitivity to radiation and chemotherapy. It has been suggested that an optimal oxygen level for tumors to respond to therapy is reflected by a hemoglobin level between 12 and 14 g/dL. Those patients with an increase in hematocrit of more than 6% also demonstrated significant improvement in energy level and daily activities. Whereas Aranesp has a longer half-life and therefore may be given at shorter intervals, there are few clear advantages compared to Procrit. Therefore, currently, patients with cancer may be counseled about the risks and benefits of the use of growth factors for the correction of anemia and now a potential progression and survival disadvantage needs to be included. Many of the pharmacologic therapies for fatigue associated with medical illness have not been rigorously 20. Psychostimulants, such as methylphenidate, pemoline, and dextroamphetamine, have been well studied for the treatment of opioid-related somnolence and cognitive impairment and depression in elderly and medically ill patients. There are no controlled studies of these drugs for cancer-related fatigue, but empiric administration may yield favorable results in some patients. A clinical response to one drug does not necessarily predict a response to the others, and sequential trials may be needed to identify the most beneficial therapy. Methylphenidate has been more extensively evaluated in the cancer population than other stimulant drugs and is often the first drug to be administered. Pemoline has less sympathomimetic activity than other psychostimulants but has a low risk of severe hepatotoxicity compared with similar agents. It is available in a chewable formulation that can be absorbed through the buccal mucosa for patients who are unable to swallow or take oral medications. Adverse effects associated with the psychostimulants include anorexia, insomnia, tremulousness, anxiety, delirium, and tachycardia. To ensure safety, slow and careful dose escalation should be undertaken to minimize potential adverse effects. A regimen of methylphenidate, for example, usually begins with a dose of 5 to 10 mg once or twice daily (morning and, if needed, midday). Most patients appear to require less than 60 mg/day, but some require much higher doses. Given the limited experience in the use of these drugs for this indication, an empirical trial should be considered only in severe and refractory cases. Amantadine has been used to treat fatigue in patients with multiple sclerosis, but it has not been studied in other patient populations. This drug is usually well tolerated, and an empirical trial may be warranted in selected patients with severe refractory cancer-related fatigue. Nonpharmacologic approaches for the management of cancer-related fatigue are supported mainly by favorable anecdotal experience (Table 20-8). In particular, sleep hygiene principles should be tailored to the individual patients and might include the establishment of a specific bedtime, wake time, and routine procedures before sleep. Patients should also be instructed to avoid stimulants and central nervous system depressants before going to sleep. Regular exercise performed at least 6 hours before bedtime may improve sleep, whereas napping in the late afternoon or evening may worsen it. Referral to a dietitian for nutritional guidance and suggestions for nutritional supplements may be useful. Pain Cancer pain can be managed effectively through relatively simple means in up to 90% of the 8 million Americans who have cancer or a history of cancer. Although cancer pain or associated symptoms cannot always be eliminated, proper use of available therapies can effectively relieve pain for most patients. Restrictive regulation of controlled substances Problems of availability of treatment or access to it Modified from Management of Cancer Pain: Adults. State and local laws often restrict the medical use of opioids to relieve cancer pain, and third party payers may not reimburse for a noninvasive pain control treatment. Thus clinicians should work with regulators, state cancer pain initiatives, or other groups to eliminate these health care system barriers to effective pain management (Table 20-9). Thorough discussions with patients and their families encouraging them to be active in pain management are critical (Table 20-10). Effective treatment strategies exist, but patients often need reassurance to report pain. The goal of the initial assessment of pain is to characterize the pain by location, intensity, and etiology. This can be accomplished through a detailed history, physical examination, social assessment, and diagnostic evaluation. To enhance pain management across all settings, clinicians should teach patients to use pain assessment tools in their homes. Changes in pain patterns and the development of new pain should trigger diagnostic evaluation and modification of the treatment plan. This includes pain resulting from a bone fracture or impending fracture, brain or epidural metastases, infection, or obstructed or perforated viscous. Even within the same family of analgesic drugs, individual variations in tolerability and side effects are well recognized. The simplest dosage and schedule and the least invasive pain management modality should be attempted first. Ask for patient and family cooperation in establishing the effective level when administering medications to prevent long-term cancer pain on an around-the-clock basis with additional doses ("as needed" and usually required). Oral administration is preferred because it is convenient and usually cost effective. Rectal administration is a safe, inexpensive, and effective route for the delivery of opioids and nonopioids when patients have nausea or vomiting. Rectal administration is inappropriate for the patient who has diarrhea, anal/rectal involvement, or mucositis; who is neutropenic; who is physically unable to place the suppository in the rectum; or who prefers other routes. Transdermal administration is also feasible but does not allow rapid dose titration. The opioid may be administered orally or via a dedicated portable pump to deliver the drug intravenously, subcutaneously, or epidurally (intraspinally). Intraspinal administration should be considered for the patient who develops intractable pain or intolerable side effects from other routes of administration. Use of this route requires skill and expertise that may not be available in certain 610 20. This route is often efficacious because gynecologic tumors often affect the pelvis, making profound analgesia frequently possible without motor or sympathetic blockade. Drugs and routes of administration that are not recommended for the management of cancer pain are summarized in Table 20-14. This includes a dose of medication that sustains pain relief for the full time period before the next dose. A sustained dose with an around-the-clock medication should be started in addition to an as-needed medication. The around-the-clock and as-needed doses are increased based on the severity of the uncontrolled pain. Of note, pure opioid preparations are preferred to eliminate the risk of overdosing acetaminophen or ibuprofen. The "as-needed" medication should be about 10% to 20% of the sustained total 24-hour dose. Of note, before converting to a transdermal approach, the pain should be relatively well-controlled by an oral shortacting opioid. The maximum patch dose is 100 mcg/ hour; however, if a patient requires a higher dose, multiple patches may be used. Although the patch typically lasts for 72 hours, being thin, fever, or heat from external sources such as electric blankets may increase the absorption of the transdermal fentanyl and thus may be contraindications to patch use. Clinicians who follow patients during long-term opioid treatment should watch for potential side effects and administer agents to counteract them.
Buy zetia with american express
Lymph flows unidirectionally from the superficial to the deep plexus and from the subareolar plexus through the lymphatic vessels of the lactiferous duct to the perilobular and deep subcutaneous plexus cholesterol medication types buy zetia online. Lymph flow from the deep subcutaneous and intramammary lymphatic vessels moves centrifugally toward the axillary and internal mammary lymph nodes. It is estimated that about 97% of the lymph flows to the axillary nodes and 3% to the internal mammary chain. Axillary lymph nodes may be divided into three anatomic levels defined in reference to the pectoralis minor muscle. Level I nodes are the axillary vein lymph nodes that lie along the axillary vein from the lateral extent of the pectoralis minor muscle to the latissimus dorsi muscle. In this area, deep to the floor of the axilla, subscapular nodes that lie on the subscapularis muscle are identified. Insulin, cortisol, thyroxine, growth hormone, and prolactin are also required for complete functional development. Minor deficiencies in any one of these hormones can be compensated for by an excess of prolactin. Estrogen influences progesterone production, uteroplacental blood flow, mammary gland development, and fetal adrenal gland function. By the 20th week of pregnancy, most of the estrogen excreted in maternal urine comes from fetal androgens. Serum prolactin rises from nonpregnant levels of 10 ng/mL to term levels of 200 ng/mL. Amniotic fluid prolactin levels are more than 100 times greater than the levels in maternal or fetal blood early in pregnancy. It is not known whether the fetal pituitary gland or the trophoblast secretes the hormone into the amniotic fluid. Elevated levels of estradiol parallel those of prolactin and indicate that estriol may be responsible for increases in prolactin. Although estrogen may initiate prolactin secretion, high levels block its physiologic effects. A decrease in estrogen level after delivery and suppression of the prolactin-inhibiting factor by suckling increase prolactin levels. If breast feeding does not occur, serum prolactin levels decrease to nonpregnant levels in about 1 week. The release of oxytocin from the posterior pituitary gland affects contraction of the duct system, stimulating the delivery of milk to the nipples. However, after 3 to 4 months of breast feeding, suckling appears to be the only stimulus required for lactation. The epithelial ridge that develops into breast tissue undergoes a series of proliferations to form the lactiferous ducts. Primitive breast tissue is under the gonadal control of fetal androgen production, which causes a suppression of breast growth during the period of gestation when the tissue is under the simultaneous influence of increasing levels of growth-promoting estrogen and progesterone. After birth, breast tissue remains dormant until adolescence, when estrogen produces a proliferation of ductal epithelium and progesterone produces rapid growth of the acini. It consists of no single entity and encompasses a histologic spectrum of changes in the breast, some of which are normal and some of which are abnormal. It is a result of fluctuating hormone levels and is most common in premenopausal women between the ages of 20 and 50. It is often associated with pain and tenderness (mastodynia) and tends to be bilateral. Most women will report symptoms during the premenstrual phase of the cycle, which suggests that progesterone 14. However, the proportional effect of both estrogen and progesterone on the cause of benign breast conditions is unclear. Pain results from breast stromal edema, ductal dilation, and associated inflammatory response. The differential diagnosis for breast pain includes other conditions affecting the anterior chest wall, such as intercostal neuralgia, myalgia, and chronic costochondritis. Women with large, pendulous breasts will have associated stretching of Cooper ligaments and associated breast pain. In some studies, reduction of dietary methylxanthines has been associated with symptomatic subjective reduction in pain, tenderness, and palpable nodularity. Other studies have failed to show an effect from decreased consumption of dietary methylxanthines, however. In 1985 the Cancer Committee of the College of American Pathologists published a consensus statement and discouraged the use of the term fibrocystic disease; they prefer the terms fibrocystic changes or fibrocystic condition. Histologically, two changes are noted with fibrocystic change: nonproliferative changes and proliferative changes. The nonproliferative changes include cystic changes with formation of microcysts (2 mm or less in size), macrocysts, and fibrosis. Hyperplasia is proliferation of ductal epithelium, which results in layering of the cells. If atypia is noted, this confers a five-fold increase in breast cancer risk for the patient. Hyperplasia with atypia is the only fibrocystic change associated with an increased risk factor for breast cancer. If atypia is noted on a core biopsy, a surgical excision of the area is recommended because it is thought that there is a 25% chance of finding a coexistent carcinoma. Adenosis is also a proliferative lesion caused by changes in the acini in the distal mammary lobule. Sclerosing adenosis refers to the dense, fibrotic tissue surrounding these small ducts. Papillomas are papillary lesions with a branching fibrovascular core surrounded by epithelium. These lesions are associated with serosanguineous nipple discharge in 25% to 50% of presentations. Intraductal papillomas are rarely associated with carcinoma but require surgical excision to rule out the possibility of misdiagnosis of a malignancy. Management of fibrocystic changes includes regular physical examinations, appropriate imaging, and supportive measures to help control symptoms. Recommendations for use of a good support bra may be helpful, especially in physically active women. Dietary restrictions of methylxanthines may produce subjective improvement in 65% of patients. For vitamin E, the mechanism of action is unknown, although an alteration in serum gonadotropins and adrenal tropines has been shown to occur in patients taking high doses of vitamin E. Diuretic therapy during the premenstrual period has been reported to provide temporary relief and requires cyclical use. Oral contraceptives suppress symptoms of fibrocystic changes in the majority of patients (70% to 90%). Other medications such as danazol (17-norethisterone) in doses of 100 to 400 mg per day should be reserved for patients in whom other agents have been ineffective. A 3- to 6-month course can provide significant reduction in symptoms, and its effect can last several months after its discontinuation. As with other progestogens, the mechanism of its effect on fibrocystic disease is unclear. Brookshaw described 514 patients who had benign breast disease treated with varying doses of danazol for as long as 6 months. For the best results, treatment was necessary for 4 to 6 months at a dose of 200 to 400 mg/day, with a complete response rate of 68%. The effectiveness of tamoxifen was studied by Ricciardi and Ianniruberto with use of 10 mg/day from day 5 to day 25 of the menstrual cycle for 4 months. Sclerosing Lesions Sclerosing lesions have been described by a variety of names, including sclerosing papillary proliferation, nonencapsulated sclerosing lesion, indurative mastopathy, and radial scar. On gross examination, they are irregular, gray or white, indurated with central retraction and have an appearance identical to scirrhous carcinoma. On microscopic examination, the lesion has a stellate configuration and consists of a central, fibrotic core containing entrapped glandular elements. The surrounding breast tissue typically shows varying degrees of intraductal hyperplasia and adenosis. The significance of this lesion relative to subsequent development of carcinoma is controversial. Available evidence suggests that these lesions are part of the fibrocystic complex.
