
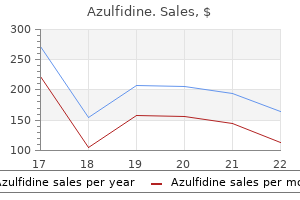
Buy azulfidine on line
While its mode of action is unknown nice guidelines treatment back pain cheap azulfidine 500mg visa, it is not effective unless skin irritation is produced. Dithranol preparations have many problems with stability, which decreases with the strength of the preparations. Addition of salicylic acid, ascorbic acid, or oxalic acid as an antioxidant stabilizes dithranol products and prevents discolouration and inactivation. White soft paraffin appears to be the most stable base, while cream bases are least stable. Dithranol must be protected from light and should be supplied in appropriate light-occlusive containers. It is common for patients to express reluctance to use topical corticosteroids because of misconceptions about the risks of their use. However, more potent corticosteroids may be used intermittently for up to two weeks. The greater the potency the greater the risk of local adverse effects, particularly perioral dermatitis. Calcipotriol Calcipotriol is an analogue of 1,25-dihydroxycholecalciferol, the active form of vitamin D. It is used topically as an ointment or cream in local treatment of plaque psoriasis. The theoretical possibility of hypercalcaemia, renal calculi, and ectopic calcification due to absorption is not a practical problem unless it is applied to large areas of inflamed skin. Calcineurin inhibitors Both pimecrolimus and tacrolimus can be formulated as topical agents. Both agents can be used on the face with minimal risk of aggravating rosacea or inducing perioral dermatitis. Retinoids the term vitamin A refers to a group of compounds that are necessary for cellular differentiation, organ development, and production of the visual pigment in the retina. These compounds also influence immune function and have some anti-inflammatory activity. Acne sufferers can experience some erythema, dryness, and irritation, which can be managed by decreasing the frequency of application or discontinuing the preparation. Patients with sun-damaged skin react more vigorously to topical tretinoin, and its use should be titrated for the individual patient, starting with a daily application for 10 min before washing off. The duration of application can be increased until the preparation is eventually left on overnight. The best results in the treatment of sun damage are not seen until the preparation has been used for six months but include improvement in texture, reduction of pigmentation, removal of Topical corticosteroids the naturally occurring hydrocortisone has anti-inflammatory and immunosuppressive effects, which are useful in treating many skin disorders. Modifications of the hydrocortisone molecule have produced a large number of agents with varying anti-inflammatory potency, which may be used systemically or topically. The potency of topically applied corticosteroids is ranked according to clinical effectiveness and potential for adverse effects (see Table 23. Adverse effects consist of loss of dermal collagen (leading to skin atrophy, striae, fragility, and easy bruising), telangiectasia, and perioral dermatitis. Penetration of corticosteroid to the dermis is greater on the face, the scrotum, and where conditions mimic application under occlusion. The use of the more potent corticosteroids on these sites therefore carries greater risk of local damage and should be avoided. With greater potency, there is increased risk of rebound on withdrawal and of tachyphylaxis. Absorption of more potent agents applied to large areas might cause suppression of the hypothalamic-pituitary axis and other usual complications associated with systemic corticosteroid administration. Topical corticosteroids should not be used on a patient where the diagnosis is uncertain. For example, patients may use topical corticosteroids for years on a groin rash where the diagnosis is tinea cruris, which is curable with correct treatment. Topical isotretinoin and adapalene are used in acne and may also cause drying, erythema, burning, and photosensitivity, but generally these symptoms would be less than with tretinoin. Antiseptics Benzoyl peroxide Benzoyl peroxide has mild keratolytic, antiseptic, and bleaching properties. As irritation is common, caution is needed when applying it near the eyes and other mucosal surfaces. Chlorhexidine Chlorhexidine is a bisbiguanide antiseptic that is commonly used in topical preparations with or without cetrimide. It is used as the acetate, gluconate, or hydrochloride in sprays, creams, gels, solutions, dressings, and powders in concentrations ranging from 0. Chlorhexidine salts may cause skin reactions, irritate mucosal surfaces, and interrupt wound healing. Discolouration of the teeth, tongue, and the buccal cavity associated with chlorhexidine mouthwash or oral gel has been reported. Cetrimide Cetrimide is a quaternary ammonium antiseptic with surfactant properties. It has been used alone or with chlorhexidine in topical preparations in concentrations ranging from 0. Skin sensitivity can occur, particularly with repeated and prolonged applications. Povidone-iodine Povidone-iodine is an iodine complex which has antibacterial, antifungal, and antiviral properties. It is used in mouthwash/gargles, skin cleansers, and antiseptic creams, ointments, solutions, and paints, in concentrations ranging from 5 to 14%. Triclosan Triclosan is a bisphenol antiseptic agent commonly used in medicated soaps and topical preparations in concentrations of up to 2%. Topical imidazole preparations can be irritating but local sensitization is uncommon. Tolnaftate is a thiocarbamate active against dermatophytes but not Candida species. Terbinafine is an allylamine, which inhibits ergosterol synthesis at an earlier stage than the azoles. It is fungicidal for dermatophytes, and is also active against pityrosporum species, but less clearly useful against Candida species. Nystatin and amphotericin are polyenes active against Candida species but not dermatophytes. Various other compounds such as undecenoic acid and the keratolytics benzoic acid and salicylic acid are used to treat tinea. Amorolfine is a morpholine with a broad spectrum, which inhibits ergosterol synthesis at different sites to other antifungals. Many products also include a reflectant, such as titanium dioxide, which increases the protection but can give the skin a white appearance. Zinc oxide is used as a physical sun barrier for the protection of the ears and nose, which often receive high sun exposure. Primary prevention is an important part of the public approach to management of skin cancer. Reduction of sunlight exposure in childhood is critical, but protection during adulthood is also important. The primary approach is natural protection, involving the use of good quality clothing and hats while outdoors, seeking shade where possible, and avoiding the sun around the middle of the day. Imidazole derivatives bifonazole, clotrimazole, econazole, miconazole, and ketoconazole have a broad spectrum of antifungal activity achieved by inhibition of ergosterol synthesis and consequent disruption of the fungal membrane. Lidocaine is used in several products for use on oral and other mucosal surfaces and ulcers. Zinc oxide Zinc oxide is a mild astringent used as a soothing and protective application in dusting powders, pastes, ointments, creams, and lotions, often combined with ingredients such as coal tar, ichthammol, salicylic acid, calamine, or castor oil. It is used for a period of three weeks on the face and on the arms and legs for four to six weeks, although times may vary. It causes severe chemical irritation with erythema and crusting, but heroic patients who complete a course reap significant benefits. If added potency is required, tretinoin can be applied along with the fluorouracil, as the two act synergistically.
Diseases
- Mixed M?llerian tumor
- Lennox Gastaut syndrome
- Neuhauser Daly Magnelli syndrome
- Entomophthoramycosis
- Floating-Harbor syndrome
- Chromosome 12p partial deletion
Buy azulfidine 500 mg with mastercard
The spreading erythema midsouth pain treatment center reviews discount azulfidine 500 mg without a prescription, dull ache, systemic reaction, and the reduction in overlying sensation should alert the physician. Surgical exploration is warranted, which then reveals a necrotic and oedematous reaction in the underlying dermis and deeper fascial planes. Treatment is by early surgical debridement, which is an essential part of management in addition to systemic broad spectrum antibiotics. The lesions develop as nodules that evolve into raised plaques with a black necrotic centre. Tuberculosis of the skin and other mycobacterial infections Mycobacterium tuberculosis is a rare cause of skin infection in most industrialized societies although it remains a regular infection seen in many tropical areas (see Chapter 8. In immune individuals there are usually few organisms, which is described as paucibacillary. In other forms of infection, particularly in those who are immunocompromized, there are many organisms, which is described as multibacillary disease. The term tuberculid is used to describe skin lesions that do not contain viable organisms but that are associated with tuberculosis elsewhere. Usually, but not always, the pathogenesis is through an antigen-mediated reaction. In papulonecrotic tuberculid, the rash is a reaction to disseminated and particulate antigen and, in some cases, viable bacteria are present. The main cutaneous forms of infection seen are tuberculosis verrucosa cutis, scrofuloderma, lupus vulgaris, and papulonecrotic tuberculid. These include Mycobacterium chelonei and Mycobacterium fortuitum which can cause cold abscesses, often as a result of local skin injury, including needlestick injury or surgical or cosmetic procedures. Mycobacterium ulcerans is the cause of rapidly spreading skin ulceration or Buruli ulcer seen in tropical and semitropical areas, ranging from West Africa to south Australia. It is associated with Other bacterial skin infections Gram-negative bacteria, such as a Pseudomonas species, can cause skin lesions. It occurs often in those whose occupations involve wearing heavy footwear or wet working conditions. Often, Gram-negative interdigital infection follows fungal infection (tinea pedis). Gram-negative folliculitis is a painful form of folliculitis presenting with small tender pustules on the trunk and limbs, sometimes associated with fever. Organisms Warty lesions on peripheries Slow spread Purplish plaques over lymph node, often in neck Plaques on face or trunk Heals with central scarring Risk of squamous cell carcinoma Multiple papules, with central area of necrosis, limbs more than trunk No Lymphadenopathy Uncommon Often other sites. It is difficult to arrest the process with antibiotics and the most successful form of management is rifampicin and streptomycin plus surgical excision. Mycobacterium marinum is an infection usually contracted from tropical fish kept in a fish tank (fish tank granuloma); however, naturally acquired infections are seen in the tropics, for example, in association with commercial fishfarming (Chapter 8. It presents with an area of localized pustular swelling, and granulomatous infiltration or ulceration, usually on a peripheral site such as a finger. Treatment with a range of different antibiotics from minocycline to rifampicin has been used. Cutaneous mycobacteriosis: analysis of 34 cases with a new classification of the disease. Treatment of uncomplicated skin and skin infections in the pediatric and adolescent patient populations. The most common of these, dermatophytosis, is seen in all countries, whereas Malassezia infections are more common in the tropics. Candida infections of the skin are less common, but are seen regularly as secondary skin infections. Many drugs and systemic diseases can influence the degree of sweating, such as thyroid disease, infection, carcinoid, and cholinergic drugs. Sebaceous glands form part of the pilosebaceous unit and are found over the entire body surface, with the exception of palms and soles. Acne is a common inflammatory skin disease often associated with significant psychosocial morbidity. An understanding of pathophysiology allows topical and systemic therapies to be combined logically to target therapy. The extent and severity of disease varies, most patients have more than one major site involved but some patients have relatively mild forms of the disease. It is a chronic disabling disease that generally progresses with time and frequently causes scarring, contractures, and significant morbidity for patients. Aetiology and epidemiology the aetiology of hidradenitis suppurativa is unclear; there is a female predominance with a ratio of 3:1 and it is associated with obesity and smoking. Patients of African descent have been reported to have a higher prevalence than Europeans which might reflect the higher density of apocrine glands in black versus white skin. The age of onset ranges from 11 to 50 years, but it is very rare to see hidradenitis suppurativa before puberty or after the menopause. Pathogenesis Hidradenitis suppurativa was first described as a clinical entity in 1839 by Velpeau who described a patient with superficial abscesses in the axillary, perianal, and mammary regions. In 1922 the sweat glands were classified as apocrine and eccrine and it was suggested that hidradenitis was localized to the apocrine glands. Occlusion of the follicular infundibula is the initial event in pathogenesis and a defect of the terminal follicular epithelium is recognized. This is followed by inflammation of the apocrine glands and rupture of the follicles. The disease is sometimes referred to as acne inversa, reflecting the similarities to acne in terms of the follicular occlusion but the locations are inverse to acne and no increase in Disorders of apocrine glands Apocrine glands are compound sweat glands with a secretory coil that extends deep through the dermis into subcutaneous tissue and drains via a long, straight secretory duct, into a hair follicle. Their function in man is not altogether clear, but in other mammals they are responsible for sexual attraction and scent production. A family history of hidradenitis suppurativa is reported in up to 42% of cases and the condition can represent an autosomal dominant inheritance in some kindreds. In animal models alteration in the -secretase gene expression can result in follicular occlusion. Clinical features A consensus approach suggests that three key elements are required to diagnose hidradenitis suppurativa. Typical primary lesions embrace painful and/or tender erythematous papules, painful or tender abscesses, and inflamed discharging papules or nodules, dermal contractures, and rope-like elevation of the skin and doubleended comedones. As a result of associated pain, purulent discharge, malodour and the involvement of sensitive and intimate areas, hidradenitis suppurativa can result in significant morbidity and impact on many aspects of quality of life. Diagnosis and differential diagnosis Some authors have based the diagnosis on several questions, including: Is there more than one inflamed lesion Is the course chronic, are lesions bilateral, and are lesions located to the primary milk line Clinical investigations the diagnosis is primarily a clinical one and diagnostic biopsy is rarely required. Many patients are smokers but smoking cessation does not universally result in improvement of hidradenitis suppurativa. Reducing friction and moist hot environments, together with weight reduction and cotton clothing will help some patients. Localized inflammatory lesions benefit from intralesional injections using triamcinolone (5 mg/ml). Small studies have shown a combination of oral clindamycin (300 mg twice daily) and rimfampicin (600 mg daily) is beneficial. Systemic antibiotics, including erythromycin 500 mg twice each day or minocycline 100 mg daily, are frequently used but topical clindamycin lotion is the only antibiotic that has been shown to be beneficial in a double-blind, placebo-controlled trial. Systemic steroids frequently produce improvement but recurrence is usual on withdrawal. Antiandrogen therapy alone as cyproterone acetate or in combination with ethinylestradiol has been used successfully in some women as has spironolactone; Finasteride, the 5- reductase inhibitor, has also been tried. Isotretinoin produces minimal benefit and the longer acting retinoid acitretin 25 mg daily has shown more promise.
Order discount azulfidine on line
The inflammation is treated with topical steroids of different potencies treatment for dog neck pain purchase azulfidine online from canada, supplemented with moisturizers. Newer therapies include topical calcineurin antagonists, with a range of systemic therapies being used to control the most severe types of disease. The exogenous eczemas are nevertheless the consequence of interactions between external factors and host susceptibility, which may be largely genetically determined. Irritant contact dermatitis Aetiology/pathogenesis Irritants are substances that inflict toxic damage on the epidermis. There are many types of irritant, but from a practical point of view they can be classified as surfactants (soaps/detergents), solvents (petrol, paraffin, oils), caustics (acids, alkalis, chemicals such as phenol), and miscellaneous chemicals that include nonanoic acid and dithranol (used in the treatment of psoriasis). Irritants vary greatly in their potency and hence the level of exposure required to induce an inflammatory response in skin. Individuals also vary greatly in their intrinsic resistance or susceptibility to the effects of irritants. A single exposure to mild irritants such as soaps and detergents is often insufficient to cause a clinically apparent irritant effect, which usually requires multiple exposures having a cumulative effect. The general effect of irritants is a perturbation of the epidermal microenvironment, which is detected as a danger signal. This results in the activation of essential components of the innate immune response. Microscopically, eczematous inflammation shows infiltration of T lymphocytes in both the dermis and epidermis, and the generation of oedema in the dermis, but also particularly in the epidermis. The oedema separates the epidermal cells from each other like the air spaces in a sponge (called spongiosis), but the oedema may coalesce into blisters, giving the appearance of a bubbly surface; these may leak or rupture producing serous oozing and crusting. There are many different types of eczema, some with known causation and others remaining cryptic. Repeated exposure may augment the microscopic response until it becomes clinically apparent inflammation. Most of the changes resulting from cumulative irritant insult are indistinguishable from those that follow the specific immunologically mediated process of allergic contact dermatitis. A survey in Sweden indicated that of 16 600 people who responded to a questionnaire about hand eczema, 11% had experienced eczema in the last year. Thirty-five per cent (35%) of cases were irritant hand eczema, 19% allergic contact dermatitis, and 22% atopic hand eczema. In northern Germany, a large study from 1990 to 1999 examined compensation claims for occupational skin disease. One notable exception is the napkin area of infants, which may be in prolonged contact with alkaline (ammoniacal) urine or faecal material, and can develop irritant napkin dermatitis as a result. The rash is erythematous with poorly defined margins, accompanied by scaling or fissures, and if more severe or acute, by eczematous blisters. Once an irritant dermatitis has been initiated it seems to require very little and only occasional exposure to irritants to maintain a chronic dermatitis. Many patients who try to protect themselves by wearing rubber gloves find that when the hands become sweaty inside the gloves, this actually irritates and aggravates the dermatitis. Those with a past or present history of atopic eczema are significantly more susceptible to developing irritant dermatitis from surfactants and solvents. This may reflect an impaired stratum corneum barrier and/or summation/synergism of the irritant effects and low-level subclinical inflammation of atopic eczema. Treatment the most important principle is avoiding further contact with irritants. Allergic contact dermatitis Aetiology Contact hypersensitivity is an acquired immune response in which T lymphocytes recognize and react to the causative molecules. Contact allergens are mostly small xenobiotic molecules, although under some circumstances proteins can act as contact sensitizers. Several factors are involved in determining whether an individual will develop contact sensitivity to a given molecule. For small molecules to become recognizable by the T-cell receptor, they have first to act as haptens, which become bound to protein carriers. The sensitizing potency of chemicals is generally proportional to their protein-binding reactivity. Some compounds (haptens) are intrinsically protein reactive, others (prohaptens) are converted to protein-reactive metabolites through the actions of phase I xenobiotic metabolizing enzymes such as the cytochrome P450 family. They may either detoxify reactive compounds and prevent immunogenicity, analogous to high acetylator status and resistance to drug allergy, or, possibly through the failure of normal detoxification, may generate protein-reactive immunogenic intermediates. Furthermore, as the sensitizing dose increased, there was a log-linear increase in the strength of the response to the elicitation challenge; in other words, as the sensitizing dose increases on a log scale, so proportionately more people are sensitized, and to a greater extent. For a chemical to induce allergic contact sensitization it must penetrate the stratum corneum. Most sensitizers are lipophilic and hence penetrate readily, but metals such as nickel, cobalt, and chromate are water soluble. Hence a major factor in augmenting sensitization by metals is mechanical penetration of the stratum corneum, as in body piercing. The induction of contact sensitization involves the activation of hapten-specific T cells, which undergo clonal expansion resulting in the establishment of immunological memory. The next time the sensitizer is in contact with the skin it will be recognized by the memory T cells, which respond by releasing interferon- and other proinflammatory cytokines. The combination of cells and cytokines generates the oedema and swelling accompanied by itch that is characteristic of allergic contact dermatitis. Individual susceptibility Very little is known of how individual susceptibility is controlled. There are clearly individuals who develop contact sensitivity to environmental substances more easily than others. Thus individuals who developed contact sensitivity to three or more unrelated chemicals could be sensitized experimentally by 2,4-dinitrochlorobenzene to a much greater degree than individuals with no pre-existing contact allergy. These differences are not qualitative, but reflect the high-responder end of the normal distribution of responsiveness. The corollary of this is that there is a low-responder end of the normal distribution-individuals who appear resistant to the spontaneous development of contact sensitivities, and who give the lowest responses to any given sensitizing dose of 2,4-dinitrochlorobenzene. There do not appear to be any major human leukocyte antigen associations with increased susceptibility to contact sensitization. As indicated here, one level at which susceptibility may be determined is that of intermediate metabolism, which can either detoxify or generate reactive intermediates. A second level, which has been shown at least with regard to nickel sensitivity, is the fundamental control of immunological tolerance, mediated by regulatory T lymphocytes. Prevalence Allergic contact sensitization and dermatitis are common; about 10% of women are sensitive to nickel. The total prevalence of contact dermatitis among the population of many countries is estimated at between 6 and 11%. The incidence of occupational contact dermatitis has been estimated to be around 0. Clinical features of allergic contact dermatitis Allergic contact dermatitis can vary from a low-grade minor nuisance-the pierced earlobes that become mildly inflamed and itchy if the earrings are left in for too long-to catastrophic and disabling acute blistering and weeping with severe oedema of the sites to which the sensitizer was applied. The key points in diagnosis are the recognition that the inflammatory process is eczematous in nature, and that the distribution on the body raises the suspicion that there is an exogenous source. The relationship of these distant areas to contact sensitivity may be much less obvious. Common sensitizers in everyday products include metals; dyes (paraphenylenediamine and other azo dyes) used for ha ir and clothing; preservatives (often formaldehyde releasers, as well as methyl- or chloromethyl-isothiazolinone) found in many personal products; rubber accelerators found in rubber gloves and glue/cement used in shoe manufacture; colophony, extracted from pine resin and used to facilitate adhesion, as in the rubbery adhesive of sticking plasters, but also in mascara and felt-tipped pens; and fragrances used in personal and domestic products. Confirmation of causality Contact allergens are applied to the skin of the back in patch tests. Patients are normally screened by an initial application of 40 substances (some individual, others as mixtures of a class) referred to as the European standard battery. These compounds have been selected by the International Contact Dermatitis Research Group and the European Environmental and Contact Dermatitis Research Group because they represent the groups of the most frequent sensitizers. The patch tests are applied on aluminium disc chambers held in place with hypoallergenic adhesive tape for 48 h, after which the chambers are removed and the skin assessed. Each compound or mixture is used at the highest concentration that does not normally induce a nonspecific irritant reaction. Many centres read the patch tests a second time at 72 or 96 h after application; this is said to reduce the number of false-positive tests that may result from irritant effects, and may detect responses that are slower to evolve.
Buy 500 mg azulfidine with mastercard
Additionally pain treatment centers of america colorado springs discount 500 mg azulfidine visa, in the United States, donated blood is screened for West Nile virus (nucleic acid amplification) and Trypanosoma cruzi as a one-time donor testing. Patient will present with purpura, mucosal bleed, epistaxis, urinary, and gastrointestinal bleeding. Posttransfusion purpura occurs due to the presence of platelet-specific alloantibodies present in patients due to previous sensitizations Table 22. Nucleic acid amplification testing screening has decreased the transfusion-related hepatitis C risk by decreasing the window period to 10 to 20 days. The first cases of transfusion-transmitted West Nile virus infection were documented in the United States of America in 2002; the following year, national blood donation screening for West Nile virus was initiated using nucleic acid amplification testing technology. The risk of transfusion-related transmission of this virus since instituting this screening test has not been established. As for parvovirus B19, only a few cases of transmission by blood components have been reported in immunocompetent recipients. These numbers may, however, be an underestimate of the overall risk of transfusion transmission of this disease. Moreover, a significant number of deceased blood recipients may not have survived long enough to manifest clinical disease even if infected. The introduction of universal leucocyte depletion of the United Kingdom blood supply in 1999 may have reduced the risk to blood recipients. A number of parasitic diseases are known or suspected to be transmitted by blood transfusion. Transmission of Lyme disease (Borrelia burgdorferi) by transfusion has not been documented. Infection with babesia, if untreated, can be dangerous in at-risk populations such as asplenic patients. At this time, blood centres maintain varying algorithms regarding the testing of T. These algorithms range from testing first time donors only, to testing first time donors and retesting donors who report having travelled to endemic areas of Central and South America. Leucocytes are effectively removed from red cell and platelet concentrates by leucocyte reduction filters. Red cells are most commonly leucoreduced shortly after blood collection (prestorage leucodepletion). Apheresis devices have been designed to collect leucoreduced platelets directly (process leucoreduction). Prestorage leucoreduced products are preferable because they contain less cytokines and other biological response modifiers produced by white blood cells. With the dramatic decrease in the risk of viral transmission, investigators are focusing on the immunomodulatory effects of blood transfusion. These effects specifically deal with associations between allogeneic transfusion and bacterial infection, tumour progression, and tumour recurrence. It is not necessary to irradiate frozen noncellular blood products such as fresh frozen plasma or cryoprecipitate because they contain very few viable leucocytes. Bone marrow or peripheral blood stem cells must never be irradiated prior to transplant. Pathogen reduction Transfusion-transmitted infections from known and emerging pathogens pose a risk to the blood supply. With donor screening and use of a donor history questionnaire, coupled with serological testing, and nucleic acid testing, the risk of transfusion-transmitted infections has decreased, but has not been completely eliminated. Newer technologies, such as pathogen reduction, will reduce this risk further by inactivating both intracellular and extracellular agents including viruses, parasites, and bacteria. Advantages of pathogen reduction include the potential to eliminate the need for future additional donor infectious disease testing, decreasing donor deferrals and extending the limited shelf life of platelets to 7 days due to the decreased risk of bacterial contamination with treated platelets stored at room temperature. Other pathogen-reduction technologies are in various stages of development for use with either whole blood plasma or cellular blood components. One licensed pathogen-reduction method targets cell membranes by using a solvent and a detergent to attack and damage the cell membrane of pathogens. This technology is thus applicable only to plasma products and not to cellular blood components. In addition, plasma can be inactivated using riboflavin (vitamin B2) light treatment. Most technologies for pathogen reduction of cellular blood components target nucleic acids, preventing the replication of pathogens and leucocytes. Methods to inactivate infectious pathogens in red cells are currently under development. It is performed for patients with repeated severe allergic/anaphylactic reactions and in neonatal alloimmune thrombocytopenia patients receiving maternal platelets, to remove the maternal alloantibodies. Approximately 20 to 30% of the red bloods cells or platelets are lost during this process. Volume reduction this process is performed by a centrifugation step and the removal of the supernatant to concentrate the product. Volumereduced platelets can be resuspended in saline and should be transfused within 4 h. The indication for platelet volume reduction is transfusion to patients who are prone to circulatory overload, for 22. Albumin, immune globulin, factor concentrates, and other plasma derivatives are treated using solvent/detergent and other protocols that essentially eliminate the risk of viral transmission. Pathogenreduction technologies are safe, nontoxic, and achieve an adequate level of pathogen inactivation while maintaining cellular quality and adequate levels of functional clotting factors. It should be noted that current technologies and most pathogen-reduction technologies currently available and under development are ineffective against spores or prions. The earliest products consisted of stroma-free haemoglobin, which was abandoned because of its renal toxicity, and polymerized haemoglobin. Most of these agents are not used clinically because of vasoactivity and other untoward effects; other formulations are in various phases of clinical trials. Molecular-based typing in the blood bank is referred to as genotyping, as compared to the current gold standard serological typing via haemagglutination known as phenotyping. However, it will not soon replace serological testing because serology is inexpensive and less complex compared with genotyping. Genotyping red cells has its advantages in certain circumstances, for example, to resolve a typing discrepancy, in positive direct antiglobulin testing, after multiple transfusions, when typing reagents are not available for certain blood group antigens, to identify a fetus at risk of haemolytic disease of the newborn, and with patients in need of chronic transfusions with an increased risk of alloimmunizations and matching their blood is problematic. This population of patients includes sickle cell, thalassemia, and oncology patients. Genotyping assays used in the blood bank are polymerase chain reaction-based assays and many platforms have been developed in recent years. In addition to the complexity of these assays, there are approximately 300 antigens identified and more than 1000 alleles coding them. A particular phenotype can result from multiple genetic variations and one should have a full knowledge of the different alleles present in a population prior to developing a molecular-based assay. Alternatives to blood component therapy Autologous transfusion Commonly used forms of autologous transfusion include preoperative blood donation, acute normovolaemic haemodilution, and autologous blood salvage. The criteria for autologous donations are less stringent than those for allogeneic donors. Preoperative blood donation can be utilized in elderly patients, although there is a higher risk of anaemia and more serious cardiovascular complications associated with the donation. Although the use of autologous blood decreases the risk of viral infection, the risk of bacterial contamination remains. Acute normovolaemic haemodilution is performed by removing blood from a patient immediately before surgery and replacing the blood volume with crystalloid or colloid solutions to maintain haemodynamic stability. Autologous blood salvage is performed by collecting and then returning blood lost during or shortly following operative procedures using intraoperative salvage devices.
Cabbage. Azulfidine.
- What is Cabbage?
- Are there safety concerns?
- Are there any interactions with medications?
- How does Cabbage work?
- Stomach pain, stomach and intestinal ulcers, bladder cancer, excess stomach acid, asthma, morning sickness, preventing osteoporosis and cancer, and other uses.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96208

Azulfidine 500 mg
Future treatments might include more targeted therapy such as desmoglein peptides to block the binding sites for autoantibodies treatment pain behind knee purchase azulfidine pills in toronto. A similar clinical picture is seen with staphylococcal scalded skin syndrome where the toxin cleaves desmoglein 1, leading to superficial blisters. Clinical features Erosions and crusting are seen in a seborrhoeic distribution affecting scalp, face, torso, and upper limbs. Diagnosis Histology shows a subcorneal split and immunofluorescence shows antibody deposition in the intercellular space. Pemphigus foliaceus Epidemiology and genetics this is a rare subtype of pemphigus with a sporadic and an endemic form. The endemic form (fogo selvagem) is seen in Brazil, Colombia, and Tunisia, and is thought to be related to insect exposure as it affects individuals living in rural areas near rivers, and resolves when they move away. Pathogenesis Autoantibodies to desmoglein 1 target this component of the adhesion complex that is located in the upper layer of epidermis, below the stratum corneum (subcorneal). Animal studies have confirmed the the treatment is similar to that of pemphigus vulgaris with topical treatment and systemic steroids to achieve remission. Elucidating environmental factors that trigger the endemic disease might lead to better understanding of the disease pathogenesis in future. Paraneoplastic pemphigus Epidemiology and genetics this is a rare subtype of pemphigus that was first recognized as an entity in 1990. Its genetic basis is not well characterized and seems to be different to other subtypes of pemphigus. Clinical features Patients present with severe mucosal erosion and skin eruption involving a large area of the body. There can be involvement of the palms and soles with blisters mimicking erythema multiforme, as well as nasopharynx, genital, and respiratory mucosal erosions. There is often multiorgan involvement and the patients are unwell with respiratory failure as the usual cause of death. Diagnosis Histology shows intraepidermal cleavage and possibly basal cell necrosis and is not diagnostic. Direct immunofluorescence of uninvolved skin shows both intercellular and intraepidermal desposition of antibodies. A substrate with transitional epithelia such as rodent bladder (devoid of desmogleins) is used in indirect immunofluorescence to confirm the presence of antibodies to plakins. Treatment and prognosis the disease is resistant to treatment but might improve if the underlying malignancy is treated. The association of bullous pemphigoid with cerebrovascular disease and dementia: a case-control study. Chronic bullous disease of childhood, childhood cicatricial pemphigoid, and linear IgA disease of adults: a comparative study demonstrating clinical and immunopathologic overlap. The differential diagnosis includes psoriasis, lichen planus, mycosis fungoides, discoid lupus erythematosus, eczema/dermatitis, drug eruptions, tinea, pityriasis versicolor, secondary syphilis, and pityriasis rosea. The presence of significant pruritus is a useful marker to help with the differential diagnosis: lichen planus and discoid eczema are typically pruritic, whereas others, such as psoriasis, are less so. The distribution is also key to diagnosis, with psoriasis often showing characteristic symmetrical involvement of the extensor surfaces, scalp, and nails. Histology can be essential to reach a diagnosis and plan an appropriate approach to management. The most common form of psoriasis is chronic plaque psoriasis, which often first affects the scalp. Systemic treatments, including biological therapies, are only required in the most refractory cases. Lichen planus is characterized by purple (violaceous) flat-topped polygonal papules that vary in size, most commonly on the flexor aspects of the wrists, the lower back, and the ankles. Early-onset, type I psoriasis is familial; one-third of patients have a first-degree relative with the disease. It is apparent that this form of psoriasis is genetically predetermined and polygenic. Twin studies underscore the importance of an interaction between environment and genotype for the expression of psoriasis, and concordance is 72% in monozygotes. The characteristic features are well-circumscribed red plaques covered with silvery-white scales. Plaques are frequently strikingly symmetrical, varying in diameter from less than 1 cm to more than 10 cm. Individual plaques are dynamic, such that in active disease a plaque may clear from the centre to leave an annular or gyrate configuration that to the uninitiated could be misdiagnosed as tinea corporis. Various phenotypes of psoriasis exist: Guttate psoriasis Named from the Latin guttata, meaning a droplet. Onset is acute, with a predominantly centripetal Psoriasis Psoriasis is one of the most common and easily identifiable inflammatory skin diseases. In Western Europe its prevalence is estimated at 2%, but is higher in parts of Scandinavia. Worldwide, the disease is rare in Inuit, Native American, Japanese, and Afro-Caribbean people, and has been estimated to affect just 0. There is no evidence that the incidence of the disease is changing, by contrast with the year-on-year increase in atopic dermatitis. Other diseases producing erythroderma include atopic dermatitis, lichen planus, drug eruptions, and cutaneous T-cell lymphoma. Erythroderma, particularly in older people, can lead to fluid loss, hypocalcaemia, impaired thermoregulation (both hypo- and hyperthermia), and high-output cardiac failure. This form of psoriasis is usually precipitated by infection or acute withdrawal of either systemic glucocorticosteroids or, on occasion, high-potency topical corticosteroids, leading to a rebound pustular flare. Recent evidence indicates that generalized pustular psoriasis is more akin to the autoinflammatory diseases and should more accurately be termed generalized pustulosis, rather than as a variant of chronic plaque disease. It has been linked to a genetically determined deficiency in interleukin-36 receptor antagonist. Flexural psoriasis Flexural psoriasis (psoriasis inversa) pertains to a form that involves the groins, axillae, and inframammary regions. Psoriasis at these sites loses many of the characteristic clinical features, in that it is shiny, nonscaly, and bright red, but retains the characteristic clear demarcation between involved and uninvolved skin. Scalp the scalp is often the first and sometimes the only site to be affected by psoriasis. Koebner phenomenon the appearance of psoriasis at sites of recent trauma or pressure to the skin, such as under a tight waistband, is known as the isomorphic or Koebner phenomenon. Although not unique to psoriasis (it occurs also in lichen planus, viral warts, sarcoid, and vitiligo) it is a clinical marker of active, progressive disease. Nails Approximately 50% of patients with psoriasis have characteristic clinical involvement of any one or up to all the finger and toe nails. The involvement of the skin of the fingers by psoriasis, and the presence of psoriatic arthritis, predispose to nail disease. Patients are frequently concerned about nail disease, and may request treatment for this aspect of psoriasis alone. Palmoplantar pustulosis Now believed to be a condition separate from psoriasis, palmoplantar pustulosis has been reclassified as a co-morbid condition. Yellow sterile painful pustules occur on the palms and soles, fading to brown scaled lesions. This is a disease of middle-aged women (female:male ratio 9:1), and more than 95% are current or previous smokers. Psoriatic arthritis this seronegative inflammatory arthritis occurs in more than 25% of patients with psoriasis. Most cases present either concomitantly with or after the first signs of skin disease, but on occasion (<10%) the arthritis predates psoriasis. A characteristic, perhaps pathognomonic, radiological feature is the presence of enthesitis- inflammation of a tendon sheath, particularly the Achilles. The immunogenetics of psoriatic arthritis are different from those of psoriasis, implying that the underlying pathogenic mechanisms are separate. It is currently unknown whether these signs are a consequence of psoriasis per se or of chronic inflammation, as is the case with arthritis. Indeed weight gain can be a precursor of the development of psoriasis and the presence of psoriatic arthritis significantly increases the risk of cardiovascular disease. Psychosocial aspects Psoriasis is associated with significant impairment of quality of life.
Purchase azulfidine in united states online
Progression and prognosis in multiple system atrophy: an analysis of 230 Japanese patients pain medication for dogs human buy genuine azulfidine online. So much so that it is generally (and often incorrectly) assumed to be understood, especially by doctors. The classification of headache, with formal definitions of different diagnostic entities, by the International Headache Society into (1) primary-occurring in the absence of external causes, and (2) secondary- some of which may have sinister cause, has greatly simplified the description, understanding, and management of this often challenging symptom. It also allows those headaches with serious or life-threatening consequences to be distinguished from other forms. Pathophysiology of primary headaches the key structures involved in producing pain appear to be the: (1) large intracranial vessels and the dura mater, (2) trigeminal nerve, (3) higher centres in the thalamus and cortex, (4) modulatory centres in the diencephalon and brainstem. Two of the most common and best studied primary headaches, migraine, and cluster headache, should be regarded as being neurological or brain disorders with any vessel change being secondary, ie neurovascular. Migraine might be part of the spectrum of diseases known as channelopathies or ionopathies: the three genes currently identified as being responsible for familial hemiplegic migraine alter ion fluxes. Moreover, in studies of the more common forms of migraine across large patient cohorts, genome-wide association studies have implicated excitatory, in particular glutamatergic, transmission to be key to the pathophysiology. Most migraine sufferers will benefit from a healthy diet, regular exercise, regular sleep patterns, avoiding excess caffeine and alcohol and (as far as practical) modifying or minimizing changes in stress. Tension-type headache Tension-type headache is common, unexplained, and completely featureless, with no nausea, no vomiting, no photophobia, no phonophobia, no osmophobia, no throbbing, and no aggravation with movement. When episodic, it is generally amenable to simple analgesics; when chronic, amitriptyline is the only proven treatment. Migraine Epidemiology and clinical features-migraine affects 12 to 18% of the population in any one year, and about 45% of females over their lifetime; it can be highly disabling. It presents with headache, often throbbing and generally accompanied by other features such as sensitivity to light, sound, or movement, and often with nausea or (less often) vomiting, but none of the features is compulsory. For example, the migraine aura-visual disturbances with flashing lights or zigzag lines moving across the fields or other neurological symptoms-is reported in only about 25% of patients. It is noteworthy that the word migraine is used to describe the diagnosis-a patient has migraine; as well as an individual attack-a patient is having a migraine. Prevention is with agents including verapamil, lithium, topiramate, and melatonin, while oral corticosteroids are used as bridge therapy. Treatments for acute attacks include oxygen inhalation, sumatriptan by subcutaneous injection, or nasal spray and zolmitriptan by nasal spray. Other primary headaches Specific conditions include (1) cough headache, (2) exercise headache, (3) sex headache, (4) thunderclap headache, (5) cold stimulus headache, (6) external pressure headache, (7) stabbing headache, (8) nummular headache, and (9) hypnic headache. Many of these can present with daily headache and are often misdiagnosed as tension-type headache. They can readily be identified from the history, often leading to effective and specific treatments, an important element of which is reduction/elimination of analgesic overuse. New daily persistent headache- this presents with abrupt onset of headache that then persists. Possible causes include: (1) primary- migrainous type, featureless (tension-type); (2) secondary- subarachnoid haemorrhage, low cerebrospinal fluid volume headache, raised cerebrospinal fluid pressure headache, posttraumatic headache, chronic meningitis, giant cell arteritis. Effective and specific treatments are available for many of these conditions if a precise diagnosis can be made. A formal nosology for headache disorders is to be found in the third edition of the International classification of headache disorders. Although it seems obvious, the key to successful management is establishment of a clear diagnosis. The general concept is that there are primary and secondary forms of headache, following the generic medical principle that clinical syndromes may be caused by something exogenous or secondary, or may manifest anew as the primary disease process. Mild secondary headache, such as that seen in association with upper respiratory tract infections, is common but only rarely worrisome. The clinical dilemma remains that, although life-threatening headache is relatively uncommon in Western society, it occurs, and its detection requires suitable vigilance by doctors. Primary headache, in contrast, often confers considerable disability over time and although not life-threatening certainly robs patients of quality of life. Primary headache disorders the primary headaches are a group of fascinating disorders in which headache and associated features are seen in the absence of any exogenous cause. Some other less well-known, indeed rarer, syndromes are mentioned because they are easily treated when diagnosed, and the most burdensome headache problems, the chronic daily headache syndromes, are explicitly covered because concepts have altered considerably in this area in recent years. Secondary headache Clinical approach-the length of the history is crucial: if this is short, the patient requires prompt attention; if this is long, then time and patience are needed rather than alacrity. Associated fever, sudden onset of pain, or the presence of neurological signs need a positive diagnosis of a benign disorder or require brain imaging with computed tomography or magnetic resonance imaging. Causes and management-medically sinister headaches requiring urgent attention include subarachnoid haemorrhage, meningitis, giant cell arteritis, and raised intracranial pressure. Other important causes of secondary headache include low volume (pressure) cerebrospinal fluid, post-traumatic headache, and cerviocogenic headache. Many of these disorders require persistent diagnostic skills and investigation; but when combined with knowledge of general principles, including the anatomy and physiology of the key cranial structures, the management of headache is generally productive and beneficial for the sufferer. Anatomy and physiology the most common disabling primary headaches, migraine, and cluster headache, have been studied extensively in recent times and they are now relatively well understood insofar as neurological disorders that involve the brain are concerned. In experimental animals the detailed anatomy of the connections of the pain-producing intracranial extracerebral vessels and the dura mater has built on the classic human observations of Wolff, Feindel, Penfield, McNaughton, and others. It is these structures, and not the brain itself, that are primarily involved in head pain, although it is not at all clear to what extent there is nociceptive activation as such, or simply the perception of that activation. General principles To manage headache can be a source of extreme frustration or undiluted pleasure-the difference simply reflects to what extent Table 24. Cranial parasympathetic autonomic outflow from the superior salivatory nucleus through the seventh cranial nerve and peripherally through the sphenopalatine ganglion, provides the basis for symptoms such as lacrimation and nasal stuffiness, which are prominent are lateralized in cluster headache and paroxysmal hemicrania, although they may also be seen in migraine. It is clear from human functional imaging studies that vascular changes in migraine and cluster headache are driven by these neural vasodilator systems so that these headaches should be regarded as neurovascular. These findings and the clinical features of migraine suggest that it might be part of the spectrum of diseases known as channelopathies, or now ionopathies-disorders involving dysfunction of ion channel fluxes. Diagram of some structures involved in the transmission of trigeminovascular nociceptive input and the modulation of that input which form the basis of a model of the pathophysiology of migraine. These influences are pictured as being direct but both direct and indirect projections are recognized. Secondary headache It is imperative to establish in the patient presenting with any form of head pain whether there is an important secondary headache declaring itself. The headaches of subarachnoid haemorrhage, meningitis, giant cell arteritis, and raised intracranial pressure are important examples of medically sinister headaches requiring urgent attention. Patients with a short history require prompt attention and may require prompt investigation and management. In the premonitory phase hypothalamic activation is observed (a), while consistently in the headache phase there is dorsolateral pons activation in episodic migraine without aura, triggered by nitroglycerin (b), or spontaneously studied (c), and in chronic migraine (f). Moreover, there is lateralization to the right (d) and left (e) in this structure that parallels the unilateral presentation of the pain. There are some important general features, including associated fever or sudden onset of pain (see Box 24. In general, it should be noted that brain tumour is a rare cause of headache, and rarely a cause of isolated long-term histories of headache. A notable exception to the general rules about secondary headache is a pituitary tumour, which can frequently trigger underlying primary headache biology, and should always be considered, especially in the differential diagnosis of trigeminal autonomic cephalalgias (see next). The management of secondary headache is generally selfevident: treatment of the underlying condition, such as an infection or mass lesion. An exception is the condition of chronic post-traumatic headache in which pain persists for long periods after head injury. None of the features is compulsory, and indeed, given that the migraine aura, visual disturbances with flashing lights or zigzag lines moving across the fields, or other neurological symptoms, are reported in only about 25% of patients, a high index of suspicion is required to diagnose migraine. In a controlled study of patients presenting to general practitioners with a main complaint of headache over the previous 3 months, migraine was the diagnosis on more than 90% of occasions, so a high index of suspicion is well rewarded. A headache diary can often be helpful in making the diagnosis, although in reality the diary usually helps more in assessing disability or recording how often patients use acute attack treatments.
Cheap azulfidine 500 mg without a prescription
Toxoplasmosis produces multiple enhancing solid or cavitating nodules with oedema not distinguishable from other bacterial or fungal infections pain medication for dogs and humans order on line azulfidine. Cryptococcal infection causes meningitis and imaging may be normal or enlargement of the perivascular spaces may be seen because this fungus produces a mucoid material. Dementia imaging this is an area of increasing interest due to the ageing population. The purpose of imaging is twofold; firstly, to identify any intracranial pathology that may mimic a dementing illness, and secondly, to assist with distinguishing different neurodegenerative processes that lead to dementia. Some patients present with cognitive impairment without a focal neurological deficit, but have pathology readily identified with imaging. Some examples include a large frontal meningioma, or an infiltrating primary brain tumour, or chronic subdural haematoma, or obstructive hydrocephalus. However, because cerebrospinal fluid escapes from the fourth ventricle and circulates round the spinal cerebrospinal fluid spaces, it means that it is safe to perform a lumbar puncture to measure and, if appropriate, lower cerebrospinal fluid pressure. Congenital anomalies and paediatric imaging Any detailed discussion of this subject is beyond the scope of this chapter, and the reader is directed to specialist texts (see also Chapter 24. It provides the most information and avoids exposure of young patients to ionizing radiation. The main drawback in this age group is the need for sedation or general anaesthesia. The most common indication for imaging in such patients is developmental delay or seizure disorders. It also plays a vital role in the imaging of a suspected, neonatal, hypoxic ischaemic insult, and in elucidating the cause of cerebral palsy. A wide variety of congenital anomalies is possible, ranging from minor abnormalities of neuronal migration, or localized areas of dysplastic cortex, to major anomalies of the whole brain and encephaloceles, in which there is an associated defect of the skull or spine such as a spina bifida. The most frequent is the Chiari 1 malformation of the posterior fossa associated with cerebellar ectopia. The cerebellar tonsils, classically peg-shaped, extend below the foramen magnum a distance of at least 5 mm. Summary and possible future developments Modern imaging techniques have revolutionized the diagnosis of neurological disease in the last 30 years. The contribution of these techniques to the efficient and effective diagnosis of intracranial and spinal pathology, together with the ability to effectively exclude structural disease, has had a huge impact on neurological and neurosurgical clinical practice. In addition, the development of endovascular interventional neuroradiological techniques for the treatment of vascular diseases of the brain 24. Some magnetic stimulators produce a predominantly monophasic field pulse, others multiphasic pulses; with the former, the side of the coil next to the scalp determines which hemisphere is predominantly excited, whereas with the latter both hemispheres are about equally excited. Physiology If a single electrical anodal shock is applied to the exposed cortex of a monkey and recordings are made from the pyramidal tract, it is seen that, if stimulus intensity is sufficient, an initial wave produced by direct activation of pyramidal tract neurons (the D wave) is followed by a variable number of other waves produced by indirect trans-synaptic activation (I waves) of the same pyramidal neurons. In humans a single weak magnetic stimulus to the scalp probably excites pyramidal tract cells trans-synaptically; stronger stimuli may excite the cells directly. There is considerable convergence and divergence of pyramidal tract fibres within motoneuron pools: single spinal motoneurons receive many corticospinal inputs and, conversely, single pyramidal tract fibres branch to supply many spinal motoneurons. Intrinsic hand muscles are the most easily excited by brain stimulation, but all voluntary muscles appear to be accessible via cortical stimulation. The amplitude of response of a muscle depends on the intensity of the stimulus, to a lesser extent on coil placement on the scalp, but most potently on the degree of voluntary preactivation of the muscle. This facilitation is probably due to both cortical and spinal cord mechanisms, voluntary action increasing the effectiveness of the stimulus at the cortex, at the same time as the excitability of spinal motoneurons is increased by other pathways. Clearly, many factors, including mental set, affect the size of muscle response to the stimulus, and it should be emphasized that this phenomenon of response variability contrasts with the identical and reproducible responses obtained from maximal electrical peripheral nerve shocks; central motor conduction studies should not be regarded simply as an extension of nerve conduction measurements. Single scalp shocks also bring into play inhibitory mechanisms: if an individual maintains a steady voluntary muscle contraction, the initial excitation caused by the stimulus is followed by a silent period, due to the inhibition of voluntary action. Magnetic stimulators are now available that can excite both upper and lower limb areas of the motor cortex, as well as cranial nerves, motor roots, and deeply sited peripheral nerves. The technique can be used serially to monitor progress of disease or after neurological injury or to examine the effects of drugs, and it can be used safely in neonates and children. Magnetic stimulators the magnetic stimulator is an essentially simple device: a brief pulse of electric current is passed through a coil which then generates an intense magnetic field permeating unattenuated into the surrounding media. Any electrical conductor, such as the brain, in the vicinity of the coil will have currents induced within it; these induced currents are capable of exciting cerebral neurons. This has proved clinically useful in serially monitoring amyotrophic lateral sclerosis. Safety of magnetic stimulation Several studies have looked at the acute effects of magnetic stimuli on animals. It has been shown that magnetic stimuli have little detectable effect on the heart rate, arterial blood pressure, or cerebral blood flow in cats. Magnetic brain stimulation has no acute effects on the human electroencephalogram or on the performance of simple cognitive tests. There have currently been no reports of adverse effects in healthy humans, but, clearly, workers in the field should remain vigilant, especially for long-term effects. It has been calculated that the total amount of power dissipated in the brain during magnetic stimulation is 1. It was considered prudent for early users of magnetic stimulation to exclude patients who had a history of epilepsy from their studies. Since then, magnetic stimulation has actually been used to attempt to localize epileptic foci in patients with intractable seizures. Despite magnetic stimulation devices being used on many thousands of patients, many of whom must have had a predilection for epilepsy, there have been only a few reports of a fit being related to singlepulse brain stimulation. Both devices activate motor roots at or just outside the intervertebral foramina, and so peripheral conduction time estimated by this method omits conduction in the small segment of motor root within the spinal canal, and central motor conduction time is slightly overestimated. Compound responses from muscle may be recorded with surface electrodes, or single motor unit responses may be recorded with needle electrodes; the former method is used clinically, the latter is useful in research. Several parameters of the surfacerecorded response are useful: the maximum amplitude, the onset latency with the muscle relaxed or contracted, the threshold for evoking a response and the input:output relation giving a measure of cortical excitability or inhibitability. Prolongation of central motor conduction time has been reported in many conditions and is not specific. Delay can be produced by a variety of pathological processes: demyelination of central fibres can lead to slowing of impulse propagation in the central motor pathway; desynchronization of descending impulses can lead to loss of temporal summation at the motoneuron and delay in its firing; and loss of corticospinal axons can lead to impairment of spatial summation at motoneurons and can again delay firing. The delay in some cases is very considerable: central motor conduction time may be up to five times longer than in controls. It is likely that, in these cases, demyelination of central fibres is the mechanism leading to delay. In other cases, delay is more modest, only a few milliseconds, Wrist C7/T1 Cortex Measurement of central motor conduction time the latency of muscle response has a central and a peripheral component and a delay due to synaptic transmission in the spinal cord. There is good evidence that, at least with limb muscle, the connection from the pyramidal tract to spinal motoneuron is monosynaptic. The central component of conduction-central motor conduction time-can be estimated by subtracting from the cortex to muscle latency an estimate of the peripheral conduction time obtained either from F-wave measurement (see Chapter 24. The amplitude of responses from brain stimulation is usually compared with that obtained from maximal peripheral nerve stimulation; again, there is great variability, but in healthy individuals the response from cortical stimuli is usually at least 15% of that from nerve stimulation. As many factors can influence these values, each laboratory should develop its own normative database. The former method is preferable because it is not possible to obtain maximal responses in all healthy individuals with magnetic coils, even with optimal coil geometry, coil orientation, and 25. Compound muscle action potentials are recorded with surface electrodes over the left and right abductor digiti minimi muscles.
Purchase azulfidine 500mg
As a generalization myofascial pain treatment center san francisco purchase azulfidine 500mg without prescription, abrupt events are vascular or electrical in origin, subacute symptoms are demyelinating or inflammatory, and symptoms that develop slowly suggest structural deficits or degeneration. The subsequent course of the symptoms also assists in identifying the underlying process: self-limiting events are often vascular; paroxysmal symptoms tend to be electrical or demyelinating, depending on their duration; and progressive syndromes are compressive or degenerative. The circumstances surrounding the development of the symptoms may be suggestive of a particular pathophysiology: trauma, preceding infection, drug exposure, or pregnancy alerts the observer to structural, demyelinating, toxic, and venous thrombotic mechanisms, respectively. The neurological examination Examination of the patient with neurological disease needs to be structured and organized without exhausting the patient and examiner through obsessive attention to irrelevant detail. Conclusions on likely localization from the history are essential to focus the examination to the most likely relevant areas. In fact, the neurological examination is often used to confirm or refute the diagnosis which has been formulated on the basis of the history. That said, it is best routinely to adopt a basic core examination and do things in order because the detection of one abnormality will determine the interpretation of another. It takes only a few minutes for the experienced and adequately equipped examiner to confirm that corrected visual acuity is normal in each eye, there is no gross field defect, and the optic fundi are normal. Movement of the lower face during forced eye closure, voluntary elevation of the palate, and rapid protrusion or side-to-side movement of the tongue take a few seconds to observe and effectively cover all the lower cranial nerves. It is rarely necessary to test the sense of smell or hearing, and a tuning fork is most useful for establishing that deafness is conductive and therefore probably not relevant. Before moving to the limbs, it is worth testing neck flexion in patients where the history suggests muscular or neuromuscular disease. It may be necessary to establish specific patterns of muscle weakness: global loss affecting the hand in cortical disease; selective involvement of extensor groups in upper motor neuron disease; the patterns of C5 to T1 nerve root lesions; diffuse distal weakness of both extremities in peripheral neuropathy; and the subtle distinctions between radial, median, and ulnar neuropathies, and C7, C8, and T1 root lesions, respectively. Detailed sensory examination of the arms rarely achieves more than can be learned from establishing that crude protective sense (recognition of a sharp pin) or discrimination (position sense and the ability to distinguish two points or perform a simple task such as manipulating a button) is intact. Although this may involve some rearrangement of clothing, it otherwise takes almost no time to swipe the abdominal reflexes in passing, before examining the legs. Here, the structured motor examination is as for the arms, although increased tone is more easily detected by lifting the relaxed leg from the couch at the thigh, and testing internal and external rotation at the hip. Characteristic patterns of weakness are the involvement of flexors at all joints and eversion at the ankle in upper motor neuron lesions, the usual diffuse symmetrical distal involvement in peripheral neuropathy at a time when the hands may be normal, and difficulty in distinguishing injury of the lateral popliteal nerve from an L5 to S1 root lesion (in which the ankle jerk is lost) in the context of unilateral foot-drop. Proximal weakness is best detected by watching the patient walk, and the calf muscles are normally so strong as to be untestable except with the patient standing. As in the arm, coordination can be assessed only once the degree of weakness has been established. Tendon reflexes in the legs may be brisk in isolation and often spread, so that, in an upper motor neuron lesion, when one is tapped several may respond-and in either leg. Sensory examination of the legs tends to be more reliable for protective than for discriminative sensation. In mapping a sensory level, it is best to move from the relatively anaesthetic to the normal zone, noting the band of hypersensitivity that usually exists at the boundary. It is a matter of fact that many patients confuse the examination by exaggeration or elaboration of physical signs; this most commonly affects power, with the usual clues being a mismatch between the ability to walk and findings on formal assessment of muscle strength (or vice versa), and simultaneous contraction of agonist and antagonist muscles. Sensory testing is subjective and so necessarily vulnerable to inaccurate reporting, but confirming that a sensory level is present both on the abdomen and back, and on the same side on each, with a slightly higher level on the trunk, is a simple manoeuvre that may yield surprising discrepancies in the patient with nonorganic deficits. The overall purpose of the history and examination is to assess where and through what mechanism structure and function have been affected. Detection of these patterns becomes routine for the experienced neurologist, but the process represents more than just a ritual of clinical neurology. Investigation of neurological disease the investigation of patients with neurological disease was revolutionized in the early 1970s with the introduction of computed tomography. Before then, only the most primitive structural details of the central nervous system could be detected by demonstrating indirectly the shape and placement of the ventricles and blood vessels, and usually at some discomfort to the patient. Function in the central nervous system and peripheral nervous system was measured using neurophysiological techniques. Investigation still does not replace clinical assessment but, as the chapters that follow make clear, it is now possible to detect structural changes in most parts of the brain and spinal cord at high resolution; to distinguish many pathological appearances at these sites on the basis of differences in the magnetic resonance signals; to map function within regions of interest using changes in blood flow and the use of metabolic substrates; to show variations in efferent and afferent electrical activity in the central nervous system and peripheral nervous system; and to detect an increasing range of soluble mediators of normal and pathological function in the cerebrospinal fluid. Taken together, these laboratory investigations still do no more than supplement clinical assessments and, in one sense, the high expectations of diagnosis make for additional difficulties in interpreting neurological illness when the images are normal, compared with the era when authoritative statements from neurologists could never be validated and necessarily went unchallenged. The value of many routine investigations lies in confirming normality and endorsing abnormalities already strongly suspected on clinical grounds. Given the increasing sensitivity of techniques for brain imaging, altered appearances that are not necessarily of pathological significance and genuine lesions that are not relevant in the particular clinical context need to be interpreted with common sense. Overall, the trend has been for the pendulum to swing from diagnosis without adequate laboratory evidence to diagnosis made in defiance of clinical intuition. Even when an imaging abnormality has been identified, its nature may require clinical discussion in order to resolve the most likely pathological substrate-the distinction between ischaemic and inflammatory tissue often proving difficult and not all neoplastic tissue being easily identified as such. The management of neurological disease the first issue that confronts the doctor looking after a person with neurological disease is when to discuss and name the diagnosis. Most wait until there is sufficient clinical or laboratory evidence to rule out misdiagnosis; telling people that they have a condition when they do not is bound to cause distress and has landed some specialists in the law courts. However, excessive caution and avoidance of discussion can be equally damaging, and there are many more patients who harbour bitterness over delay in learning the true nature of their illness than those who wish that they had not been told so soon, or at all. Most individuals cope extremely well even with the prospect of conditions that are known to be life-threatening or have a poor prognosis for disability. Advice may be needed on alterations in lifestyle resulting from neurological disease. There is a basic human need to know why a thing has happened and most patients enquire about causation but, naturally, the uppermost question is whether symptoms can be treated, or the natural history of disease usefully modified. Drug treatment may be used, on an intermittent or regular basis, to suppress symptoms; for example, intravenous methylprednisolone to reduce inflammation, anticonvulsants to suppress epilepsy, -aminobutyric acid agonists to deal with spasticity or anticholinesterases to enhance transmission at the neuromuscular junction. Pharmacological options also exist for interfering with the mechanism of disease, again on an intermittent or routine basis. In other situations, the rationale of treatment is to modify the underlying disease process; for example, by suppressing inflammatory processes in acute post-infectious polyneuritis using intravenous -globulin, treating patients with multiple sclerosis using -interferon, and using immunosuppressants such as methotrexate and cyclophosphamide in polymyositis and vasculitis, respectively. Many other illustrations could be given, confirming that the age-old witticism concerning the therapeutic nihilism of clinical neurology is at best now only of historical interest and was always generally rather ill-informed. Beyond the present pharmacological achievements in drug treatment lie many opportunities for improving handicap and disability through the use of rehabilitation, which increasingly assumes centre stage in the management of neurological disease through attention to the person with impairments in a particular social and cultural setting rather than focusing on the pathophysiology of disease in an individual void. For the future, there is the prospect of enhanced regeneration in the context of diseases affecting the central nervous system and peripheral nervous system, restoring structure and function, and thereby both limiting and repairing the damage. They have some practical importance, influencing the way that doctors approach patients and train students, and they underpin a deep theoretical problem in biology, the puzzling relationship between body and mind. A century of research on the biological basis of cognition, mood, personality, and behaviour, and much recent writing in philosophy, points to the need to rethink these time-honoured beliefs. But both everyday clinical experience and our growing understanding of the physical basis of mind challenge this view. Patients are always a compound of body and mind; discoveries relating to the mechanisms, phylogeny, ontogeny, and functions of the central nervous system are gradually traversing the mind-body and mind-brain divides. We should take a bio-psycho- social approach in every clinical encounter and seek theories that explain the emergence of mind from life much as life emerges from matter. We use it to refer, broadly, to the capacities that enable our cognition, mood, motivation, personality, and behaviour. Cognition is currently subclassified into attention, memory, executive function (the ability to organize thought and behaviour), language, perception, and praxis (our capacity for skilled action). Cognition is closely related to-but not identical with-the other aspects of mind: mood and motivation are self-explanatory; personality refers to the more or less enduring traits that characterize our conduct of our lives and our approach to other people; behaviour is included among the elements of mind to allow for instances-like temper tantrums-in which the outward manifestations of mental processes are their most striking feature. There is, for example, a powerful human tendency, apparent across cultures and historical time, to believe that the mind can be prised apart from the body and survive its death. Whatever our own attitudes to these beliefs, they continue to exert a widespread influence. Introduction Here is one view of the relationship between medicine and psychiatry: physicians study, diagnose, and treat disorders of the body. Medicine is concerned mainly with processes in objects- like the circulation of the kidney; psychiatrists concern themselves mainly with the experiences of subjects-like auditory hallucinations.
500mg azulfidine mastercard
When a patient blood sample is delivered to the blood bank and appropriate patient identification is performed lateral knee pain treatment generic azulfidine 500 mg online, the specimen is centrifuged and tests are performed on either serum or plasma. If an antibody is present in the serum/plasma, it will react with the screening cell(s) and cause red cell agglutination. If a pattern is detected, the specificity of the alloantibody can usually be identified. Blood bank tests are performed using the tube testing system in which red cell agglutination is identified in standard test tubes. These include gel systems based on the differential mobility of red cell agglutinates through gel columns and capture systems in which test red cells are immobilized on microtitre plates. Blood group systems Blood group antigens are proteins and carbohydrates attached to lipids or proteins. The codominantly expressed A and B genes, located on chromosome 9, code for glycosyltransferases that add either Nacetyl-d-galactosamine (A gene) or -d-galactose (B gene) to the common precursor H antigen (Table 22. Group O individuals lack functional transferases due to a single base deletion in the A gene that eliminates its production. Circulating A and B antibodies can fix complement and cause intravascular haemolysis. Accordingly, group A individuals produce anti-B, group B produce anti-A, and group O produce both anti-A and anti-B, as well as anti-A,B, an IgG antibody. It is worth noting that this anti-A,B antibody produced by group O individuals can cross the placenta and potentially lead to haemolytic disease of the newborn in non-group O neonates. Circulating A and B antibodies are of critical importance in blood therapy because they are responsible for most major haemolytic transfusion reactions. The five major antigens in the Rh system (D, C, c, E, and e) are responsible for most Rh-related transfusion incompatibility. Rh-null red cells are morphologically abnormal and typically have shortened survival, resulting in a mild haemolytic anaemia. The most clinically important Rh antigen is D because it is strongly immunogenic; the likelihood of a D-negative person developing anti-D following exposure to as little as 0. Anti-D is responsible for immune reactions including haemolytic disease of the newborn and immunemediated transfusion reactions. Despite widespread use of Rh immune globulin, anti-D remains a most common cause of serious haemolytic disease of the newborn. Rh-negative women most commonly produce anti-D after exposure to D-positive red cells during pregnancy, a miscarriage, or abortion. The anti-D formed is of the IgG class and therefore can cross the placenta where it may cause potentially fatal intrauterine haemolysis in an Rh-positive fetus. Antibodies to these blood group antigens may form following exposure to the corresponding antigens during transfusion or pregnancy and are associated with immune-mediated red cell destruction of transfused cells and haemolytic disease of the newborn (Table 22. In most cases, compatible blood can be found for patients with red cell alloantibodies. Based on the high incidence of some red cell antigens among specific donor populations, however, some patients may be difficult to transfuse if they have developed multiple antibodies. This is particularly true in patients with sickle cell disease and other red cell disorders who require frequent transfusions. The Kell system is linked to chronic granulomatous disease, a congenital disease in which a decreased oxidative capacity of neutrophils leads to recurrent, severe bacterial infections. The genetic defect seen in chronic granulomatous disease is located on the X chromosome near the Kx Kell locus, mutation at that locus results in depressed expression of the Kell antigens. Abnormalities described in this disease include acanthocytic red cells that are prone to mild haemolysis, cardiomyopathy, areflexia, and skeletal myopathies: this is known as the McLeod phenotype. The Duffy antigens, which occur at a much lower incidence among African populations, have an interesting association with malaria. The antibodies to the Kidd antigens are unusual in that once formed, they often fall below the level of detection and may not be detected in an already immunized patient. Some alloantibodies are naturally occurring and some are formed following exposure to transfusion or by pregnancy. Antibody significance is determined by their class and subclass, quantity, ability to activate Table 22. In this situation, transfusion of additional Kidd-positive red cells may cause a rapid, secondary immunological response, leading to formation of high-titre anti-Kidd with subsequent haemolysis and delayed transfusion reactions. A clinically significant alloantibody can cause a haemolytic transfusion reaction or haemolytic disease of the newborn. Autoantibodies Autoantibodies consist of immunoglobulins that react with a wide range of self-antigens including membrane and intracellular components, adsorbed plasma proteins, and nuclear antigens. However, patients with warm autoimmune haemolytic anaemia often require transfusion. Additional time may be required by the blood bank to exclude the presence of a significant underlying alloantibody that is obscured by the autoantibody. Upwards of 25% of previously transfused patients with warm autoimmune haemolytic anaemia may have an underlying alloantibody which can cause red cell haemolysis. Many hospitals will supply group O Rhnegative red cells until a patient sample is obtained and tested. In either case, compatibility testing is performed on these transfused units as soon as possible. It is critically important to realize that supplies of O-negative blood are limited and some centres adopted the strategy of transfusing males with O Rh D-positive units in an emergency situation and preserve the O Rh D-negative units for children and females. Although a true serological crossmatch is not performed, the computer crossmatch is safe in the vast majority of transfusions. Clinical use of blood components Blood component therapy refers to transfusing only the specific component that is required by a patient. Individual components are stored under optimal conditions, which maintain the integrity and potency of each respective blood component. The difference in storage requirements among blood components is one of the reasons why whole blood usage has dropped. Other reasons include the requirement to provide the best blood component for the patient, cost, manufacturing logistics at the blood centre, and Compatibility testing Routine compatibility testing is performed only on red cell units, whole blood, and granulocytes prior to transfusion. Plasma separated from whole blood can be further fractionated into coagulation factor concentrates, albumin, or gamma globulin. Red cell units, prepared from whole blood by removing most of the plasma, are indicated for patients with acute haemorrhage or chronic anaemias (Table 22. Earlier preservative solutions composed of citrate, dextrose, and phosphate buffers allowed storage of red cells from 21 to 35 days. Citrate contained in blood preservatives binds calcium to inhibit clotting and may cause hypocalcaemia and alkalosis in neonates and massively transfused patients. They are frozen with glycerol to avoid cell dehydration and damage during the freezing process. Younger patients will usually tolerate a given degree of hypoxaemia and hypotension better than older patients who may have underlying coronary or myocardial disease. Evidence of symptomatic anaemia includes excessive fatigue, malaise, headache, tachycardia, hypotension, and end-organ damage. Initially, the haematocrit will be falsely elevated in acute haemorrhage, but will then fall with fluid resuscitation. Transfusion is rarely indicated when the haemoglobin (Hb) level is greater than 100g/litre, and is often not considered until the Hb level is less than 70g/litre. Patients with unstable angina or acute myocardial infarction may require transfusion when the Hb level is less than 100g/litre. In the absence of active red cell destruction, transfusing a single unit will typically increase the Hb level by 10g/litre (haematocrit by 3%). Platelets Platelets are in most cases a by-product of red cell and plasma separation. The risk of bacterial growth and development of platelet function abnormalities (platelet storage defect) has precluded longer storage. Additionally, platelets can be collected and manufactured by apheresis resulting in single donor platelets.
