
Purchase cheap cyclophosphamide on line
Some species become dormant in tissues and cause prolonged treatment 2nd degree burn cheap cyclophosphamide 50mg fast delivery, asymptomatic infection. Its propagation depends on the presence of a reservoir of partially immune, asymptomatic human carriers. Because it is more virulent and more likely to be resistant to antimalarial drugs, Plasmodium falciparum must be distinguished from other plasmodia and treated promptly. Like malaria, babesiosis is a protozoal infection of erythrocytes, but it is more geographically localized and less prevalent, partly because it is transmitted by ticks rather than mosquitoes. Cats are the definitive (intestinal) host for Toxoplasma gondii; all other animals develop dormant toxoplasmic cysts in their muscles and viscera. Humans acquire infection by ingesting oocysts from cat feces or muscle cysts in undercooked meat. Virulence attributes of various Leishmania species determine whether infection results in a chronic skin ulcer at the site of the sand fly bite or a disseminated chronic febrile illness involving the liver, spleen, and lymph nodes. Long-standing infection with the agent of Chagas disease, Trypanosoma cruzi, may result in immunopathologic damage to the heart and the gastrointestinal tract. The agent of African sleeping sickness, Trypanosoma brucei, evades the host immune response by a genetically determined mechanism of antigenic variation. Protozoa that infect tissues can cause significant damage to the eyes, brain, or heart (toxoplasmosis); to the brain (African sleeping sickness); or to the heart and gastrointestinal tract (Chagas disease). It occurs in many tropical and semitropical regions of the world, with approximately 200 to 300 million cases annually (see Table 51-1). An estimated 2 to 3 million people die of malaria each year, especially malnourished African children. Infected humans are the only reservoir for these plasmodial species that infect humans; transmission occurs through the bite of infected female anopheline mosquitoes. However, a less common form of human malaria has recently been attributed to a monkey parasite, P. After 1 week in Nairobi, she embarked on a 10-day trip through the wildlife preserves of Serengeti and Ngorongoro, with a final visit to Mombasa on the Indian Ocean. She suddenly developed an intense chill that lasted for about 30 minutes, followed by a fever to 40. Her symptoms continued to worsen, and she was brought to the hospital unconscious 2 days later. She showed no signs of endocarditis, and a lumbar puncture was negative for bacterial meningitis. The attending physician, drawing on his experience while serving in the armed services abroad, recognized that Ms. The recent history of travel to endemic areas gave credence to his suspicion of the disease, and the diagnosis was confirmed when a Giemsa-stained smear of Ms. The parasites were identified as Plasmodium falciparum by their characteristic ring shape. Hypoglycemia can result both from consumption of glucose by large numbers of parasites and from the direct release of insulin from the pancreas caused by quinidine or quinine. She was given multiple transfusions for her anemia and was put on a dialysis machine because of her kidney failure. She recovered and was discharged after spending 10 days in the intensive care unit. Most cases of malaria that occur in Europe and North America are acquired in endemic areas and then imported into the nonendemic areas during the incubation period (imported malaria). However, mosquitoes that can serve as vectors (Anopheles) exist in the United States. Although malaria can no longer take hold in temperate, industrialized countries like the United States, in rare cases, persons who have never traveled abroad have contracted the disease. It is assumed that such cases occur when potential vector mosquitoes feed on blood from a malaria carrier. Introductions of malaria have occurred when a large number of infected soldiers have returned from war and when a region has received a large number of immigrants at one time. Malaria also can be transmitted by blood transfusion or by the sharing of needles among intravenous drug users (induced malaria). In the infected mosquito, plasmodia inhabit the salivary glands as sporozoites, a stage of the parasite that is infectious for humans. Sporozoites are injected into the human bloodstream when infected mosquitoes bite and feed. These organisms travel through the bloodstream and enter liver cells within 30 minutes of injection. Over the next 8 to 14 days, the parasites multiply and mature inside liver cells to very large numbers. At the end of that period (the hepatocellular cycle), they are released once again into the bloodstream in a form that can invade red blood cells (merozoites). After 2 or 3 days, the cells burst, liberating a new generation of infective merozoites that infect previously unparasitized red blood cells (the erythrocytic cycle). A minority of the merozoites in the blood develop into forms capable of sexual reproduction, called gametocytes. In the mosquito gut, the haploid male and female gametes fuse to form a diploid zygote. After the zygote is formed, the parasite undergoes further changes in the mosquito gut and then divides by meiosis to generate sporozoites. Sporozoites migrate to the salivary glands and once again become infective for humans. All the subsequent asexual stages in the human, up to and including the gametes, are haploid. In each of those stages, the plasmodial cells are morphologically distinguishable. Thus, infection with either species can cause a series of relapses to occur months or even years after the initial episode. Recurrent malaria is prevented by treatment with an antimalarial agent that targets the latent parasites (hypnozoites) within liver cells. The spleen recognizes and removes older and less deformable red blood cells from the circulation, thus removing parasitized red blood cells from the circulation. Not surprisingly, malaria may cause enlargement of the spleen (splenomegaly), and splenectomized people have higher degrees of parasitemia and more-severe infections. When multiple parasitized red blood cells adhere and accumulate on the endothelium, blood flow through the deep vascular beds is impeded. However, the obstruction of blood flow in the microcirculation may have dire pathological consequences for the host. However, some parasites remain dormant in the liver as hypnozoites (see the dashed lines from stages 1 to 3). When gametocytes are taken up by a female Anopheles mosquito, the male gametocyte loses its flagellum, producing male gametes. Mature oocysts produce sporozoites, which migrate to the salivary gland of the mosquito (1) and repeat the cycle. The dashed line between stages 12 and 13 indicates that absence of the mosquito vector precludes natural transmission through this cycle. Note that infection by the injection of infected blood bypasses that constraint and permits transmission of malaria among intravenous drug addicts and to persons who receive blood transfusions from infected donors. The surge in those cytokines is the stimulus for the sudden chill and fever characteristic of a malaria paroxysm. Parasite replication can become synchronized so that all infected red blood cells lyse at the same time. As a result, a regular, periodic fever pattern may develop, depending on the length of the intracellular replication cycle: every 2 days with P. Other frequent clinical presentations include a syndrome similar to influenza (fever, muscle aches, and malaise) and gastroenteritis of different ages: P. For example, parasite invasion of red blood cells depends on the presence of specific surface molecules. Many epidemiological studies have shown that sickle cell disease-a recessive genetic disorder that causes red blood cells to become rigid and elongated when oxygen tension is reduced-is common in areas of Africa with a high incidence of P. A defective form of hemoglobin, called sickle cell hemoglobin (HbS), causes the disease.
Cheap cyclophosphamide 50mg fast delivery
Because of their effects on pRb and p53 medicine look up drugs order cyclophosphamide with a mastercard, adenoviruses possess oncogenic potential. Indeed, the cellular proteins are known as tumor suppressors, since mutations in their respective genes are associated with a wide range of nonviral human cancers. Adenoviruses are not alone in their effects on tumor suppressors: Papillomaviruses, polyomaviruses, and some herpesviruses encode proteins that subvert the functions of pRb and p53, resulting in the induction of tumors. Released virus can attach directly to adjacent cells or spread to cells in remote locations through the bloodstream. Systemic symptoms such as chills, headache, muscle aches, and fever are common, and conjunctivitis sometimes accompanies the other symptoms (pharyngoconjunctival fever). Different serotypes are associated with different disease manifestations (Table 39-1). Serotypes 1, 2, 5, and 6 are endemic in most populations, and 80% of all young adults have neutralizing antibodies to those types. Adenoviruses are also an important cause of acute gastrointestinal disease in children and may be responsible for up to 15% of childhood intestinal infections. Many serotypes of adenoviruses are present, not only in the stool of patients but in normal stool as well, in contrast to other serotypes that are only associated with disease. Adenovirus type 12 (Ad12) has been implicated in the development of celiac disease (gluten enteropathy). The development of that illness appears to depend on protein sequence homology between an Ad12 early protein and gliadin-, a component of the cereal grains that activate the disease. It is possible that exposure to Ad12 induces an antibody response to gliadin-, which predisposes to celiac disease in some persons. Less common than respiratory and gastrointestinal disease is adenovirus-induced conjunctivitis without other symptoms. Mild "swimming pool conjunctivitis" 408 Part 2: Infectious Agents is probably most often a result of adenovirus infection, as is the more serious, highly contagious epidemic keratoconjunctivitis. Latent adenovirus infections are very common; adenoviruses can be recovered from as many as 80% of the tonsils or adenoids removed from children and young adults. In fact, the majority of healthy adults examined have very small numbers of peripheral lymphocytes apparently undergoing a typical adenovirus lytic cycle. Early gene products that interfere with host defense mechanisms may play a role in persistence. Disseminated adenovirus infections also are a significant cause of mortality among stem cell transplant recipients. In these cases, reactivation of latent adenovirus infection is probably the source of the acute infection. Interactions with Host Defense Systems Adenoviruses carry several genes that function to evade or antagonize antiviral host defenses. In cotton rats, infections of the lung with adenovirus mutants that do not express the E3 protein induce a striking pulmonary infiltration of neutrophils, suggesting that this protein influences the course of disease in vivo. Another way in which adenoviruses escape cellular immunity is through resistance to signals from immune cells that would otherwise cause premature death of the infected cell. Adenoviruses produce proteins that block these death pathways and render cells relatively resistant to either death stimulus. In addition, adenovirus mediates the removal of a cell-surface receptor required for killing by Fas ligand. A third line of defense against viral infection is the antiviral state induced in cells by interferon-a and interferon-b. Among other effects, the interferons prevent protein synthesis in virus-infected cells by initiating a chain of events that culminates in the inactivation of the cellular translation machinery. Obviously, adenoviruses do not completely blunt antiviral responses, because most adenovirus infections eventually are cleared. However, it is likely that reductions or delays in these processes contribute to the success of adenoviruses as common human pathogens. Those studies have contributed significantly to knowledge about the molecular basis of carcinogenesis. While playing no apparent role in human cancer, adenoviruses induce phenotypic changes in cultured cells that resemble those that occur during natural carcinogenesis. Transformation by adenoviruses requires the products of the E1A and E1B regions, which transform cells largely by interacting with the cellular tumor suppressor products pRb and p53 (see the Paradigm Box). Importantly, transformation by adenoviruses is only an incidental consequence of the mechanisms that regulate viral gene expression. This property has been exploited to introduce nonviral genes into animals or animal cells. Because much is known about adenovirus biology and genetics, adenoviruses are considered to be particularly promising vectors for foreign gene delivery. Such genetically engineered adenoviruses direct the production of the foreign antigen in infected cells. A second potential application for adenovirus is as a vector for the introduction of an exogenous gene into an individual for therapeutic purposes. Gene therapy is usually envisioned as a therapeutic approach for an inherited disease. Significant technical problems, such as short-lived expression of the exogenous genes, need to be overcome before gene therapy of this sort becomes practical. The tragic death of a human volunteer in an adenovirus gene therapy trial in 1999 points out the social and ethical problems that also accompany the development of gene therapy. Numerous clinical trials with recombinant adenoviruses designed specifically to kill cancer cells are under way. Cell death is variously accomplished by delivery of toxic genes, by delivery of genes that stimulate antitumor immunity, or by use of adenovirus mutants that grow selectively in cells with genetic abnormalities frequently found in cancer cells. As with adenovirus vaccination and gene therapy, much work remains before adenovirus anticancer therapy becomes clinically useful. As many as 80% of some groups of recruits are affected, with one-fourth to one-half requiring hospitalization in some outbreaks. Vaccine manufacture is now being reestablished, and it is likely that the disease will again come under control. Largely because of the risk of severe adenovirus disease in transplant recipients, significant efforts have been made to identify antiadenovirus drugs. Several established and developmental antiviral drugs show efficacy against adenovirus in tissue culture, but none has yet shown sufficient promise in animals to justify use in humans. The eye, the upper and lower respiratory tracts, and the gastrointestinal tract are often involved. Adenoviruses are capable of cellular transformation and oncogenesis in animals, but convincing evidence linking adenoviruses to cancer in humans is lacking. The expression of adenovirus genes follows a defined program, some genes being expressed early, while others are expressed late. Modified adenoviruses may be suitable candidates for recombinant vaccines to be used in immunizing against a variety of antigens or for introducing genes into humans for correction of genetic diseases. Recent lessons in gene expression, cell cycle control, and cell biology from adenovirus. Treatment and Prevention: Treatment includes chemical, surgical, and physical modalities that destroy infected tissue. Clinical manifestations of warts range from inapparent (subclinical) to large bulky growths. The majority of patients with warts seek medical attention because of physical discomfort or concern about the appearance of a new skin lesion. While most papillomavirus-induced warts are biologically benign, some warts may become cancers. Particles of these viruses are formed by two tightly packed viral proteins called L1 and L2 and contain a single copy of the circular viral genome. Because the viruses do not bud from infected cells, they do not have a lipid envelope. Therefore, these viruses remain infectious in the environment for long periods of time.
Buy generic cyclophosphamide line
Therefore medications xyzal buy cyclophosphamide 50mg otc, infection originating in medullary bone can easily spread and rupture through the thin cortex into the subperiosteal space. Subperiosteal abscesses are common in this age group and lead to a stimulation of periosteal bone formation at an inappropriate site, as periosteal cells transform into osteoblasts. The new bone formation is disorganized and produces a weakened bone called an involucrum. Osteomyelitis in an infant can be a devastating disease because early in life the capillaries of the metaphysis extend into the epiphyseal growth plate. Consequently, osteomyelitis in an infant can be a destructive process resulting in permanent deformity of bone and abnormalities of growth. Children In children between the age of 1 year and puberty, bone infection also occurs most frequently in long bones but is generally contained within the metaphysis. This pathophysiology is likely attributable to the thicker cortex and lack of transphyseal blood vessels in children of this age in contrast to infants. The periosteum also adheres more tightly to the cortex in this age group; thus, rupture of infection into the subperiosteal space and formation of involucrum is less likely. However, within the bone itself, pressure can increase and cause occlusion of arterioles and clot formation in the capillaries. The end result is often necrosis of bone, and in advanced cases, a sequestrum can form. Tissue in a sequestrum is no longer in contact with the vasculature and acts essentially as a foreign body in which organisms can proliferate out of reach of both host defenses and antibiotics. Ultimately, the sequestrum must be resorbed (by the body) or removed surgically if the infection is to be cured. As children age, this complication is even more likely because the bone is more calcified and the periosteum even more tightly attached to bone. Fracture Involucrum Adults Hematogenous osteomyelitis seen in adults most frequently involves the vertebral bodies. The reason for that predilection is uncertain but may stem from degenerative bony changes and vascular proliferation in the disk space between the vertebrae, which normally occur with age. The infection usually begins in the disk space and then spreads to the contiguous vertebrae. Involucrum secondary to extensive periosteal reaction and fracture caused by weakened infected bone. Infection of vertebrae can also result from drainage of infected pelvic organs through pelvic veins into the complex, interconnected venous networks surrounding the spinal column known as Batson plexus. Because the possible causes of vertebral osteomyelitis are numerous, it is imperative to obtain material from the infected area for culture (unless blood cultures rapidly yield causal organisms). Vertebral osteomyelitis usually responds to medical therapy alone, but the neurologic status of the patient must be monitored closely because infection can spread from the vertebral body into the subdural or subarachnoid space through the rich venous and arterial plexus of the paravertebral circulation. The development of sensory or motor changes requires urgent surgical drainage to prevent irreversible neurologic damage. Radiograph showing changes in more advanced osteomyelitis with extensive bone lesions. Osteomyelitis Secondary to Contiguous Foci of Infection Bone infection can result from the direct introduction of microorganisms from an external source or spread from a contiguous source. An additional common setting for contiguous bone infection is following insertion of orthopedic hardware, such as a joint prosthesis or bone fixation device. These infections are difficult to eradicate because the bone has been traumatized (reducing the effectiveness of host defenses), and the foreign body acts as an avascular sanctuary for the persistence of bacteria. Bacteria, especially staphylococci, can grow and reside in biofilms on the surface of foreign bodies and are thus sheltered from antibiotics. In the face of active infection, deciding whether to remove a fixation device or joint prosthesis to facilitate cure is often difficult and emotionally traumatic. On one hand, such a device may be necessary to achieve bony union or to allow ambulation or proper joint function; on the other hand, its presence may prevent cure of the infection. In some infections involving orthopedic prostheses, the devices can be salvaged, especially if the infection is caught early, the organism is exquisitely susceptible to antibiotics (as are streptococci), and there has not been loosening of the prosthesis. Treatment decisions require close interactions between surgeons and infectious diseases specialists to determine if and when removal is necessary and in the best overall interest of the patient. Frequent complications of vertebral osteomyelitis are spinal epidural abscess, which, if not treated appropriately, can cause irreversible loss of neurologic function, and psoas abscess, which often requires surgical drainage for cure. X-ray of the lumbar vertebrae showing destruction of bone associated with staphylococcal osteomyelitis. It is especially important to determine the bacterial etiology of the infections because of the frequent involvement of inherently resistant organisms such as enterococci and P. Results of surface cultures correlate poorly with those taken from bone and deep tissue and should not be used to guide therapy. In the absence of definitive culture results from bone or deep tissues, antibiotics must target a wide range of Gram-positive and Gram-negative bacteria, including anaerobic bacteria. Unfortunately, amputation is frequently the result of what may have started out as a trivial soft tissue infection of the foot, in spite of appropriate surgical and medical management. Chronic Osteomyelitis A serious complication of inadequately treated acute osteomyelitis is chronic osteomyelitis. Chronic osteomyelitis can remain dormant, and affected patients can be asymptomatic for years or even decades. Exacerbations are often associated with purulent drainage from a fistulous tract to the skin and may be accompanied by worsening pain, fever, and elevations in C-reactive protein and erythrocyte sedimentation rate. Antibiotic therapy often results in resolution of such episodes, and patients generally feel entirely well between them. The identity of the pathogen often reflects the circumstances of the trauma and the part of the body involved. Contamination of a wound by dirt or water often leads to infection with Gram-negative bacteria, including P. A wound may become contaminated with bacteria that are constituents of fecal flora, particularly in an incontinent patient with a hip fracture. Coagulasenegative staphylococci are more likely to cause infections in the presence of a prosthesis. In evaluating a patient presenting with arthritis, the physician must make three determinations. First, the physician must decide whether the joint inflammation is the result of infection. Noninfectious inflammatory joint disease can be caused by gout, pseudogout, rheumatoid arthritis or other connective tissue diseases, or viral infection, and these entities may be difficult to distinguish clinically from a bacterial process. Second, if infection appears likely, the physician must determine the pathophysiology of the infectious process. As with osteomyelitis, a joint can be seeded during the course of bacteremia from another primary focus, bacteria can be introduced directly into the joint by trauma or a surgical procedure, or bacteria can extend into the joint space from adjacent bone. Usually, all three determinations can be made by obtaining a complete history, performing a careful physical examination, and analyzing fluid obtained by aspiration of the joint. Osteomyelitis in Persons with Diabetes A special category of osteomyelitis occurs in persons with diabetes as a consequence of the large vessel and microvascular disease and neuropathy that frequently complicate this condition. Skin and soft tissue ulcerations on the feet may go unnoticed because of sensory neuropathy, persist because of impaired host defenses, and ultimately penetrate into bone. Bone infections in diabetic patients are especially difficult to treat owing to the poor vascular supply to 668 Part 3: Pathophysiology of Infectious Diseases the diagnosis of infection is supported by the finding of numerous white blood cells, predominantly neutrophils, in joint fluid, a positive Gram stain or culture of the fluid, and an absence of other potential causes for inflammation, such as crystals. Synovial fluid consists of water, electrolytes, and other low molecular weight substances filtered from plasma, as well as components synthesized and secreted by synovial cells. Serum proteins are present in normal synovial fluid but in lower concentrations than in plasma. The inflammatory reaction in synovial fluid is caused by the interaction of serum proteins, phagocytic host cells, and microorganisms. The diagnosis of one type of joint disease does not preclude the presence of a second.
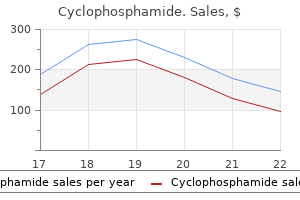
| Comparative prices of Cyclophosphamide | ||
| # | Retailer | Average price |
| 1 | HSN | 195 |
| 2 | OfficeMax | 984 |
| 3 | Wegman's Food Markets | 205 |
| 4 | Giant Eagle | 837 |
| 5 | Albertsons | 920 |
| 6 | Nordstrom | 747 |
Buy generic cyclophosphamide pills
Leishmania Species Leishmania species produce a spectrum of clinical syndromes symptoms indigestion purchase cyclophosphamide american express, from superficial ulcers to severe lesions of the liver, spleen, and bone marrow accompanied by systemic signs such as fever, weight loss, and anemia. The reason for the wide diversity in clinical disease is not well understood, but it is probably owing in part to the temperature preferences of the various species. Most previously healthy persons do not need treatment for self-limited, acute toxoplasmosis. A smear taken from the edge of the lesion stained with Giemsa revealed Leishmania-containing macrophages. The protozoa are transmitted by the bite of sand flies-small, short-lived insects that feed on many mammals. The phlebotomine sand flies that transmit leishmaniasis are generally found in tropical or subtropical parts of the world, which explains why the disease is rare in North America and Europe. However, phlebotomine sand flies are occasionally found in more temperate regions, and indigenous cases have been reported in the United States. Like malaria, leishmaniasis in the United States is seen mainly among travelers returning from tropical countries and has been observed in military personnel who participated in the 1991 Gulf War. Reservoirs of Leishmania parasites include rodents, dogs, other animals, and infected humans. The diseases they cause include localized skin ulcers, mucocutaneous lesions (espundia), disseminated cutaneous leishmaniasis, and disseminated visceral leishmaniasis (kala azar). Leishmania species also produce superoxide dismutase, which protects them from superoxide produced by the macrophages. After they are taken up into phagosomes, the parasites differentiate into a nonflagellate form, called the amastigote. Although the parasite-containing phagosomes fuse with lysosomes, the amastigotes are resistant to killing by lysosomal enzymes. The flagellated (promastigote) insect form of the parasite (1) is injected under the skin by the sand fly (Phlebotomus) vector (2). Once within the human host, the parasite transforms into a nonflagellated (amastigote) form that is more capable of evading the host immune response than the promastigote form (it stimulates less release of H2O2 from mononuclear cells than the promastigote and produces its own superoxide dismutase). The parasite then invades lymphoreticular cells (3), replicates (4), lyses the cells (5), and repeats the same sequence in other reticuloendothelial cells (6). In endemic areas, the cycle is completed when previously uninfected sand flies acquire infectious leishmanial amastigotes by biting infected humans (7). The amastigotes then transform into flagellated promastigotes (8) and replicate in the gastrointestinal tract of the sand fly (9). The dashed line between stages 6 and 7 indicates that transmission is blocked at this point in nonendemic areas such as the United States because the sand fly vector is not present. Chapter 52: Blood and Tissue Protozoa 517 depend on the low pH of the phagolysosomes for the uptake of nutrients such as glucose and proline. Immunity against leishmaniasis involves cell-mediated mechanisms and the induction of interferon- (a Th1 response; see Chapter 7). It is thought that the parasite may facilitate its own survival by possessing immunodominant antigens that preferentially induce a Th2 response, which is not protective. Leishmaniasis is best diagnosed by histologic examination of biopsy material using the high-dry objective. However, the various species look alike and cannot be distinguished morphologically. Leishmania species can be distinguished by culturing them in special media and then analyzing patterns of isoenzymes. A variety of drugs are used to treat leishmaniasis, especially the invasive forms of the disease. However, disease of deep organs, such as the bone marrow, may produce fatal anemia and granulocytopenia, despite treatment. Some forms of cutaneous leishmaniasis can be treated with allopurinol or ketoconazole. Overt disease is much less common than infection, but the reasons for the difference are poorly understood. In the endemic areas of South and Central America, most persons are infected by T. The reduviid bug vector deposits feces containing infectious trypomastigotes on the skin (1). The human host rubs the itching bite wound, allowing the parasites to enter the bloodstream. In the human host, the trypomastigote transforms into an amastigote (analogous to the leishmanial amastigote) as it invades tissue such as muscle (2). Cells containing large numbers of amastigotes often rupture, liberating large numbers of trypomastigotes (3). Trypomastigotes invade other host cells (arrow from 3 back to 2) or may be taken up by the vector to complete the cycle (4). In the vector, the parasite replicates as an epimastigote (5) and produces additional infectious trypomastigotes (6). The dashed line below stage 4 indicates that natural transmission does not occur in areas lacking the reduviid bug vector. Although reduviid bugs are present in the southern United States, indigenous cases are rare. Although some persons develop serious (even fatal) illness, most develop a relatively mild disease with fever, recover spontaneously, and remain asymptomatic. Radiologic examination of his gastrointestinal tract revealed a large, dilated colon (megacolon) and a somewhat less-dilated esophagus (megaesophagus). Infected reduviid bugs are present in the southern United States and are presumably responsible for the sporadic cases of Chagas disease observed among lifelong residents of Florida, Louisiana, Mississippi, and California. Consequently, several investigators have postulated that autoimmune mechanisms may play a significant role in the pathogenesis of those complications. Organisms often are found in the blood if it is cultured in an appropriate medium. Early infection can also be diagnosed by detecting infection in reduviid bugs that have purposely been allowed to feed on the patient. The diagnosis of chronic infection with complications is based on a positive antibody titer or history of exposure plus a known complication. Patients with early acute Chagas disease may respond to treatment with either nifurtimox or benznidazole. However, no effective treatment is available for patients with late complications, perhaps because the critical damage has already occurred and is no longer reversible. The disease is endemic in Africa and transmitted by the bite of infected tsetse flies. The tsetse fly vector inoculates infectious trypomastigotes under the skin (1) when it bites humans or other mammals. Once inside the new host (2), the parasite replicates in the bloo dstream by binary fission as a trypomastigote (3). Unlike Leishmania species and the trypanosome that causes Chagas disease, the trypanosomes that cause African sleeping sickness do not have promastigote or amastigote forms. The rate of movement of trypomastigotes from the bloodstream and lymph nodes to the central nervous system defines the point at which the illness changes from a systemic (hemolymphatic) infection to an encephalitis. Within the tsetse fly, the parasites replicate in the gastrointestinal tract and transform into epimastigotes (5). The dashed line below stage 4 indicates that natural transmission does not occur in countries such as the United States where the tsetse fly vector is not present. Two weeks ago, he developed a severe headache, stiff neck, and an aversion to light (photophobia). Trypanosomes were seen on Giemsa-stained specimens of blood and cerebrospinal fluid under the oil immersion objective. In East Africa the main reservoirs are wild game animals (such as impalas); West African reservoirs are infected humans and domestic animals, such as cattle. Several weeks to months after the initial infection, a patient develops a systemic illness with fever and swollen lymph nodes, and trypanosomes are present in the bloodstream. After several months (in the East African form) or years (in the West African form), the parasites invade the central nervous system and infect the brain and spinal fluid. During months or years of chronic bloodstream infection, patients undergo bouts of parasitemia.
Order cyclophosphamide 50mg line
For example treatment refractory 50mg cyclophosphamide free shipping, patients with tuberculosis, histoplasmosis, or lung abscesses sometimes experience acute, rapidly progressing disease. Physicians must also be aware that immunocompromised patients are at risk for a more severe and fulminant presentation of both acute and subacute pneumonias. Additionally, they may be susceptible to opportunistic pathogens, those which usually do not cause disease in immunocompetent individuals. On examination, her respiratory rate was elevated at 22 breaths per minute and her pulse oximetry was normal at 96%. A chest radiograph showed an infiltrate in her left lower lobe consistent with pneumonia. Over the next several days, her fevers resolved, and within 2 weeks, her symptoms had disappeared. Sometimes the patient complains of chest pain, frequently pleuritic (exacerbated by respiratory motion). Patients with extensive involvement of the lungs may have shortness of breath, rapid respiration, and cyanosis (bluish tinge to the skin indicative of hypoxemia). Auscultation may reveal crackles (also called rales) and peripherally auscultated bronchial breath sounds, which are usually indicative of alveolar disease. Traditionally, organisms have been divided into two groups, typical and atypical, based on the belief that the clinical and radiographic features of presentation suggest certain etiologic agents. A typical presentation is characterized by high fever, shaking chills, chest pain, and lobar consolidation on chest x-ray. Although studies have shown that it is very difficult to predict an etiologic agent based on presentation, the classification of organisms as typical and atypical persists. Although considerable overlap exists in the clinical manifestations of pneumonia, certain pathogens tend to be associated with characteristic presentations or to affect certain patient populations. Nursing home residents, immunocompromised patients, and people with underlying structural lung disease are at higher risk for pneumonia due to Pseudomonas aeruginosa, Gram-negative enteric bacteria (derived from the gut), and S. Several pneumonias result from agents found in animals or in the environment (Table 62-4). For example, Chlamydia psittaci, a common cause of disease in birds, can lead to psittacosis (parrot fever) in humans and may be acquired by inhalation (see Chapter 27). This illness is difficult to diagnose unless the physician obtains the history of contact with birds. Another example is Q fever, caused by the rickettsia Coxiella burnetii and usually acquired from sheep, goats, or cattle. The organism is stable in the environment, and infection can occur after exposure to contaminated material from infected animals. As with psittacosis, diagnosis of Q fever is difficult unless the physician elicits the history of exposure to animals or their environment. The clinical course is usually milder, with spontaneous recovery, although rarely, some viral pneumonias can lead to severe respiratory disease. Severe acute respiratory syndrome virus and influenza have been associated with acute respiratory distress syndrome. Additionally, bacterial 636 Part 3: Pathophysiology of Infectious Diseases superinfection can occur with viral pneumonia (especially influenza), causing a more severe clinical picture. In children under 2 years of age, the agents of acute pneumonias are more often viruses than bacteria. The most important diagnostic finding is a chest radiograph that reveals a shadow, or infiltrate. The radiographic pattern may suggest particular pathogens, although this is not definitive. Skilled interpretation is important because other processes, tumors, pulmonary edema, or pulmonary hemorrhage can produce radiographic changes very similar to those of pneumonia. Several prediction rules have been proposed to identify patients at increased risk of a complicated course. These are generally based on identifying host factors associated with more virulent organisms or an impaired response to infection. A patient with relatively mild illness managed outside the hospital usually does not undergo sputum Gram stain and culture tests, whereas these tests are performed for patients admitted to hospitals. In addition, in about half of cases of pneumonia, a microbiologic cause is not identified. Opinionbased recommendations by multispecialty experts have been published to provide guidance for empiric antimicrobial therapy based on clinical scenarios and host factors (Table 62-5). It is the leading cause of death from hospital-acquired infections, with an estimated mortality of 20 to 50%. Physical exam may reveal fever, tachycardia (elevated heart rate), and tachypnea (elevated respiratory rate). Signs of consolidation on physical exam include crackles and bronchial breath sounds. Microaspiration of bacteria from the oropharynx is considered the most common route of infection. Factors influencing the risk of pneumonia are the types of bacteria colonizing the pharynx and prior exposure to antibiotics. The oropharynx of hospitalized patients can become colonized with Gram-negative bacteria within several days of admission. Furthermore, illness and medications can disrupt the gastric pH, leading to colonization of the stomach with bacteria. Patients with advanced age; poor nutrition; history of smoking, alcoholism, or intravenous drug use; or other underlying chronic illnesses are also at increased risk for developing nosocomial pneumonia. In patients requiring mechanical ventilation, the endotracheal tube can provide a conduit from the outside environment to the lower airway by circumventing the defenses of the upper airway and allowing direct passage of oropharyngeal secretions, gastric contents, and associated bacteria down the course of the tube itself into the lower respiratory tract. In patients who have more severe infections, who have been exposed to broad-spectrum antimicrobial agents, or have had more prolonged hospitalizations, P. Fever, elevated white blood cell count, and purulent sputum are suggestive but not definitive. Chest radiograph showing a new infiltrate is sensitive but not specific because other conditions. Update of practice guidelines for the management of community-acquired pneumonia in immunocompetent adults. Some patients cannot produce sputum, or they produce sputum contaminated by oropharyngeal contamination. The presence of squamous epithelial cells in large numbers indicates contamination by oropharyngeal contents, and a culture of such a specimen can yield misleading information. Finding a predominant organism in the Gram stain may point toward the etiological agent; however, if an organism is cultured, it can be difficult to differentiate a colonizing organism from one causing active disease. Bronchoscopic sampling of the lower airways by bronchoalveolar lavage may be more helpful in establishing an etiologic agent but is an invasive procedure generally reserved for immunocompromised patients, individuals with severe disease, and those with illness not resolving with standard therapy. The procedure went well, but on postoperative day 3, he was noted to have a fever of 38. With appropriate therapy, many patients display improvement 48 to 72 hours after treatment is initiated. However, many patients with severe infections may develop complications and require mechanical ventilation, sometimes for prolonged periods. Patients with pleural effusion associated with pneumonia (parapneumonic effusion) should have the fluid evaluated for evidence of infection of the pleural space. Subacute Pneumonias A common cause of subacute pneumonia is the lung abscess, often a consequence of gross aspiration of oropharyngeal or gastric contents. The typical lung abscess represents a polymicrobial infection with multiple species of bacteria. The bacteria most commonly involved are anaerobes and microaerophilic organisms from the normal flora of the mouth. Lung abscesses can also result from infection with other organisms that destroy lung tissue, including S. The clinical course tends to be less acute than that of most other forms of bacterial pneumonia.
Discount cyclophosphamide 50mg fast delivery
When given for 5 days before viral infection 911 treatment for hair purchase cyclophosphamide online from canada, interferon was 80% effective in preventing illness. However, when given for longer than 5 days, interferon led to nasal symptoms as bothersome as those of a cold. Interferon treatment of rhinovirus infection is no longer being pursued because it is not effective in clearing an established viral infection. Antiviral drugs that inhibit various stages of the viral life cycle have been developed. Although some of the compounds have proven safe and effective in clinical trials, their effectiveness is reduced by the emergence of resistant viral strains. Further compromising the effectiveness of antiviral drugs is the short duration of virus shedding and illness. Studies of human coronaviruses in the 1960s and 1970s confirmed the capacity of these viruses to cause up to 30% of common colds. However, the limited frequency of severe human disease and the difficulty in growing human respiratory coronaviruses from clinical specimens were obstacles to identifying coronaviruses and understanding their potential to cause human illness. Research studies using animal coronaviruses have demonstrated that coronaviruses can undergo rapid genetic change with alterations in clinical disease and "trans-species" movement to new animal hosts. Recent studies of coronavirus genomics and evolution give important clues to the answers to those and other questions. Advances in understanding the molecular biology of coronaviruses have defined several biological characteristics that may influence the capacity of these viruses to move from one species to another. The coronavirus polymerase has a high intrinsic error rate with the potential to introduce multiple nucleotide changes during each genome replication. Although readily communicable, only rarely do Chapter 32: Picornaviruses and Coronaviruses 347 they cause severe disease. Illnesses caused by enteroviruses may be highly tissue specific (poliovirus) or can affect many organs (coxsackievirus and echovirus). These diseases are often difficult to distinguish clinically, and their presumptive diagnoses are often based on epidemiological features. The success in eradicating poliovirus with vaccination is providential because no other way is known to control the disease. Although it is a benign illness, associated complications such as asthma and lower respiratory tract infection can be life threatening. Furthermore, newly discovered members of the rhinovirus C species are now known to cause severe, life-threatening lower respiratory tract infections. It is therefore essential to develop effective means of controlling rhinovirus infections. Because conventional vaccine approaches do not appear feasible, current efforts are directed toward identifying novel approaches to immunization and effective antiviral compounds against rhinoviruses. Enteroviruses: polioviruses, coxsackieviruses, echoviruses, and newer enteroviruses. Encounter: Arthropodborne viruses are maintained in natural cycles between insects and birds, wild animals, or humans. Spread and Replication: Replication occurs in both invertebrate and vertebrate hosts. Damage: Infection may cause fever, encephalitis, rash, arthritis, or hemorrhagic fever. Diagnosis: Disease is usually diagnosed by serology or reverse transcription-polymerase chain reaction. Treatment and Prevention: these infections cannot currently be treated, but vaccines exist for a few and are under development for others. These viruses belong to several different virus families, the most important of which are the Togaviridae, Flaviviridae, and Bunyaviridae. Human infection is often asymptomatic, but when disease occurs, it can be manifested by mild to severe febrile illness, rash, arthritis, meningitis, encephalitis, or hemorrhagic fever. Each virus causes a characteristic spectrum of illness, but the same virus can produce diseases of differing severity depending on the viral inoculum and host factors such as age, genetic background, and immunological status. After an infected insect bites a human or reservoir host, the virus replicates locally, enters the blood, and then spreads to target cells and organs, such as the brain, liver, skin, or endothelium. Virus in the blood provides the means for infection of new susceptible insects that feed on the infected individual during that time. This transmission increases the number of infected mosquitoes, ticks, or flies and amplifies the infection in nature. The amount of virus in the blood determines the likelihood of the insect becoming infected during feeding. For many arboviruses, humans are "dead-end" hosts because the viremia is of short duration and levels of virus in blood are low. However, for yellow fever and dengue viruses, and occasionally for Chikungunya and Ross River viruses, humans are important vertebrate hosts for amplifying viral infection. For eastern equine encephalitis virus, the natural cycle is maintained between birds in salt marshes and Culiseta mosquitoes. Transmission to other hosts requires infection of "bridge" mosquito species, such as Aedes and Culex, that feed on a variety of hosts, including humans. Other animals, such as humans and horses, are susceptible to these infections but are unimportant for maintaining these viruses in nature. Other arboviruses may use the same mosquito species for transmission to humans and other hosts. Many cause encephalitis, while others produce fever, rash, arthritis, hepatitis, or hemorrhagic disease. Arboviruses are often named after the disease they cause or the place where they were first isolated. The natural cycle for many arboviruses involves transmission between the insect vector and wild animals or birds. Humans are often only accidentally infected and unimportant for maintaining the virus in nature. However, for dengue and yellow fever viruses, humans are important hosts for the natural cycle and, in concert with the urban mosquito Aedes aegypti as a vector, can lead to explosive outbreaks of human disease. For all groups, the lipid-containing envelope, acquired during budding from host cell membranes, contains surface glycoprotein spikes that are important for attachment and entry of the virion into new cells. Louis encephalitis virus, and Japanese encephalitis virus and the tickborne encephalitis viruses. Dengue virus usually causes a febrile rash disease, but it also can cause a severe vascular leakage syndrome. Bunyaviruses are the most varied and numerous of the arboviruses and include the mosquito-transmitted La Crosse virus in North America and Rift Valley fever virus in Africa, a group of viruses that cause sandfly fever around the Mediterranean, and tickborne Crimean-Congo hemorrhagic fever virus in Africa and Europe (see Table 33-1). Some diseases not transmitted by arthropod vectors are caused by viruses in the same families as arboviruses. For example, the virus that causes rubella belongs to the Togaviridae family, the virus that causes hepatitis C belongs to the Flaviviridae family, and the viruses that cause Hantavirus pulmonary syndrome and hemorrhagic fever with renal syndrome belong to the Bunyaviridae family. Several viruses in the tickborne encephalitis group of flaviviruses are transmitted between animals by ticks. For several days, she had experienced fever, headache, cognitive decline, and difficulty walking. She was active outdoors (president of the local garden club), had not traveled out of the area, and her husband was not ill. She showed no signs of improvement over the next 2 weeks, and life support was withdrawn on day 19 of hospitalization. Serum collected just prior to death was positive for IgG antibody to West Nile virus. Nearly any insect that feeds on humans can also be a vector for infection, including mosquitoes, ticks, sandflies, tsetse flies, black flies, reduviid bugs, fleas, and lice. Viruses, bacteria, rickettsia, protozoa, and helminths are among the infectious agents that can be transmitted by insects. In most instances, the infectious agent must develop and multiply within the vector before it can be transmitted. The geographical distribution of an arthropodborne infection is determined by the habitat requirements of the vector. The temperature, humidity, altitude, and vegetation determine whether vector and host will survive in a specific location.
Order cyclophosphamide paypal
The basis for these differences is not understood but is probably related to the fact that these organisms do not induce as intense an inflammatory response and do not make shiga toxin treatment 101 generic cyclophosphamide 50 mg on-line. In some parts of the world, up to 50% of patients with bloody diarrhea or dysentery are culture positive for Shigella. In contrast, this diagnosis may escape consideration in the mild watery diarrhea caused by S. The presence of leukocytes in diarrheal stool is a simple indicator of an invasive pathogen, and their detection provides immediately useful diagnostic information. Because shigellae die off rapidly when excreted in stool, isolation rates depend on rapid processing of the stool sample, by either streaking directly onto isolation agar or, in field studies, into a transport medium to maintain viability until the sample can be processed. As with other enteric bacteria, media have been designed to detect the lactose-negative phenotype characteristic of Shigella. A rapid presumptive diagnosis can be made by suspending suspicious colonies in saline and carrying out agglutination reactions with antisera to group antigens of Shigella. Testing for biochemical and fermentation patterns allows genus and species identification. Often this ability allows microbes to survive within a host because the secreted molecules aid in microbial survival or dissemination. In Gram-negative cells, toxins are typically delivered extracellularly in a two-step process. In a second step, the toxin is transferred across the outer membrane, apparently without unfolding. Translocation across the outer membrane may require a dedicated protein pore through which the toxin, but not other proteins, can pass. Once extracellular, the secreted toxins gain access to the host cell by first binding to host surface molecules. In contrast to the process described in the previous paragraph, there is no detectable periplasmic form of the protein secreted in this system. Rather, the secreted protein is delivered directly from the microbe into the host cell by a process that has been likened to injection with a syringe. The complex of proteins required for this mechanism is collectively called the injectisome. For Shigella the system is used to transfer proteins that cause the host cell to take up the microbe. Host cell invasion by shigellae is the first step in its eventual intracellular survival and cell-to-cell spread. Some of the conserved proteins appear to form a pore within the host cell membrane, through which other proteins can pass into the cytosol of the host. Once the flagellum is finished being assembled, secretion of the other proteins then ceases. Oral fluids usually suffice to correct the mild-to-moderate degree of dehydration and electrolyte abnormality. In more severe cases that involve bloody diarrhea or dysentery and high fever, the use of effective antibiotics reduces the duration of illness and the period of infectivity to others. Reducing the infective period is particularly important because the small inoculum needed for infection with Shigella frequently results in transmission to other household members. Chapter 17: Invasive and Tissue-Damaging Enteric Bacterial Pathogens: Bloody Diarrhea and Dysentery 211 the use of antibiotics is complicated by the ease with which the organisms acquire antibiotic resistance; it is not pure chance that transferable antibiotic resistance was first discovered in Shigella. To make educated empiric decisions on which drug to use, clinicians should be aware of the drug susceptibility pattern of pathogens encountered in their communities and institutions. No vaccine for shigellosis has been licensed, but many studies are under way using a number of strategies. In some approaches, virulence antigens, the Ipas, are being altered and packaged in various ways; other strategies depend on delivering the O antigen of Shigella in the vaccine preparation. A major goal is to produce live, attenuated vaccines that can be administered by mouth and will immunize the gut itself. Ultimately, however, these vaccines must be tested in humans because no animal model truly mimics human shigellosis. Less often in the United States, bloody watery diarrhea is caused by other pathogens, including Shigella, Salmonella, Campylobacter jejuni, or, more uncommonly, Yersinia enterocolitica. Later that morning, he had a watery diarrhea every 15 to 30 minutes, initially with small amounts of visible blood. Later that day, bright red stools consisting of what seemed to be pure blood appeared. A barium enema revealed edema of the ascending and transverse colon with areas of spasm. The patient was treated with intravenous fluids and gradually recovered over the next 7 days. By the time he was discharged and returned to the nursing home, his stool was negative for that particular E. The laboratory reported a significant decrease in platelets and red blood cells, many of which looked abnormal. No hypertension developed, the renal failure and hemolytic anemia did not progress, and dialysis was not performed. She was discharged 1 week later with no further diarrhea and improvement in the blood count. These strains have a convenient distinguishing characteristic: the inability to ferment sorbitol. O157:H7 clearly causes both outbreaks and sporadic disease, primarily as a zoonosis transmitted from animals to humans. Undercooked hamburger is the principal vehicle, but other food vehicles have been described. Groundwater contaminated in the vicinity of cattle farms can transmit infection as well. The organism appears to be acid resistant, and the estimated infectious dose is very low, approximately 50 organisms per gram of hamburger. It is currently believed that profuse bleeding is caused by the interaction of inflammatory cytokines and shigalike toxins, which damages blood vessels in the lamina propria. When the target is the brain, commonly in older adults, the syndrome is called thrombotic thrombocytopenic purpura. It is quite clear from various studies that the toxin causes these clinical pictures. Shiga toxin is cytotoxic, suggesting that direct damage to glomerular endothelial cells may be the initiating factor of these diseases. Endothelial cell products (including von Willebrand factor, plasminogen activator inhibitor, prostacyclin, nitric oxide, and others) can mediate local pathophysiology leading to platelet thrombi, the characteristic feature of the disease. In the lysogenic state, the phage genes-including the toxin gene-are repressed so their levels are very low or nonexistent. During lytic growth, toxin is expressed at high levels from the phage, and its release is the result of phage-mediated lysis of the host bacteria that occurs after induction. Notice the attaching bacteria and the altered epithelial cell membrane beneath them showing intimate attachment and "pedestal" formation. Chapter 17: Invasive and Tissue-Damaging Enteric Bacterial Pathogens: Bloody Diarrhea and Dysentery 213 infected people. Less severe bloody diarrhea is not so revealing, and diagnosis depends on detecting the organism in stool. An enzyme immunoassay to detect Shiga toxins 1 and 2 is commercially available to detect toxin or any toxin-producing organisms in stool and is both highly sensitive and specific. Thrombotic thrombocytopenic purpura usually responds rapidly to exchange transfusion, for unknown reasons. Some salmonellae are specific to animals and do not cause human disease; some, such as S. The genus Salmonella is vast, comprising more than 2,300 serological varieties (serovars), and the number is growing. One explanation for this association may be that patients with more severe diarrheal disease are more likely to be treated with antibiotics and will thus fare worse than patients with less severe disease, with or without the drugs. Near the end of her visit, she cared for her aunt, who had high fevers and some diarrhea. Her abdomen was diffusely tender, and her liver and spleen were enlarged, although she did not have jaundice. An astute clinician made the presumptive diagnosis of typhoid fever, and therapy with ceftriaxone was initiated and continued for 14 days.
50 mg cyclophosphamide sale
Hookworm infection can be prevented by improved sanitation (using indoor or outdoor toilets or treating feces used for fertilizer) or by protecting the skin from contaminated soil medications voltaren order cyclophosphamide, for example, by wearing shoes. Hookworm infection was common in some areas of the southern United States, where poor sanitary conditions were common until the early part of the last century. However, if the worm burden is large, the infection may cause pain, vomiting, and diarrhea when the number of worms becomes large. Those symptoms occur because, unlike the other intestinal roundworms, the female S. That invasion may cause severe disease, because the early rhabditiform larvae that hatch from the eggs can cross the intestinal wall into the peritoneum and cause intestinal perforations, permitting intestinal bacteria to follow and producing peritonitis. As a result, strongyloidiasis can produce acute clinical syndromes (such as peritonitis) or mimic chronic abdominal problems such as peptic ulcer or gallbladder disease. Reinfection may then occur from larval invasion of the perianal skin, even if the patient has not been exposed to new external sources of infection. Strongyloides autoinfection produces a characteristic snakelike (serpiginous) urticarial rash (larva currens), typically located near the anus. Strongyloides infections may become chronic and produce symptoms for several decades. Those individuals often have chronic syndromes that are misdiagnosed as peptic ulcer or gallbladder disease and fail to respond to medical or surgical treatments for those conditions. Patients in whom autoinfection has been controlled can develop urticarial skin lesions from the migration of larvae at the surface of the skin. In immunocompromised patients, the process of endogenous reinfection may produce a hyperinfection syndrome that is sometimes fatal. She apparently maintained an asymptomatic Strongyloides infection by the mechanism of autoinfection. With the administration of corticosteroids later in life, the infection was no longer controlled, and she experienced respiratory and abdominal symptoms. However, they become unable to control the infection when their cell-mediated immunity is compromised by the immunosuppressive drugs used to prevent rejection of the transplanted kidney. Because the hyperinfection syndrome is often seen in patients with impaired cell-mediated immunity, it seems likely that this kind of immunity is the critical factor in the control of strongyloidiasis. Because the worms lay their eggs in the bowel wall, the eggs (which closely resemble hookworm eggs) are rarely found in the stool. It is more typical to diagnose Strongyloides by identifying rhabditiform larvae in the stool. Patients with strongyloidiasis typically have a marked eosinophilia (10 to 20% of white blood cells, >10,000 to 20,000 eosinophils/L of blood). The magnitude of the eosinophilia in persons with the hyperinfection syndrome may be limited by the basic T-cell defects predisposing to the syndrome, the outpouring of neutrophils resulting from secondary bacterial infection, and corticosteroid therapy. Patients thought to have strongyloidiasis should be studied first by stool examination. Even if three or more stool examinations reveal no larvae, examination of the duodenal contents or duodenal biopsy could be positive. An individual tapeworm is actually an animal colony, because each segment (known as a proglottid) is a self-contained unit capable of reproduction, metabolism, and food uptake (a tapeworm has no common gut). A tapeworm attaches to the intestinal wall by a head (scolex) that has sucking disks or grooves. In their intermediate animal host, tapeworms penetrate deep tissues and develop into infective, cystic larval forms. During a diplomatic reception, they were served steak tartare (highly seasoned raw beef), a traditional dish in that region. She experienced nausea, apparently brought about by seeing the worms in her stool. Laboratory studies revealed that the segments were proglottids of Taenia saginata. On the other hand, he could understand her revulsion at seeing the worm segments in her stool and visualizing the rest of the worm inside her. The clinical picture of intestinal infection is generally mild and is essentially the same for all tapeworms. Unfortunately, confusion is possible because one tapeworm (pork tapeworm) can produce both taeniasis and deep tissue infection in the same patient. The eggs hatch in the intestine of cattle and enter the bloodstream to lodge in peripheral tissues, where they develop into cysticerci (see Chapter 55). Beef tapeworm infection only exists in areas where infected humans defecate in grazing areas for cattle. All human intestinal tapeworm infections correlate with gastronomic preferences: They are found mainly among people who consume their meat undercooked or raw (as in the case of Mrs. Life cycle of intestinal tapeworms Taenia solium (pork tapeworm) and Taenia saginata (beef tapeworm). Humans acquire intestinal tapeworm infections by ingesting the tissue stage of the parasite (cysticercus) in inadequately cooked meat (1). The parasite then hatches in the intestine (2) and matures to an intestinal tapeworm (3). The pork tapeworm (outside diagram) has a crown of spines on its head and fewer pairs of lateral uterine branches in its proglottids (segments) than the beef tapeworm (4). When human feces containing viable eggs are ingested by either pigs or cattle, the eggs hatch (7) and produce the tissue (cysticercal) stage of the infection in those animals (1) to complete the cycle. Cooking effectively destroys the larvae, but cooks have been known to become infected by tasting raw food during preparation. For example, fish tapeworm infection is said to be an occupational hazard of Jewish or Scandinavian women in the north-central United States who make gefilte fish or lutefisk. Those who are not cured often have nausea or vomiting with their first treatment and typically respond to a second treatment with the drug. Patients with cysticercosis require a different approach to therapy (see Chapter 55). The infection is usually noted only because of the presence of tapeworm segments (proglottids) in the stool. Almost half the people infected with fish tapeworm have low levels of vitamin B12, leading to serious megaloblastic anemia. The B12 deficiency appears to be the result of competition between the host and the parasite for that vitamin in the diet. The intestinal disease caused by tapeworm is very different from the tissue disease (see Chapter 55). With the exception of Strongyloides, helminthic parasites have no capacity to increase their numbers in the infected host. Therefore, the worm burden in infections other than those caused by Strongyloides is directly related to the size of the ingested inoculum (or the accumulation of repeated inocula). Because Strongyloides infection can be asymptomatic and sustained, the hyperinfection syndrome can occur during immunosuppression decades after the initial exposure. Hyperinfective strongyloidiasis in the medical ward: review of 27 cases in 5 years. Pulmonary infiltrates, asthma and eosinophilia due to Ascaris suum infestation in man. Although the eggs of pork and beef tapeworms are identical, their proglottids can be distinguished by the experienced observer (those of T. Encounter: Trichinosis is maintained by a "cycle of carnivorism" in which predators and scavengers feed on each other and acquire larvae encysted in muscles. Humans usually acquire infection from undercooked meat from pigs or carnivorous game animals.
