
Discount fluticasone 500 mcg on line
Routine monitoring by mycobacterial culture of sputum is rarely feasible in developing countries in the tropics asthma symptoms checker discount 500 mcg fluticasone visa. If sputum smears remain positive at this stage despite careful adherence to treatment it may indicate that the patient had a particularly heavy initial bacillary load. If smears remain positive after a month of the continuation phase, this constitutes treatment failure and the patient should be restarted on a full course of an appropriate re-treatment regimen (see Table 12. At the end of the treatment course, treatment outcomes are recorded according to one of six categories shown in Table 12. Protecting others from infection is, on the whole, best achieved by careful chemotherapy rather than physical isolation. Such individuals are usually identified by skin testing and are either contacts of known smear-positive index cases or people who are occupationally exposed to infection (such as nurses and doctors). The success of this strategy depends on the implementation of a fivepoint package. Tuberculosis control activities should aim to meet two minimum targets: a cure rate of 85% and a case detection rate of 70%. The standardized outcome reporting categories described above make it possible to conduct quarterly cohort analyses of treatment outcomes and hence to report cure rates. Isoniazid preventive therapy the rationale behind preventive therapy is to eradicate latent infection before it develops into active disease. Many now accept that this system does not always make it easy for patients to adhere to every prescribed dose of treatment. If, for example, patients live far from the health care worker, they will inevitably incur considerable direct and opportunity costs in the daily travel required. The guiding principle should be to make it as easy as possible for patients to stick with therapy for the full course. The increasing use of three- and four-drug fixed-dose combinations to supplement the existing two-dose combinations of rifampicin and isoniazid should make it easier for patients to adhere (because of reduced pill burden) and harder for drug resistance to emerge. Estimating the expected number of infectious cases in a given population requires full-scale community-based prevalence surveys or longitudinal cohort studies. These are expensive and time-consuming and most countries have not had the resources to undertake them. The process of case detection needs close attention, especially if it is to work for those who need it most, i. The process of sputum submission takes the patient a minimum of 24 h and three visits to the health facility followed by another visit to collect the results and, usually, one further visit to start treatment. These repeat visits may be impossible for particularly disadvantaged patients such as the poor and women in some traditional cultures. In some instances this means establishing extra laboratory services (but no more than one such facility for 100 000 people, as the volume of work is then not sufficient for staff to retain skills). In other instances this means ensuring excellent logistics for transporting specimens and results between microscopy centres and collection sites. The requirement for 3 sputum specimens in order to categorize patients has been relaxed and it is now recognized that 2 specimens are sufficient, provided the quality of the smear microscopy can be assured. A recent large-scale, multicentre randomized trial has also indicated that collecting the first two specimens one hour apart provides sensitivity that is equivalent to that achieved when the specimens are collected on consecutive days. All these steps towards one-stop diagnosis have great benefits for improving access by poor and disadvantaged groups. However, it, or related approaches (sometimes called intensified case-finding), may be appropriate in some situations. This mortality appears to be multifactorial and includes late initiation of treatment. This may be partly a result of the difficulties of diagnosis but stigma and other factors also contribute. Early detection of drug resistant cases may mean that conventional monitoring of therapy by smear microscopy needs to be rethought. New interventions No new drug regimen looks set to replace the current gold standard 6-month short-course chemotherapy in the short term, but there are suggestions that adding moxifloxacin to first-line regimens will enable shorter treatment regimens to be developed. Point of care tests will improve this when they become cheaper for use in resource-poor settings. Dual infections can occur and there is no evidence that one infection protects against the other. Both viruses cause the same immune defects and are associated with a similar disease. They define the national testing algorithms and counselling protocols and also set standards for logistics, data management and quality assurance. Here the counsellor offers a more client-focused, couple or family pre-test counselling session with test results accompanied by counselling, referral and linkage to facility-based treatment and care services. Many are available as single kits and so can be efficiently used when small numbers of samples need testing. Patients thought to be seroconverting should be followed up within two weeks of the first test for confirmatory testing and enrolment in care and treatment. As a minimum, a national algorithm should recommend serial testing, where every reactive result is confirmed with a second test before a positive result is given out. In high prevalence countries it may be cost effective to have a parallel testing algorithm, where all positives and all negatives are automatically confirmed, as this saves cost time and effort in recalling all those with reactive results. The national reference laboratory is responsible for external quality assurance of all testing. Accurate diagnostic testing for infants below this age therefore requires virological testing i. If this is unavailable, regular clinical monitoring should take place until antibody tests can be used. In resource-poor settings, often few resources are available for epidemiological monitoring. With experience and institutional strengthening, surveillance is now much more accurate. Other groups commonly monitored include pregnant women attending for antenatal care, blood donors, military recruits and newborn infants, although all these groups have inherent biases. Ideally, a representative population-based sample should be tested at regular intervals to accurately determine prevalence and incidence in a particular region. This provides the most valuable information, but population-based testing is difficult and expensive to organize. Global seroprevalence With rapid spread of infection (and delays in reporting and analysis) current figures quickly become out of date. The largest regional increases in prevalence are occurring in Eastern Europe and central Asia block countries, largely driven by injecting drug users. While the majority of infection is via the heterosexual route there is increasing recognition of the importance of sex between men as a driver of the epidemic in Africa, Asia and other settings in the tropics. There are numerous factors such as the age and sex of the individual (young women seem more susceptible, perhaps because of an immature genital tract), as well as the factors mentioned below. Transmission by infected blood Two groups are at particular risk: patients receiving blood transfusions and people who inject drugs and share needles and syringes. Improperly sterilized injection equipment in hospitals and other health facilities is another (unquantifiable) risk. T-helper lymphocytes have an important role in the regulation of the cell-mediated immune response and also cooperate with B cells in the production of antibody. Cytokine secretion by infected macrophages is aberrant and may have a role in chronic fever, wasting and enteropathy. Progressive immunosuppression With the progressive destruction of one part of the immune system, a distinct form of immunosuppression develops. At this stage disease presentations are clinically typical and there is normal response to standard treatment. As with other immune deficiency syndromes, a relatively limited number of organisms are able to exploit the specific immune defect and commonly cause disease in seropositive individuals. Common pathogens occurring in advanced infection are Cryptococcus neoformans, Toxoplasma gondii, Pneumocystis jirovecii, human herpes virus 8, cytomegalovirus and varicella zoster virus. Disease is caused by acute infection or by reactivation of a dormant or contained organism.
Cheap fluticasone 250mcg overnight delivery
It is prepared as a solution in propylene glycol and is given by slow intravenous infusion asthma 2014 soundtrack order 500mcg fluticasone with mastercard. However, it is an efficacious agent that can be used for late stages of trypanosomal disease, although resistance has been reported. Its metabolism has not been well studied, but it is excreted predominantly in the urine. Melarsoprol is active in the treatment of all stages of African trypanosomiasis due to T. Melarsoprol is commonly associated with significant toxicity, including vomiting, abdominal pain, hepatotoxicity, peripheral neuropathy, hypersensitivity reactions, myocarditis, cardiac arrhythmias, and albuminuria. Administration can also lead to a reactive encephalopathy in up to 10% of patients, and this is associated with significant mortality. The injection is very irritating, and extravasation during intravenous administration should be avoided. It is not absorbed when given orally and is usually administered as a 10% solution by slow intravenous infusion. Following intravenous injection, it is rapidly distributed, and >99% becomes bound to plasma proteins. It should not be used in the presence of renal failure or significant hepatic dysfunction. An advantage of suramin is that it has macrofilaricidal activity, damaging the intestinal epithelium of adult O. Potential side effects include an immediate reaction, with nausea, vomiting, shock, and loss of consciousness, following suramin injection. Other adverse effects include renal impairment, exfoliative dermatitis, and neurological toxicity. No case of infant malformation has been Eflornithine the main indication for use of eflornithine (also known as difluoromethylornithine) is for treatment of African trypanosomiasis. Drug availability is limited, and it is not available in the United States for systemic use. Eflornithine selectively and irreversibly inhibits ornithine decarboxylase, an enzyme required for the formation of polyamines needed for cellular proliferation and differentiation in parasites. Eflornithine can be administered by mouth and has >50% oral bioavailability, but significant diarrhea frequently results, so it is usually given intravenously. It displays some activity against other parasites, including Plasmodium species, C. Common adverse reactions include vomiting, abdominal pain, diarrhea, dizziness, arthralgias, hearing loss, and rash. Bone marrow toxicity resulting in anemia, thrombocytopenia, and leukopenia has also been described. There are no good studies of its safety in pregnancy or lactation (pregnancy category C), so it should only be used when the potential maternal benefits outweigh the possible risks to the fetus. Side effects are common with benznidazole and are seen in up to 40% of treated individuals, commonly including vomiting, abdominal pain, peripheral neuropathy, rash, and pruritis. Nifurtimox has significant side effects that preclude the completion of therapy in many patients. Adverse effects include anorexia, nausea, rash, headache, sleep disturbance, peripheral neuropathy, and myalgias. Benznidazole crosses the placenta, but there are minimal data regarding teratogenic effects for either agent in either animals or humans (168). Nifurtimox is detected in breast milk, so caution is recommended during breast feeding (169). Similarly, safety data for benznidazole and lactation are lacking, so withholding treatment during breast feeding is again recommended. Flubendazole: a candidate macrofilaricide for lymphatic filariasis and onchocerciasis field programs. Ceballos L, Virkel G, Elissondo C, Canton C, Canevari J, Murno G, Denegri G, Lanusse C, Alvarez L. A pharmacology-based comparison of the activity of albendazole and flubendazole against Echinococcus granulosus metacestode in sheep. Treatment of human pulmonary paragonimiasis with triclabendazole: clinical tolerance and drug efficacy. Administration of triclabendazole is safe and effective in controlling fascioliasis in an endemic community of the Bolivian Altiplano. Apparent triclabendazole-resistant human Fasciola hepatica infection, the Netherlands. Nifurtimox and Benznidazole the two agents used for treatment of American trypanosomiasis are nifurtimox and benznidazole. Nifurtimox is a synthetic nitrofuran, and benznidazole is a 2-nitroimidazole derivative. It is thought to cause increased phagocytosis, cytokine release, and production of reactive mitogen intermediates that result in destruction of intracellular parasites (160). The mechanism of action of nifurtimox seems to be related to its metabolism to chemically reactive radicals that cause production of toxic reduced products of oxygen, such as superoxide, hydrogen peroxide, and hydroxyl radicals (12, 161). These compounds accumulate within trypanosomes, leading to toxic effects, including membrane damage and enzyme inactivation. Benznidazole is available for oral administration and has a bioavailability of >90%. Dose reduction is advised for patients with significant hepatic or renal impairment, but no specific guidelines exist. Neither agent has demonstrated efficacy in late stages of disease, and indications for treatment of chronic infection remain controversial but are expanding (164 166). No randomized trial has evaluated the comparative safety and efficacy of nifurtimox and benznidazole in adults (167). Nifurtimox is now also increasingly being used in combination with eflornithine for first-line treatment of T. It also has been shown to have some activity in leishmaniasis but is not routinely used for this indication. Serum ivermectin levels after enteral and subcutaneous administration for Strongyloides hyperinfection: a case report. Ivermectin distribution in the plasma and tissues of patients infected with Onchocerca volvulus. A randomized, double-blind, multicenter clinical trial on the efficacy of ivermectin against intestinal nematode infections in China. Albendazole and mebendazole administered alone or in combination with ivermectin against Trichuris trichiura: a randomized controlled trial. Ivermectin in human medicine, an overview of the current status of its clinical applications. Loa loa encephalopathy temporally related to ivermectin administration reported from on- 17. Analysis of benzimidazoles in body fluids by high-performance liquid chromatography. Pharmacokinetics of combined treatment with praziquantel and albendazole in neurocysticercosis. Albendazole-praziquantel interaction in healthy volunteers: kinetic disposition, metabolism and enantioselectivity. Concentrations of albendazole in serum, cerebrospinal fluid and hydatidous brain cyst. Efficacy of current drugs against soil-transmitted helminth infections: systematic review and meta-analysis. Albendazole and its metabolites in the breast milk of lactating women following a single oral dose of albendazole. Praziquantel: mechanisms of action, resistance and new derivatives for schistosomiasis. Albendazole plus praziquantel versus albendazole alone as a pre-operative treatment in intra-abdominal hydatisosis caused by Echinococcus granulosus. Antiparasitic Agents n chocerciasis mass treatment programs from 1989 to 2001: implications for the future. Assessment of the efficacy of diethylcarbamazine on adult Wuchereria bancrofti in vivo. Efficacy of diethylcarbamazine in eradicating infection with lymphatic-dwelling filariae in humans.
Cheap 250mcg fluticasone free shipping
Of the transplants since 2000 asthma treatment guidelines stepwise generic 500mcg fluticasone with visa, the most common cause of graft failure was chronic rejection (41%), followed by acute rejection (10%). While vascular thrombosis continues to be an important cause of graft failure (7%), the proportion of grafts lost to this event has decreased in the more recent era (2000Ͳ007). Approximately 12% of reported graft failures had unknown causes in the database, and death with a functioning graft represented 10% of graft losses. Some of these factors are more predictive of short-term survival while others have an effect on long-term graft survival. Finally, for deceased donor kidneys, outcomes are superior for pediatric recipients of grafts from donation after brain death than donation after cardiac death due to increased risk of graft loss by 4 years in the latter. However, short-term graft survival for this age group has improved in the recent era. Transplants from very young donors (under age 5 years) to pediatric recipients have historically been avoided due to reports of increased risk of graft loss. There is some evidence that donation from a sibling with non-inherited maternal antigens confers survival benefit42,205 for the graft and may be due to bidirectional immune regulation57 between donor and recipient immune cells. This has particular relevance for pediatrics, since mothers represent the majority of parental donors. Children in the United States receive fewer zeromismatched kidneys than adults (3% of pediatric recipients versus 8% of adults) under the current allocation policy. Therefore, the risk of sensitization from mismatched primary transplants may have a negative impact on this population if it becomes a barrier to subsequent transplant. The practice of donor-specific blood transfusion has fallen out of favor in the recent era given lower rejection rates on the newer immunosuppression regimens. This finding could relate to prolongation of operative time and cold ischemia time, increased third spacing of fluid, more complex postoperative fluid management, and increased risk of poor graft perfusion. Risk factors for graft thrombosis in children include recipient age <6 years, donor age <6 years, cold ischemia time >24 hours, and history of peritoneal dialysis. Finally, issues with medical compliance or unstable family situations can delay consideration for kidney transplant. Situations that might not be appropriate for referral or listing include active or untreated malignancy, active or untreated infection, and multiple or progressive medical conditions with overall poor prognosis for recovery. Transplant is considered following a reasonable disease-free period for children with prior malignancies. Mild, isolated mental retardation is not a contraindication to transplant per se, as improvement in neurocognitive development has been seen following transplant. It is usually characterized by nephrotic-range proteinuria (protein/creatinine ratio >2 mg/mg) and hypoalbuminemia, but can present as complete nephrotic syndrome, including anasarca and hypercholesterolemia. Biopsies early following recurrence often demonstrate normal histology on light microscopy with effacement of podocyte foot processes on electron microscopy. It is likely a multifactorial process involving cytokines secreted by T cells,174,337 a humoral factor that alters podocyte cytoskeletal structure,129,288 and a balance between circulating permeability factors and inhibitors of such factors. Some centers perform plasmapheresis either before a planned living donor transplant or in the perioperative period of deceased donor transplant. Other causes include deficiency of factor H,76 or presence of an inhibitory autoantibody against factor H,203 the natural inhibitor of C3bBb. No correlation was found between pretransplant presentation or C3 levels with the risk of recurrence or graft loss. Non-specific treatments using angiotensin blockade, steroids, anticoagulation, or antiplatelet therapy have been reported in the literature with variable success. In patients with deficiency in factor H, plasma infusion can be used to correct the deficiency. As high as 40͵0% of patients with recurrence have been reported to have graft failure in some single-center studies155,256; however, a recent analysis of patients in East Asia found that chronic rejection had a larger effect on long-term graft survival rate in patients with IgA nephropathy. Epidemiological studies estimate that 5ͱ0% of children with Shiga toxin-producing E. Cases typically have large bacterial burden with empyema and bacteremia, but cases with meningitis or pericarditis have also been described. T-antigen exposure can be confirmed on patient erythrocytes using the lectin Arachis hypogaea. Genetic or acquired disorders of complement regulation are identified in about 60ͷ0% of these cases. The risk of recurrence following transplant varies depending on the genetic mutation identified. While early attempts resulted in acute thrombotic events and high mortality rates, several centers in Europe have reported improved outcomes with ancillary plasma exchange and anticoagulation therapies. However, the risk of morbidity and mortality has limited the use of this approach. While studies of long-term outcomes are not available, a requirement for lifelong therapy is anticipated. Membranous Nephropathy Membranous nephropathy is rare in children, so risk of recurrence in children following transplant is not clear. This is likely owing to the late presentation of recurrence, which for most patients who are transplanted as adolescents would occur in adulthood. Average time to recurrence is 31 months, but can occur within weeks to many years following transplant. Renal recurrence is often heralded by microscopic hematuria and proteinuria with focal or diffuse pauciimmune necrotizing glomerulonephritis seen on biopsy. Adult-sized kidneys from living donors have excellent potential for long-term graft survival in pediatric recipients. Live donation from a sibling is also considered, but most programs do not routinely accept donors under the age of 18 years on ethical grounds. More than 100 different mutations have been described and there is considerable phenotypic heterogeneity, even within family members with identical mutations. The most severe form presents in infancy with renal failure necessitating dialysis. In children with less severe presentation and early diagnosis, conservative management with pyridoxine (thought to reduce oxalate production in a subset of B6-responsive patients), increased fluid intake, and citrate treatment might delay the progression of kidney disease. While nephropathic cystinosis does not recur posttransplant, protocol biopsies have shown interstitial deposition of cystine crystals Evaluation of Recipient Many similarities exist in the medical evaluation of potential pediatric and adult transplant recipients (see Chapter 4). However, certain conditions occur more frequently in children, so the medical evaluation of pediatric recipients has a slightly different emphasis. The following section describes the common medical, surgical, and psychological issues taken into consideration during the pretransplant evaluation of a pediatric patient. Chronic fluid overload can result in left ventricular hypertrophy and dilated cardiomyopathy. Impaired systolic function following transplant can impair perfusion of the allograft, increasing the risk of delayed graft function and impacting graft survival. Therefore, aggressive management of persistent hypertension, including intensified dialysis treatment and optimization of pharmacotherapy in children on dialysis, is paramount to successful transplant outcomes. Among hypertensive or other at-risk patients, echocardiography at the time of pretransplant evaluation and periodically thereafter (semi-annual to annual basis) can identify patients at highest risk for cardiovascular morbidity. Bilateral nephrectomy is sometimes required to control recalcitrant hypertension in children with elevated blood pressures despite multiple antihypertensive medications and optimized fluid management (see section below). Active nephrotic syndrome with hypoalbuminemia at the time of transplant can complicate postoperative fluid management because of increased third spacing, thereby increasing the risk of electrolyte derangement, graft hypoperfusion, thromboembolic events, and delayed graft function. Native nephrectomies have been utilized at some centers to minimize this confounding variable. Persistent hyperparathyroidism following kidney transplant can result in hypercalcemia and limits growth potential. The risk of developing persistent hyperparathyroidism after transplant is attributed to hyperplasia of the parathyroid gland. Over time, uncontrolled secondary hyperparathyroidism can lead to nodular transformation and monoclonal growth, resulting in tertiary hyperparathyroidism (resistant to vitamin D therapy). As mentioned previously, most centers prefer pediatric patients to achieve a weight of 10ͱ5 kg prior to kidney transplant, and infants on dialysis may not reach this goal prior to 2 years of age. Pediatric transplant candidates should be free from active infection to prevent infectious complications posttransplant.
Cheap 500mcg fluticasone otc
However peep 0 asthma buy fluticasone once a day, strains clinically resistant to metronidazole can have cross-resistance to tinidazole. Drug resistance occurs when transcription of one or more of these enzymes is decreased, and laboratory-generated resistant isolates have smaller hydrogenosomes (80). However, clinical resistance does not correlate with lower transcript levels of these enzymes or smaller hydrogenesome size (80, 81). The nitroimidazole drugs are also reduced by the flavin enzyme thioredoxin reductase and covalently bind and inhibit proteins associated with thioredoxin-mediated redox regulation (82). Furthermore, use of a flavin inhibitor rendered a normally susceptible isolate resistant to high concentrations of metronidazole. A third possible mechanism for nitroimidazole resistance was suggested by the observation that trichomonas isolates that harbored Mycoplasma hominis symbionts had a mean in vitro resistance level 10-fold higher than noninfected trichomonads (84). In a separate study, there was no association of mycoplasma infection with clinical resistance (85). It remains unclear which, if any, of these mechanisms is responsible for the clinical nitroimidazole resistance observed in some T. Treatment of patients who have metronidazole-resistant trichomoniasis often results in an immediate resolution of symptoms and a negative wet mount. However, within 3 to 4 weeks, in the absence of further exposure, symptoms may recur as the number of organisms rises. Thus, it is important to monitor efficacy of treatment for up to a month and to encourage patients to avoid unprotected intercourse during this time. When nitroimidazole resistance is encountered, patients are often successfully treated with increased doses of drug for a longer time (71, 72); however, many patients cannot tolerate high doses of metronidazole and such practices may only exacerbate the development of drug resistance. In addition, some patients experience hypersensitivity reactions in response to metronidazole and tinidazole. While no drugs were as effective as the 5-nitroimidazoles, some enhanced the activity of metronidazole when used in combination (87). Intravaginal treatment with drugs such as furazolidone and paromomycin sulfate that are not absorbed well from the intestine or cannot be ingested has been successful to cure some patients but, in general, has limited efficacy (86, 88). Povidone-iodine and boric acid have also shown efficacy for some patients but additional clinical testing is needed (88, 89). Depending in part on which of the possible 20 species of Leishmania that infects humans is present, pathology can range from a cutaneous lesion that is self-limiting to the more severe mucosal or visceral forms. Use of antileishmanial drugs is limited by their high cost, the difficulty of their administration (injections for several weeks), and/or their associated toxicity. These factors are even more consequential in the developing countries where leishmaniasis is endemic and can lead to premature selftermination of therapy, which in turn may promote increased levels of resistance (92). While true drug resistance has been described for isolates of some Leishmania spp. True resistance is more likely in anthroponotic forms of leishmaniaisis, such as Leishmania donovani and Leishmania tropica, because the zoonotic species that primarily infect animals, with humans as an occasional host, rarely encounter drugs and serve as a reservoir for drug-sensitive parasites (94, 97). The frontline drugs for treating Leishmania infections caused by all species and all clinical forms have long been the pentavalent-antimonial compounds such as sodium stibogluconate and meglumine antimoniate. These compounds are inexpensive compared to other anti-leishmanial drugs but their extensive use has led to widespread treatment failure. For example, in some areas of endemicity in India, treatment failure of visceral leishmaniasis caused by L. Evidence for true drug resistance in this setting comes from observations that isolates from clinically resistant patients require higher in vitro concentrations of drug to kill the parasites than do isolates from patients who respond to treatment (99). However, the correlation between clinical outcome of treatment for leishmaniasis and the in vitro susceptibility of the causative isolate is not always clear (9395, 100). Adding to the difficulty of defining resistance mechanisms, more than one of these mechanisms may arise, even within closely related parasite strains (101). Genomic, proteomic, and metabolomic approaches have further revealed the complex, multifactorial nature of antimonial resistance in Leishmania spp. Because of the high level of pentavalent-antimonial resistance, this treatment is no longer considered useful in parts of India and, in these places, miltefosine is now the primary treatment for visceral leishmaniasis (96, 112). Miltefosine was originally developed as an anti-cancer drug and is particularly promising because it can be taken orally and has fewer side effects than most of the parenteral treatments for leishmaniasis (113). As a result, although the drug is more expensive than other therapies, it can be administered on an outpatient basis, reducing the overall cost for treatment in comparison to less costly drugs that require hospitalization. Enthusiasm is tempered, however, both because it is teratogenic, thereby limiting its unregulated use in women of child-bearing age, as well as the observation that leishmanial resistance to miltefosine develops easily in vitro (113). Relapse rates of 20% within 1 year after miltefosine treatment have already been reported (114). However, recent studies suggest that these mechanisms do not explain all of the clinical resistance to miltefosine and other mechanisms, such as infectivity of the parasite strain, may be involved (112, 114, 118). Another drug now being used for primary treatment of visceral leishmaniasis is amphotericin B, which interacts with parasite-specific 24-alkyl sterols and induces pore formation in the parasite plasma membranes (92). The use of amphotericin B has been limited in the past due to its high cost and toxicity; however, new lipid-associated formulations of amphotericin B have greatly reduced toxicities and retain good efficacy even when administered in lower doses (119). Like the pentavalent antimonials, optimal activity of amphotericin B may require competent host immune responses (120, 121). Lipid-associated formulations of amphotericin B are phagocytized by host monocytes and accumulate in the phagocytic lysosomes where Leishmania amastigotes reside. Interestingly, although the mode of action of amphotericin B is thought to differ greatly from that of the antimonials, field isolates indicated that those with greater sodium-antimonygluconate resistance had greater in vitro resistance to ampho- 150. As with the other anti-lesihmania drugs, amphotericin B resistance is associated with greater drug efflux and altered thiol metabolism (122). Part of the challenge for understanding drug activity and treatment failure during leishmaniasis relates to the intracellular location of the amastigotes within host macrophages. As a result, treatment efficacy involves host factors in addition to the parasites and therapeutic compounds (123). While melarsoprol treatment failure may be as high as 20% in some settings (136), field resistance to eflornithine and nifurtimox has not been documented. Nevertheless, resistance in laboratory strains has been readily induced for both drugs (137, 138). Eflornithine resistance is associated with the loss of a nonessential amino acid transporter that is responsible for drug uptake, raising the concern that field resistance could easily develop (137). The two subspecies are endemic in eastand west-central Africa, respectively, with T. Because these parasites possess antigenic-switching mechanisms, host immune responses are ineffective and the prospects for the development of vaccines against these organisms are meager. Control efforts have largely been focused on prevention through reduction of the tsetse fly vector, usually through traps or insecticides (126). However, recent political unrest with subsequent loss of an effective public health infrastructure in parts of Africa has caused a resurgence of this disease. As a result, drug treatment is the only medical intervention available to combat sleeping sickness for the foreseeable future. Pentamidine and suramin are drugs used for treatment of the first stage but not advanced disease because they are highly ionic and do not cross the bloodbrain barrier. While clinical resistance to these drugs does not seem to be a problem, failures can occur when infections are diagnosed and treated after disease has progressed past the hemolymphatic stage. Late-stage, central nervous system disease is treated with melarsoprol, eflornithine, or nifurtimox-eflornitihine combination therapy (126, 128). Pentamidine and melarsoprol share an amidinium-like moiety with amino purines that is recognized and actively taken up by nucleoside transporters in the trypanosome membrane, resulting in concentration of these compounds within the parasite (127). However, tbat1 knockout parasites were only partially resistant, leading to the Drug resistance in human helminths is rare, a fact attributed to their long reproduction cycles and to their lack of multiplication inside the human host (the exception being Strongyloides stercoralis). Thus, when considering treatment failures in schistosomiasis, it is important to distinguish characteristics leading to reduced drug efficacy from true drug resistance. For example, persons with very high levels of infection are less likely to be cured with single-dose therapy than individuals with lower worm burdens (139, 140). This is in part related to the fact that the standard drug used to treat schistosomiasis, praziquantel, is only effective against the adult stage of the parasite and, even under the best conditions, a single dose of praziquantel does not demonstrate complete efficacy (141, 142). Immature worms that may be present at the time of drug treatment, especially in areas of high transmission, are not susceptible to the initial treatment and subsequently develop into patent infections that give the impression of drug resistance. As a result, two treatments spaced 4 to 6 weeks apart are more effective than a single treatment and should be attempted when drug resistance is suspected (139, 143, 144). Rapid reinfection in areas of high transmission should also be considered as a possible explanation for apparent praziquantel-treatment failure (145, 146). Suspected true praziquantel resistance has been described for Schistosoma mansoni infections in Egypt and Kenya (147, 148).
Order fluticasone 500 mcg on line
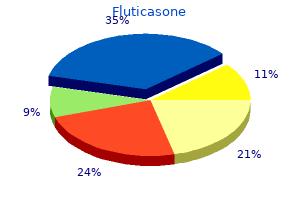
The size of the circles represents the health expenditure in the six World Health Organization regions asthma treatment nih cheap 250 mcg fluticasone overnight delivery. Africa, with almost 25% of the global disease burden, has less than 5% of the healthcare workforce and spends the least on healthcare. In a recent report from Nigeria, less than 2% of patients initiated on dialysis were still receiving treatment 1 year later. Of the developing regions, Latin America is faring best, with the prevalence of dialysis treatment 320 pmp. Despite these challenges, even some of the poorer countries are initiating dialysis programs, albeit on a restricted basis. These initiatives are often launched with the effort of dedicated individuals supported by international organizations such as the International Society of Nephrology. In order to ensure some fairness and equity in the allocation of dialysis, some countries have so-called Life or Death Committees that decide on who should be offered renal replacement treatment. When transplants are done, it is crucially important that the timing of transplantation be optimized, graft function maximized, and costs and complications minimized. Hemodialysis Globally, hemodialysis is the preferred mode of dialysis despite the many advantages of peritoneal dialysis in the developing countries setting. Water quality is often substandard with very high aluminum content resulting in excessive blood and bone aluminum levels. Staphylococcus aureus is the most common pathogen (60%), of which 35% are methicillinresistant. Dialysis is a highly resource-intensive treatment that few governments are able to afford. Because of insufficient government support, chronic dialysis is poorly organized, lacks clear policies, and is largely unsustainable, because of the need for out-of-pocket payments by patients or their supporters. At less than 20 persons pmp the lowest treatment rates in the world prevail in sub-Saharan Africa (with the exception of South Africa, that has a treatment rate of 70 pmp). Inset: the relative overall renal replacement activity in developed and developing regions in 2001. The outcome of patients on peritoneal dialysis is particularly dismal in some developing countries. Reasons for the poor outcomes include the high peritonitis rates, poor nutrition, poor patient selection, poor adherence, and the late presentation of patients. Peritoneal dialysis offers patients greater independence and mobility, and may allow breadwinners to return to work. Organizationally, it does not require the major capital expenditure associated with setting up a hemodialysis unit and it it possible to service large numbers of patients, even in remote areas. Peritoneal dialysis would be an ideal form of renal replacement treatment in a developing country setting. The chief reason for its limited use is the high cost of treatment in developing countries because peritoneal dialysis solutions have to be imported. In developing countries, the dose of treatment is related to available resources, and many patients are unable to afford the standard three to four exchanges per day. The introduction of new connection technology, such as the Y-system and twin-bag system, has resulted in a significant reduction in acute peritonitis rates. Lack of legislation, infrastrucure, resources, and cultural factors, as well as ignorance, contribute to the ongoing shortage of organs. Although the transplant rate is a function of the healthcare system, cultural beliefs and values are also important barriers. Developed countries are able to satisfy 30ͳ5% of their transplant needs, in contrast to developing countries, where only 1Ͳ% of the estimated need for organ transplantation is met. Living donors may be related, spouses, or unrelated; deceased donors may be heartbeating or non-heartbeating. In a recent report from Korea, living related transplants declined from 84% in the 1970s to 61% in the 2000s; living unrelated transplants increased from 14% (1970s) to 37% in the 1990s but declined again in the 2000s to 19%, perhaps reflecting the international condemnation of commercial transplantation. Despite the large size of extended families, with on average six genetically related members being available at initial workup, almost half of potential donors are eliminated because of comorbid disease while one-quarter refuse to donate. After some initial resistance, most religious commentators, including Islamic, Christian, Hindu, Judaic, and Buddhist, support solid-organ transplantation. Saudi Arabia is an excellent example of a conservative Muslim country that has implemented a deceased donor program successfully. The growth of the deceased donor program in Latin America is another example of what can be achieved with the combined effort of the medical community and governmental involvement. Several developed countries report good results with the use of kidneys from non-heartbeating donors but it is a source that is yet to be explored by developing countries. Barriers to Transplantation Programs A range of obstacles hinder the development of transplant programs in developing countries. Health authorities tend to prioritize these diseases over chronic kidney failure, which is seen as affecting a relatively small proportion of the population, is expensive to treat, and requires vast resources. Developing countries rely more heavily, and in many cases, exclusively on living organ donors. The number of countries transplanting has increased and even some of the poorer countries are initiating transplant programs, emphasizing the growing global demand. A call for government accountability to achieve national self-sufficiency in organ donation and transplantation. A successful kidney transplant program requires a dedicated team consisting of surgeons (urologists, vascular surgeons, transplant surgeons), nephrologists, pathologists, as well as the backup of a good radiology and laboratory service, not to mention a dialysis service. The severe shortage of intensive care unit beds in developing countries can be a major limitation. A reliable tissue-typing laboratory also is an essential service for the success of a deceased donor transplant program. In Saudi Arabia, the government took a leading role and established a national procurement agency responsible for the supervision of organ donation and transplantation, emphasizing the importance of government will and involvement. Sociological Factors Religious beliefs, traditional value systems and cultures are important factors influencing organ transplantation and organ donation. In many cultures there is a strong belief that the sanctity of the deceased is paramount and any form of mutilation must be avoided. Among Muslims, who form a sizeable proportion of the developing world population, living donation and deceased donation are allowed provided unconditional consent is given, a view especially prevalent in the Middle East. The Saudis have been at the forefront of developing active cadaveric programs, enacting laws to support these. Reasons for the ongoing skepticism include belief that the human body is only entrusted to man and may not be interfered with, and ongoing controversy with regard to the concept and definition of brainstem death. Hinduism, with a following of some 1 billion people, is the predominant faith in South Asia. In contrast to the Abrahamic religions, the physical integrity of the body is not crucial to the reincarnation of the soul. It is therefore not surprising that the World Council of Hindus stated, "Organ donation is an integral part of our living. Buddhism, practiced in much of Asia, especially Thailand, Cambodia, Singapore, and Vietnam, is also characterized by rebirth and belief that the integrity of the physical body is not essential, although there is ambivalence surrounding the concept of brain death. Some Buddhist scholars frown upon deceased donor transplantation while others leave the choice to the individual. Traditional Chinese religious beliefs are strongly influenced by Confucianism and Taoism, both of which favor organ donation. Shintoism is the predominant belief system in Japan and teaches that the body is impure after death and interfering with the corpse brings bad luck. Although the Japanese law changed in 1997 to allow transplantation from deceased donors, 90% of all kidney transplants in Japan are from living donors. Today, the number of Japanese who carry organ donor cards remains among the lowest in the world. A concerted education campaign is required to increase public awareness of the need for organ donation to change negative public attitudes that hinder discussion of this subject by family members. The concept of brain death continues to be a source of controversy in some Muslim countries, with the result that legislation does not exist or is poorly implemented in Egypt, Morocco, Syria, Sudan, and Libya. The Human Organ Transplant Act was amended in 2004 to include death from all causes and extended to include organs other than kidneys. Pakistan, the center of illegal trade in organs, passed the Transplantation of Human Organs and Human Tissue Ordinance of 2007 into law in March 2010, after considerable international and national pressure.
Buy generic fluticasone 500 mcg
Postoperative pain control can be managed with epidural or patientcontrolled analgesia asthma treatment yahoo cheap 500mcg fluticasone with visa. Circulating plateletderived microparticles with procoagulant activity may be a potential cause of thrombosis in uremic patients. Insidious intoxication after morphine treatment in renal failure: delayed onset of morphine-6glucuronide action. Cardiac pathology in patients with end-stage renal disease maintained on hemodialysis. C-reactive protein, cardiac troponin T and low albumin are predictors of mortality in hemodialysis patients. Plasma protein binding of fentanyl: the effect of hyperlipidaemia and chronic renal failure. Plasma protein binding of etomidate in patients with renal failure or hepatic cirrhosis. Dopamine lowers the incidence of delayed graft function in transplanted kidney patients treated with cyclosporine A. Pharmacokinetics and pharmacodynamics of thiopental in patients undergoing renal transplantation. Renal function and serum fluoride concentrations in patients with stable renal insufficiency after anesthesia with sevoflurane or enflurane. Time course of neuromuscular effects and pharmacokinetics of rocuronium bromide (Org 9426) during isoflurane anaesthesia in patients with and without renal failure. End-stage renal failure reduces central clearance and prolongs the elimination of half-life of remifentanil. Pharmacokinetics and pharmacodynamics of atracurium during isoflurane anesthesia in normal and anephric patients. Diagnosis and management of coronary artery disease in patients with end-stage renal disease on hemodialysis. Pharmacokinetics of 1R-cis 1R-cis atracurium besylate (51 W89) and plasma laudanosine concentrations in health and chronic renal failure. Absence of biochemical evidence for renal and hepatic dysfunction after 8 hours of 1. Patient survival after kidney transplantation: relationship to pretransplant cardiac troponin T levels. Pharmacokinetics and pharmacodynamics of remifentanil in persons with renal failure compared with healthy volunteers. Peri-operative cardiac morbidity in kidney transplant recipients: incidence and risk factors. Propofol infusion for induction and maintenance of anaesthesia in patients with endstage renal disease. Pharmacokinetics of propofol and haemodynamic changes during induction of anaesthesia in uraemic patients. Comparison of propofol/ alfentanil anaesthesia with isoflurane/N2O/fentanyl anaesthesia for renal transplantation. Readmission to an intensive care unit following liver and kidney transplantation: a 50-month study. Risk factors for delayed graft function in cadaveric kidney transplantation: a prospective study of renal function and graft survival after preservation with University of Wisconsin solution in multi-organ donors. Cardiovascular risk factors of sirolimus compared with cyclosporine: early experience from two randomized trials in renal transplantation. Cardiovascular risk assessment among potential kidney transplant candidates: approaches and controversies. Exercise in hemodialysis patients after treatment with recombinant human erythropoietin. Pharmacokinetics of pancuronium in patients with normal and impaired renal function. Prognostic value of dipyridamole thallium-201 screening to minimize perioperative cardiac complications in diabetics undergoing kidney or kidneypancreas transplantation. Perioperative anticoagulation and antiplatelet therapy in renal transplant: is there an increase in bleeding complication? Treatment of the anemia of progressive renal failure with recombinant human erythropoietin. The pharmacokinetics and pharmacodynamics of atracurium in patients with and without renal failure. Clinical and echocardiographic disease in patients starting end-stage renal disease therapy. Renal concentrating function with prolonged sevoflurane or enflurane anesthesia in volunteers. Sevoflurane degradation product concentrations with soda lime during prolonged anesthesia. Death in the first year after kidney transplantation: implications for patients on the transplant waiting list. Evaluation of induction doses of propofol: comparison between endstage renal disease and normal renal function patients. Cardiac events in patients undergoing noncardiac surgery: shifting the paradigm from noninvasive risk stratification to therapy. Dopamine treatment of human cadaver kidney graft recipients: a prospectively randomized trial. The effect of different crystalloid solutions on acidase balance and early kidney function after kidney transplantation. Pharmacokinetics and pharmacodynamics of the three isomers of mivacurium in health, in end-stage renal failure and in patients with impaired renal function. Laser Doppler blood flow measurement as a predictor of viability of renal allografts. Anaesthesiological complications in renal transplantation: a retrospective study of 500 transplantations. Comparison of a continuous glucose-insulin-potassium infusion versus intermittent bolus application of insulin on perioperative glucose control and hormone status in insulin-treated type 2 diabetics. Dobutamine stress echocardiography for the detection of significant coronary artery disease in renal transplant candidates. Changes in renal blood flow in response to sympathomimetics in the rat transplanted and denervated kidney. Improvement of left ventricular function and arterial blood pressure 1 year after simultaneous pancreas kidney transplantation. The impact of timing of maximal crystalloid hydration on early graft function during kidney transplantation. The effect of repeated doses of succinylcholine on serum potassium in patients with renal failure. Defective high-density lipoprotein composition in patients on chronic hemodialysis. Predictability of difficult laryngoscopy in patients with long-term diabetes mellitus. Increased volume of gastric contents in diabetic patients undergoing renal transplantation: lack of effect with cisapride. Pharmacokinetics and pharmacodynamics of rocuronium in patients with and without renal failure. Increased sensitivity to vecuronium and prolonged duration of its action in patients with end-stage renal failure. Determinants of coronary artery calcification progression in renal transplant recipients. Informational contribution of noninvasive screening tests for coronary artery disease in patients on chronic renal replacement therapy. Dyspepsia and gastroparesis in chronic renal failure: the role of Helicobacter pylori. Sufentanil disposition in patients undergoing renal transplantation: influence of choice of kinetic model. Studies on morphine disposition: influence of renal failure on the kinetics of morphine and its metabolites. Does the choice of antihypertensive therapy influence haemodynamic responses to induction, laryngoscopy and intubation? Optimal medical therapy with or without percutaneous coronary intervention for patients with stable coronary artery disease and chronic kidney disease.
Generic 500 mcg fluticasone mastercard
Outcome of subclinical antibody-mediated rejection in kidney transplant recipients with preformed donor-specific alloantibody asthmatic bronchitis emedicine cheap fluticasone 250mcg free shipping. Clinical results from transplanting incompatible live donor kidney donor/recipient pairs using kidney paired donation. Proteasome inhibitor-based primary therapy for antibody-mediated renal allograft rejection. Transplant glomerulopathy: ultrastructural abnormalities occur early in longitudinal analyses of protocol biopsies. This requires a coordinated effort to collect data about incompatible pairs and about other types of participants such as nondirected (altruistic) donors and compatible pairs, and to select appropriate matches28 by a manual or algorithmic process. This also requires that all donors who are part of the arrangement donate simultaneously, to avoid a situation where an individual donates but the intended recipient does not receive a transplant because another donor decides against donation. By 2003, paired donations comprised more than 10% of living kidney donations at one Korean center. There is no obvious party responsible for paying the expenses incurred in donor evaluations for incompatible donors, some of whom never donate, nor for the tissue typing and administrative costs of maintaining a paired donation registry to locate suitable matches. This donor might donate immediately to a candidate on the deceased donor waiting list, creating a closed chain (domino paired donation). Alternatively, the last donor might wait (for a few months or longer) as a bridge donor, subsequently donating to another incompatible pair to begin another sequence of donations (open chain, or non-simultaneous extended altruistic donor chain). Non-directed donors are particularly valuable in paired donation because non-directed donors are not paired with one particular candidate who must receive a kidney, easing the reciprocal compatibility requirement. Furthermore, a renege will not directly harm a pair (because no individual donates without his or her paired recipient receiving a transplant), even though a renege will cause the chain to break and, therefore, the final patient on the deceased donor waiting list (the one who would have closed the chain) does not receive a transplant. In the Netherlands, non-directed donors are only matched to incompatible pairs after the pairs have tried to find a traditional kidney exchange with other pairs. Also, nondirected donors in the Netherlands are allocated on a center basis rather than by the national program. In practice, all functioning registries in the United States that use chains "close" them when those involved feel that the bridge donor has either waited too long or will inevitably wait for a long period of time. At the most basic level, every donor should be blood group and tissue typecompatible with the candidate to whom he or she will donate. These centers may wish to combine desensitization with kidney exchange in order to obtain transplants for their hardest-to-match patients. For a fixed pool of participants in a paired donation registry, "matching" means selecting a non-overlapping set of matches to proceed to transplant. Some seemingly effective matching heuristics neglect the interconnectedness of these decisions. For instance, it is not optimal to 25 Kidney Paired donation Programs for Living donors 375 rank all possible matches and then choose the highestranked match first, the next highest-ranked available match second, and so on. This match rank heuristic, which has been used in some operational registries,15 might transplant fewer people than would be possible with better matching algorithms. There are only two correct approaches to find the best set of matches among a specific list of participants: exhaustive search or integer programming (optimization). In exhaustive search, a computer generates every possible set of matches and then compares them to select the best set of matches, as in the Korean registry. Integer programming models, including some algorithms specialized for the paired donation problem,1 use mathematical techniques to locate and verify the best set of matches without having to describe all possible sets of matches explicitly. Media attention to this modality, and greater physician familiarity with its variations, will be positive forces in expanding access to paired donation. We believe innovations in this field will allow more candidates with incompatible donors to benefit from kidney transplantation. Clearing algorithms for barter exchange markets: enabling nationwide kidney exchanges. Donor exchange programs in kidney transplantation: rationale and operational details from the north central donor exchange cooperative. Dynamic challenges inhibiting optimal adoption of kidney paired donation: findings of a consensus conference. A comparison of populations served by kidney paired donation and list paired donation. Cross-over kidney transplantation with simultaneous laparoscopic living donor nephrectomy: initial experience. Starting a crossover kidney transplantation program in the Netherlands: ethical and psychological considerations. Five years of single-center experience with paired kidney exchange transplantation. All candidates benefit from increasing pool size, but the benefit is particularly pronounced for sensitized candidates. For instance, a nationwide registry in the United States would create a sixfold increase in kidney exchange opportunities for sensitized candidates. Because fewer incompatible pairs and many fewer sensitized candidates will find matches if participants are divided into smaller pools than if the participants were in one larger pool, the proliferation of multiple registries is of concern, as discussed in a recent national consensus conference. Altruistic donor triggered domino-paired kidney donation for unsuccessful couples from the kidney-exchange program. Increasing the opportunity of live kidney donation by matching for two and three way exchanges. Transporting live donor kidneys for kidney paired donation: initial national results. Cold ischemia time and allograft outcomes in live donor renal transplantation: is live donor organ transport feasible? Successful threeway kidney paired donation with cross-country live donor allograft transport. Clinical results from transplanting incompatible live kidney donor/ recipient pairs using kidney paired donation. Finally, the biopsy serves, in turn, to validate the hypothesis tested in 377 378 Kidney transPlantation: PrinciPles and Practice such trials. Renal biopsy interpretation currently relies primarily on histopathology complemented by immunological molecular probes, and perhaps in the future, with quantitative gene expression. The discussion is broadly divided into allograft rejection and non-rejection pathology, with an emphasis on differential diagnosis of acute and chronic allograft dysfunction. Grading systems of acute and chronic rejection are discussed further in those sections. Classification of Pathologic Diagnoses in the Renal Allograft the ideal diagnostic classification of renal allograft pathology should be based on pathogenesis, have therapeutic relevance, and be reproducible. The current classification, based on Banff and other systems (Table 26-1), meets these criteria. Optimal Tissue At least seven non-sclerotic glomeruli and two arteries (bigger than arterioles) are recommended for adequate evaluation. In contrast, a large portion of cortex with a minimal infiltrate does not exclude rejection. Subcapsular cortex often shows inflammation and fibrosis and is not representative. Microscopy the biopsy is examined for glomerular, tubular, vascular, and interstitial pathology, including: (1) transplant glomerulitis, glomerulopathy, and de novo or recurrent glomerulonephritis; (2) tubular injury, isometric vacuolization, tubulitis, atrophy, or intranuclear viral inclusions; (3) endarteritis, fibrinoid necrosis, thrombi, myocyte necrosis, nodular medial hyalinosis, or chronic allograft arteriopathy; (4) interstitial infiltrates of activated mononuclear cells, edema, or neutrophils, fibrosis, and scarring. Our standard immunofluorescence panel detects IgG, IgA, IgM, C3, C4d, albumin, and fibrin in cryostat sections. Objective pathologic criteria based on outcome that could be applied to the renal biopsy as a screening test have not been established, as donor biopsies are not routinely performed and controlled trials have not been done. One of the major problems in assessing the donor kidney is that this is usually done with cryostat sections, often by nonrenal pathologists in the middle of the night. Even though many other studies try to correlate fibrosis or vascular disease, reproducibility of scoring these lesions, even on permanent sections by expert renal pathologists in broad daylight, is notoriously poor. In two large studies, the outcome at 1͵ years was not measurably correlated with pathological lesions. Glomerulosclerosis can be readily assessed in frozen section, by the most casual observers, and has been a popular parameter for judging the quality of the donor kidney. Glomerulosclerosis >20% correlates with poor graft outcome in some, but not all, studies. Other lesions may cause the transplant surgeon or pathologist to argue against use of the graft. Mathematically combined scores of pathological lesions have been proposed as a guide,314 including, most recently, the Maryland Aggregate Pathology Index. Further, whether this will provide an efficient separation of beneficial organs will depend on prospective validation studies.
