
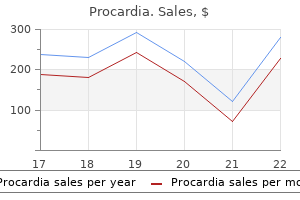
Cheap procardia 30mg without prescription
It results from facilitation of the synaptic pathways cardiovascular disease uae cheap 30 mg procardia mastercard, and the process is called memory sensitization. As we discuss later, special areas in the basal limbic regions of the brain determine whether information is important or unimportant and make the subconscious decision about whether to store the thought as a sensitized memory trace or to suppress it. We know that some memories last for only a few seconds, whereas others last for hours, days, months, or years. For the purpose of discussing these types of memories, let us use a common classification that divides memories into (1) short-term memory, which includes memories that last for seconds or at most minutes unless they are converted into longerterm memories; (2) intermediate long-term memories, which last for days to weeks but then fade away; and (3) long-term memory, which, once stored, can be recalled up to years or even a lifetime later. In addition to this general classification of memories, we also discussed earlier (in connection with the prefrontal lobes) another type of memory, called "working memory," which includes mainly short-term memory that is used during the course of intellectual reasoning but is terminated as each stage of the problem is resolved. Memories are frequently classified according to the type of information that is stored. One of these classifications divides memory into declarative memory and skill memory, as follows: 1. They are important because once the traces are established they can be selectively activated by the thinking mind to reproduce the memories. Experiments in lower animals have demonstrated that memory traces can occur at all levels of the nervous system. Even spinal cord reflexes can change at least slightly in response to repetitive cord activation, and these reflex changes are part of the memory process. Also, longterm memories result from changed synaptic conduction in lower brain centers. However, most memory that we associate with intellectual processes is based on memory traces in the cerebral cortex. Positive and Negative Memory-"Sensitization" or "Habituation" of Synaptic Transmission. Although we often think of memories as being positive recollections of previous thoughts or experiences, probably the greater share of our memories is negative, not positive. If our minds attempted to remember all this information, the memory capacity of the brain would be rapidly exceeded. Fortunately, the brain has the capability to ignore information that is of no consequence. This capability results from inhibition of the synaptic pathways for this type of information; the resulting effect is called habituation, which is a type of negative memory. Another possible explanation of short-term memory is presynaptic facilitation or inhibition, which occurs at synapses that lie on terminal nerve fibrils immediately before these fibrils synapse with a subsequent neuron. The neurotransmitter chemicals secreted at such terminals frequently cause facilitation or inhibition lasting for seconds up to several minutes. They will eventually be lost unless the memory traces are activated enough to become more permanent; then they are classified as long-term memories. Experiments in primitive animals have demonstrated that memories of the intermediate long-term type can result from temporary chemical or physical changes, or both, in either the synapse presynaptic terminals or the synapse postsynaptic membrane, changes that can persist for a few minutes up to several weeks. When the sensory terminal is stimulated repeatedly but without stimulation of the facilitator terminal, signal transmission at first is great, but it becomes less and less intense with repeated stimulation until transmission almost ceases. It is a type of negative memory that causes the neuronal circuit to lose its response to repeated events that are insignificant. Conversely, if a noxious stimulus excites the facilitator terminal at the same time that the sensory terminal is stimulated, instead of the transmitted signal into the postsynaptic neuron becoming progressively weaker, the ease of transmission becomes stronger and stronger, and it will remain strong for minutes, hours, days, or, with more intense training, up to about 3 weeks even without further stimulation of the facilitator terminal. Thus, the noxious stimulus causes the memory pathway through the sensory terminal to become facilitated for days or weeks thereafter. It is especially interesting that even after habituation has occurred, this pathway can be converted back to a facilitated pathway with only a few noxious stimuli. One terminal, which is from a sensory input neuron, terminates directly on the surface of the neuron that is to be stimulated and is called the sensory terminal. Nevertheless, much smaller than normal amounts of calcium ions can diffuse into the habituated terminal, and much less sensory terminal transmitter is therefore released because calcium entry is the principal stimulus for transmitter release (as was discussed in Chapter 46). In the case of facilitation, at least part of the molecular mechanism is believed to be the following: 1. Stimulation of the facilitator presynaptic terminal at the same time that the sensory terminal is stimulated causes serotonin release at the facilitator synapse on the surface of the sensory terminal. The serotonin acts on serotonin receptors in the sensory terminal membrane, and these receptors activate the enzyme adenyl cyclase inside the membrane. Motor and Integrative Neurophysiology is necessary for rapid recovery from the action potential. The prolonged action potential causes prolonged activation of the calcium channels, allowing tremendous quantities of calcium ions to enter the sensory synaptic terminal. These calcium ions cause greatly increased transmitter release by the synapse, thereby markedly facilitating synaptic transmission to the subsequent neuron. Thus, in a very indirect way, the associative effect of stimulating the facilitator terminal at the same time that the sensory terminal is stimulated causes prolonged increase in excitatory sensitivity of the sensory terminal, which establishes the memory trace. Studies by Byrne and colleagues, also in the snail Aplysia, have suggested still another mechanism of synaptic memory. Their studies have shown that stimuli from separate sources acting on a single neuron, under appropriate conditions, can cause long-term changes in membrane properties of the postsynaptic neuron instead of in the presynaptic neuronal membrane, but leading to essentially the same memory effects. Changes in structures of the dendritic spines that permit transmission of stronger signals Thus, in several different ways, the structural capability of synapses to transmit signals appears to increase during establishment of true long-term memory traces. Number of Neurons and Their Connectivities Often Change Significantly During Learning During the first few weeks, months, and perhaps even year or so of life, many parts of the brain produce a great excess of neurons, and the neurons send out numerous axon branches to make connections with other neurons. If the new axons fail to connect with appropriate neurons, muscle cells, or gland cells, the new axons will dissolute within a few weeks. Thus, the number of neuronal connections is determined by specific nerve growth factors released retrogradely from the stimulated cells. Furthermore, when insufficient connectivity occurs, the entire neuron that is sending out the axon branches might eventually disappear. Therefore, soon after birth, the principle of "use it or lose it" governs the final number of neurons and their connectivities in respective parts of the human nervous system. For example, if one eye of a newborn animal is covered for many weeks after birth, neurons in alternate stripes of the cerebral visual cortex-neurons normally connected to the covered eye-will degenerate, and the covered eye will remain either partially or totally blind for the remainder of life. Until recently, it was believed that very little "learning" is achieved in adult human beings and animals by modification of numbers of neurons in the memory circuits; however, recent research suggests that even adults use this mechanism at least to some extent. However, long-term memory is generally believed to result from actual structural changes, instead of only chemical changes, at the synapses, and these changes enhance or suppress signal conduction. Again, let us recall experiments in primitive animals (where the nervous systems are much easier to study) that have aided immensely in understanding possible mechanisms of long-term memory. Structural Changes Occur in Synapses During Development of Long-Term Memory Electron microscopic pictures taken from invertebrate animals have demonstrated multiple physical structural changes in many synapses during development of longterm memory traces. The structural changes will not occur if a drug is given that blocks protein synthesis in the presynaptic neuron, nor will the permanent memory trace develop. Therefore, it appears that development of true long-term memory depends on physically restructuring the synapses themselves in a way that changes their sensitivity for transmitting nervous signals. This process requires 5 to 10 minutes for minimal consolidation and 1 hour or more for strong consolidation. For instance, if a strong sensory impression is made on the brain but is then followed within a minute or so by an electrically induced brain convulsion, the sensory experience will not be remembered. Likewise, brain concussion, sudden application of deep general anesthesia, or any other effect that temporarily blocks the dynamic function of the brain can prevent consolidation. Consolidation and the time required for it to occur can probably be explained by the phenomenon of rehearsal of the short-term memory, as described in the following section. Therefore, over a period of time, the important features of sensory experiences become progressively more and more fixed in the memory stores. This phenomenon explains why a person can remember small amounts of information studied in depth far better than large amounts of information studied only superficially. It also explains why a person who is wide awake can consolidate memories far better than a person who is in a state of mental fatigue. Studies have shown output pathways from the "reward" and "punishment" areas of the limbic system, as explained in Chapter 59. Sensory stimuli or thoughts that cause pain or aversion excite the limbic punishment centers, and stimuli that cause pleasure, happiness, or sense of reward excite the limbic reward centers. Among these motivations is the drive in the brain to remember those experiences and thoughts that are either pleasant or unpleasant. The hippocampi especially and to a lesser degree the dorsal medial nuclei of the thalamus, another limbic structure, have proved especially important in making the decision about which of our thoughts are important enough on a basis of reward or punishment to be worthy of memory.
Buy generic procardia pills
The mechanism of color contrast analysis depends on the fact that contrasting colors your capillaries purchase procardia with amex, called "opponent colors," excite specific neuronal cells. It is presumed that the initial details of color contrast are detected by simple cells, whereas more complex contrasts are detected by complex and hypercomplex cells. Effect of Removing the Primary Visual Cortex Removal of the primary visual cortex in the human being causes loss of conscious vision-that is, blindness. However, psychological studies demonstrate that such "blind" people can still, at times, react subconsciously to changes in light intensity, to movement in the visual scene, or, rarely, even to some gross patterns of vision. This vision is believed to be subserved by neuronal pathways that pass from the optic tracts mainly into the superior colliculi and other portions of the older visual system. Fields of Vision; Perimetry the field of vision is the visual area seen by an eye at a given instant. The area seen to the nasal side is called the nasal field of vision, and the area seen to the lateral side is called the temporal field of vision. To diagnose blindness in specific portions of the retina, one charts the field of vision for each eye by a process called perimetry. This charting is performed by having the subject look with one eye toward a central spot directly in front of the eye; the other eye is closed. In all perimetry charts, a blind spot caused by lack of rods and cones in the retina over the optic disc is found about 15 degrees lateral to the central point of vision, as shown in the figure. Occasionally, blind spots are found in portions of the field of vision other than the optic disc area. Such blind spots, called scotomata, are frequently caused by damage to the optic nerve resulting from glaucoma (too much fluid pressure in the eyeball), allergic reactions in the retina, or toxic conditions such as lead poisoning or excessive use of tobacco. In this disease, portions of the retina degenerate, and excessive melanin pigment is deposited in the degenerated areas. Retinitis pigmentosa usually causes blindness in the peripheral field of vision first and then gradually encroaches on the central areas. Destruction of the optic chiasm prevents the crossing of impulses from the nasal half of each retina to the opposite optic tract. Therefore, the nasal half of each retina is blinded, which means that the person is blind in the temporal field of vision for each eye because the image of the field of vision is inverted on the retina by the optical system of the eye; this condition is called bitemporal hemianopsia. Such lesions frequently result from tumors of the pituitary gland pressing upward from the sella turcica on the bottom of the optic chiasm. Interruption of an optic tract denervates the corresponding half of each retina on the same side as the lesion; as a result, neither eye can see objects to the opposite side of the head. The oblique muscles function mainly to rotate the eyeballs to keep the visual fields in the upright position. From both the pretectal Superior rectus Superior oblique Lateral rectus Medial rectus Nuclei N. Also shown are interconnections among the brain stem nuclei by way of the nerve tract called the medial longitudinal fasciculus. Each of the three sets of muscles to each eye is reciprocally innervated so that one muscle of the pair relaxes while the other contracts. The first of these mechanisms allows a person to move the eyes voluntarily to find the object on which he or she wants to fix the vision, which is called the voluntary fixation mechanism. The second is an involuntary mechanism, called the involuntary fixation mechanism, that holds the eyes firmly on the object once it has been found. Bilateral dysfunction or destruction of these areas makes it difficult for a person to "unlock" the eyes from one point of fixation and move them to another point. It is usually necessary to blink the eyes or put a hand over the eyes for a short time, which then allows the eyes to be moved. Conversely, the fixation mechanism that causes the eyes to "lock" on the object of attention once it is found is controlled by secondary visual areas in the occipital cortex, located mainly anterior to the primary visual cortex. When this fixation area is destroyed bilaterally in an animal, the animal has difficulty keeping its eyes directed toward a given fixation point or may become totally unable to do so. To summarize, posterior "involuntary" occipital cortical eye fields automatically "lock" the eyes on a given spot of the visual field and thereby prevent movement of the image across the retinas. To unlock this visual fixation, voluntary signals must be transmitted from cortical "voluntary" eye fields located in the frontal cortices. Each time the spot drifts as far as the edge of the fovea, a sudden reflex reaction occurs, producing a flicking movement that moves the spot away from this edge back toward the center of the fovea. Thus, an automatic response moves the image back toward the central point of vision. The dashed lines show the slow drifting across the fovea, and the solid lines show the flicks that keep the image from leaving the foveal region. This involuntary fixation capability is mostly lost when the superior colliculi are destroyed. When a visual scene is fixation discussed in the previous section results from a negative feedback mechanism that prevents the object of attention from leaving the foveal portion of the retina. The eyes normally have three types of continuous but almost imperceptible movements: (1) a continuous tremor at a rate of 30 to 80 cycles/sec caused by successive contractions of the motor units in the ocular muscles; (2) a slow drift of the eyeballs in one direction or another; and (3) sudden flicking movements that are controlled by the involuntary fixation mechanism. When a spot of light becomes fixed on the foveal region of the retina, the tremulous movements cause the moving continually before the eyes, such as when a person is riding in a car, the eyes fix on one highlight after another in the visual field, jumping from one to the next at a rate of two to three jumps per second. The jumps are called saccades, and the movements are called opticokinetic movements. The saccades occur so rapidly that no more than 10 percent of the total time is spent moving the eyes, with 90 percent of the time being allocated to the fixation sites. Also, the brain suppresses the visual image during saccades, so the person is not conscious of the movements from point to point. During the process of reading, a person usually makes several saccadic movements of the eyes for each line. In this case, the visual scene is not moving past the eyes, but the eyes are trained to move by means of several successive saccades across the visual scene to extract the important information. The Special Senses observes a painting, except that the saccades occur in upward, sideways, downward, and angulated directions one after another from one highlight of the painting to another, and so forth. It was pointed out earlier in the chapter that corresponding points of the two retinas transmit visual signals to different neuronal layers of the lateral geniculate body, and these signals in turn are relayed to parallel neurons in the visual cortex. Interactions occur between these cortical neurons to cause interference excitation in specific neurons when the two visual images are not "in register"-that is, are not precisely "fused. Once the corresponding points of the two retinas are in register, excitation of the specific "interference" neurons in the visual cortex disappears. The eyes can also remain fixed on a moving object, which is called pursuit movement. A highly developed cortical mechanism automatically detects the course of movement of an object and then rapidly develops a similar course of movement for the eyes. For instance, if an object is moving up and down in a wavelike form at a rate of several times per second, the eyes at first may be unable to fixate on it. However, after a second or so, the eyes begin to jump by means of saccades in approximately the same wavelike pattern of movement as that of the object. Then, after another few seconds, the eyes develop progressively smoother movements and finally follow the wave movement almost exactly. This represents a high degree of automatic subconscious computational ability by the pursuit system for controlling eye movements. Superior Colliculi Are Mainly Responsible for Turning the Eyes and Head Toward a Visual Disturbance. Neural Mechanism of Stereopsis for Judging Distances of Visual Objects Because the two eyes are more than 2 inches apart, the images on the two retinas are not exactly the same. That is, the right eye sees a little more of the right-hand side of the object, and the left eye sees a little more of the lefthand side; the closer the object, the greater the disparity. Therefore, even when the two eyes are fused with each other, it is still impossible for all corresponding points in the two visual images to be exactly in register at the same time. Furthermore, the nearer the object is to the eyes, the less the degree of register. This degree of nonregister provides the neural mechanism for stereopsis, an important mechanism for judging the distances of visual objects up to about 200 feet (60 meters). The neuronal cellular mechanism for stereopsis is based on the fact that some of the fiber pathways from the retinas to the visual cortex stray 1 to 2 degrees on each side of the central pathway.
Syndromes
- Blood tests such as thyroid function tests, complete blood count, iron count and pregnancy test
- Eating too fast, failing to chew food well enough, or eating with improperly fitted dentures
- End-stage kidney disease
- Kidney failure
- Radiation therapy
- Parasites
- Medications to treat symptoms
- Serum immunoelectrophoresis
- Osteonecrosis (avascular necrosis)
- In organs, tissues, and cells
Purchase 30mg procardia mastercard
If the condition occurs before adolescence blood vessels brain 3d purchase procardia 30 mg mastercard, before the epiphyses of the long bones have become fused with the shafts, height increases so that the person becomes a giant-up to 8 feet tall. The giant ordinarily has hyperglycemia, and the beta cells of the islets of Langerhans in the pancreas are prone to degenerate because they become overactive owing to the hyperglycemia. Consequently, in about 10 percent of giants, full-blown diabetes mellitus eventually develops. In most giants, panhypopituitarism eventually develops if they remain untreated because the gigantism is usually caused by a tumor of the pituitary gland that grows until the gland is destroyed. This eventual general deficiency of pituitary hormones usually causes death in early adulthood. However, once gigantism is diagnosed, further effects can often be blocked by microsurgical removal of the tumor or by irradiation of the pituitary gland. If an acidophilic tumor occurs after adolescence-that is, after the epiphyses of the long bones have fused with the shafts-the person cannot grow taller, but the bones can become thicker and the soft tissues can continue to grow. Enlargement is especially marked in the bones of the hands and feet and in the membranous bones, including the cranium, nose, bosses on the forehead, supraorbital ridges, lower jawbone, and portions of the vertebrae, because their growth does not cease at adolescence. Consequently, the lower jaw protrudes forward, sometimes as much as half an inch, the forehead slants forward because of excess development of the supraorbital ridges, the nose increases to as much as twice normal size, the feet require size 14 or larger shoes, and the fingers become extremely thickened so that the hands are almost twice normal size. In addition to these effects, changes in the vertebrae ordinarily cause a hunched back, which is known clinically as kyphosis. Finally, many soft tissue organs, such as the tongue, the liver, and especially the kidneys, become greatly enlarged. Possible Role of Decreased Growth Hormone Secretion in Causing Changes Associated with Aging In people who have lost the ability to secrete growth hormone, some features of the aging process accelerate. For instance, a 50-year-old person who has been without growth hormone for many years may have the appearance of a person aged 65 years. The aged appearance seems to result mainly from decreased protein deposition in most tissues of the body and increased fat deposition in its place. The physical and physiological effects are increased wrinkling of the skin, diminished rates of function of some of the organs, and diminished muscle mass and strength. As one ages, the average plasma concentration of growth hormone in an otherwise normal person changes approximately as follows: Age (years) 5to20 20to40 40to70 ng/ml 6 3 1. In fact, some studies of growth hormone therapy in older people have demonstrated three important beneficial effects: (1) increased protein deposition in the body, especially in the muscles; (2) decreased fat deposits; and (3) a feeling of increased energy. Other studies, however, have shown that treatment of elderly patients with recombinant growth hormone may produce several undesirable adverse effects including insulin resistance and diabetes, edema, carpal tunnel syndrome, and arthralgias (joint pain). Therefore, recombinant growth hormone therapy is generally not recommended for use in healthy elderly patients with normal endocrine function. These tracts pass to the neurohypophysis through the pituitary stalk (hypophysial stalk). If the pituitary stalk is cut above the pituitary gland but the entire hypothalamus is left intact, the posterior pituitary hormones continue to be secreted normally, after a transient decrease for a few days; they are then secreted by the cut ends of the fibers within the hypothalamus and not by the nerve endings in the posterior pituitary. Each of these nuclei can synthesize about one sixth as much of the second hormone as of its primary hormone. When nerve impulses are transmitted downward along the fibers from the supraoptic or paraventricular nuclei, the hormone is immediately released from the secretory granules in the nerve endings by the usual secretory mechanism of exocytosis and is absorbed into adjacent capillaries. Both the neurophysin and the hormone are secreted together, but because they are only loosely bound to each other, the hormone separates almost immediately. This formation causes phosphorylation of elements in the special vesicles, which then causes the vesicles to insert into the apical cell membranes, thus providing many areas of high water permeability. Thus, this process temporarily provides many new pores that allow free diffusion of water from the tubular fluid through the tubular epithelial cells and into the renal interstitial fluid. Water is then absorbed from the collecting tubules and ducts by osmosis, as explained in Chapter 29 in relation to the urine-concentrating mechanism of the kidneys. However, immediately inside the cell membrane are a large number of special vesicles that have highly water-permeable pores called aquaporins. Somewhere in or near the hypothalamus are modified neuron receptors called osmoreceptors. Although some researchers place these osmoreceptors in the hypothalamus (possibly even in the supraoptic nuclei), others believe that they are located in the organum vasculosum, a highly vascular structure in the anteroventral wall of the third ventricle. Regardless of the mechanism, concentrated body fluids stimulate the supraoptic nuclei, whereas dilute body fluids inhibit them. A feedback control system is available to control the total osmotic pressure of the body fluids. This occurs strongly when the blood volume decreases 15 to 25 percent or more; the secretory rate then sometimes rises to as high as 50 times normal. For further details about this blood volume-pressure feedback mechanism, refer to Chapter 29. The hormone oxytocin, in accordance with its name, powerfully stimulates contraction of the pregnant uterus, especially toward the end of gestation. Therefore, many obstetricians believe that this hormone is at least partially responsible for causing birth of the baby. This belief is supported by the following facts: (1) In a hypophysectomized animal, the duration of labor is prolonged, indicating a possible effect of oxytocin during delivery; (2) the amount of oxytocin in the plasma increases during labor, especially during the last stage; and (3) stimulation of the cervix in a pregnant animal elicits nervous signals that pass to the hypothalamus and cause increased secretion of oxytocin. These effects and this possible mechanism for aiding in the birth process are discussed in more detail in Chapter 83. Oxy- tocin also plays an especially important role in lactation- a role that is far better understood than its role in delivery. In lactation, oxytocin causes milk to be expressed from the alveoli into the ducts of the breast so that the baby can obtain it by suckling. This mechanism works as follows: the suckling stimulus on the nipple of the breast causes signals to be transmitted through sensory nerves to the oxytocin neurons in the paraventricular and supraoptic nuclei in the hypothalamus, which causes release of oxytocin by the posterior pituitary gland. The thyroid secretes two major hormones, thyroxine and triiodothyronine, commonly called T4 and T3, respectively. Complete lack of thyroid secretion usually causes the basal metabolic rate to fall 40 to 50 percent below normal, and extreme excesses of thyroid secretion can increase the basal metabolic rate to 60 to 100 percent above normal. The thyroid gland also secretes calcitonin, a hormone involved in calcium metabolism that is discussed in Chapter 80. The purpose of this chapter is to discuss the formation and secretion of the thyroid hormones, their metabolic functions, and regulation of their secretion. Once the secretion has entered the follicles, it must be absorbed back through the follicular epithelium into the blood before it can function in the body. The thyroid gland has a blood flow about five times the weight of the gland each minute, which is a blood supply as great as that of any other area of the body, with the possible exception of the adrenal cortex. The thyroid gland also contains C cells that secrete calcitonin, a hormone that contributes to regulation of plasma calcium ion concentration, as discussed in Chapter 80. To prevent iodine deficiency, common table salt is iodized with about 1 part sodium iodide to every 100,000 parts sodium chloride. However, almost all the thyroxine is eventually converted to triiodothyronine in the tissues, so both are functionally important. The functions of these two hormones are qualitatively the same, but they differ in rapidity and intensity of action. Triiodothyronine is about four times as potent as thyroxine, but it is present in the blood in much smaller quantities and persists for a much shorter time compared with thyroxine. Normally, most of the iodides are rapidly excreted by the kidneys, but only after about one fifth are selectively removed from the circulating blood by the cells of the thyroid gland and used for synthesis of the thyroid hormones. The basal membrane of the thyroid cell has the specific ability to pump the iodide actively to the interior of the cell. This pumping is achieved by the action of a sodium-iodide symporter, which co-transports one iodide ion along with two sodium ions across the basolateral (plasma) membrane into the cell. In a normal gland, the iodide pump concentrates the iodide to about 30 times its concentration in the blood. When the thyroid gland becomes maximally active, this concentration ratio can rise to as high as 250 times.
Buy generic procardia 30 mg
For instance coronary artery occlusive disease procardia 30 mg online, pain in one of the visceral organs often is referred to an area on the body surface. Knowledge of the different types of referred pain is important in clinical diagnosis because in many visceral ailments the only clinical sign is referred pain. Pain,Headache,andThermalSensations stretching of the connective tissue surrounding or within the viscus. Essentially all visceral pain that originates in the thoracic and abdominal cavities is transmitted through small type C pain fibers and, therefore, can transmit only the chronic-aching-suffering type of pain. Ischemia causes visceral pain in the same way that it does in other tissues, presumably because of the formation of acidic metabolic end products or tissuedegenerative products such as bradykinin, proteolytic enzymes, or others that stimulate pain nerve endings. On occasion, damaging substances leak from the gastrointestinal tract into the peritoneal cavity. For instance, proteolytic acidic gastric juice may leak through a ruptured gastric or duodenal ulcer. This juice causes widespread digestion of the visceral peritoneum, thus stimulating broad areas of pain fibers. Spasm of a portion of the gut, the gallbladder, a bile duct, a ureter, or any other hollow viscus can cause pain, possibly by mechanical stimulation of the pain nerve endings. Often pain from a spastic viscus occurs in the form of cramps, with the pain increasing to a high degree of severity and then subsiding. For instance, each time a peristaltic wave travels along an overly excitable spastic gut, a cramp occurs. The cramping type of pain frequently occurs in persons with appendicitis, gastroenteritis, constipation, menstruation, parturition, gallbladder disease, or ureteral obstruction. Extreme overfilling of a hollow viscus also can result in pain, presumably because of overstretch of the tissues themselves. Overdistention can also collapse the blood vessels that encircle the viscus or that pass into its wall, thus perhaps promoting ischemic pain. Yet the liver capsule is extremely sensitive to both direct trauma and stretch, and the bile ducts are also sensitive to pain. In the lungs, even though the alveoli are insensitive, both the bronchi and the parietal pleura are very sensitive to pain. Second, sensations from the abdomen and thorax are transmitted through two pathways to the central nervous system: the true visceral pathway and the parietal pathway. True visceral pain is transmitted via pain sensory fibers within the autonomic nerve bundles, and the sensations are referred to surface areas of the body often far from the painful organ. Conversely, parietal sensations are conducted directly into local spinal nerves from the parietal peritoneum, pleura, or pericardium, and these sensations are usually localized directly over the painful area. These parietal surfaces, like the skin, are supplied with extensive pain innervation from the peripheral spinal nerves. An example can emphasize the difference between this pain and true visceral pain: a knife of the body, the person generally localizes it in the dermatomal segment from which the visceral organ originated in the embryo, not necessarily where the visceral organ now lies. These are the areas of the body surface that send their own somatosensory nerve fibers into the C3 to T5 cord segments. Most frequently, the pain is on the left side rather than on the right because the left side of the heart is much more frequently involved in coronary disease than is the right side. The stomach originated approximately from the seventh to ninth thoracic segments of the embryo. Therefore, stomach pain is referred to the anterior epigastrium above the umbilicus, which is the surface area of the body subserved by the seventh through ninth thoracic segments. Pain from the viscera is frequently local- ized to two surface areas of the body at the same time because of the dual transmission of pain through the referred visceral pathway and the direct parietal pathway. General Principles and Sensory Physiology Heart Esophagus Some Clinical Abnormalities of Pain and Other Somatic Sensations Hyperalgesia-Hypersensitivity to Pain A pain nervous pathway sometimes becomes excessively excitable, which gives rise to hyperalgesia. Possible causes of hyperalgesia are (1) excessive sensitivity of the pain receptors, which is called primary hyperalgesia, and (2) facilitation of sensory transmission, which is called secondary hyperalgesia. An example of primary hyperalgesia is the extreme sensitivity of sunburned skin, which results from sensitization of the skin pain endings by local tissue products from the burn-perhaps histamine, prostaglandins, and others. Secondary hyperalgesia frequently results from lesions in the spinal cord or the thalamus. This infection causes severe pain in the dermatomal segment subserved by the ganglion, thus eliciting a segmental type of pain that circles halfway around the body. The disease is called herpes zoster, or "shingles," because of a skin eruption that often ensues. The cause of the pain is presumably infection of the pain neuronal cells in the dorsal root ganglion by the virus. In addition to causing pain, the virus is carried by neuronal cytoplasmic flow outward through the neuronal peripheral axons to their cutaneous origins. Here the virus causes a rash that vesiculates within a few days and then crusts over within another few days, all of this occurring within the dermatomal area served by the infected dorsal root. Tic Douloureux Lancinating or stabbing type of pain occasionally occurs in some people over one side of the face in the sensory distribution area (or part of the area) of the fifth or ninth nerves; this phenomenon is called tic douloureux (or trigeminal neuralgia or glossopharyngeal neuralgia). The pain feels like sudden electrical shocks, and it may appear for only a few seconds at a time or may be almost continuous. Often it is set off by exceedingly sensitive trigger areas on the surface of the face, in the mouth, or inside the throat- almost always by a mechanoreceptive stimulus rather than a pain stimulus. For instance, when the patient swallows a bolus of food, as the food touches a tonsil, it might set off a severe lancinating pain in the mandibular portion of the fifth nerve. The pain of tic douloureux can usually be blocked by surgically cutting the peripheral nerve from the hypersensitive area. The sensory portion of the fifth nerve is often sectioned immediately inside the cranium, where the motor and sensory roots of the fifth nerve separate from each other, so that the motor portions, which are necessary for many jaw movements, can be spared while the sensory elements are destroyed. Furthermore, sometimes the operation is unsuccessful, indicating that the lesion that causes the pain might be in the sensory nucleus in the brain stem and not in the peripheral nerves. Pain impulses pass first from the appendix through visceral pain fibers located within sympathetic nerve bundles, and then into the spinal cord at about T10 or T11; this pain is referred to an area around the umbilicus and is of the aching, cramping type. Pain impulses also often originate in the parietal peritoneum where the inflamed appendix touches or is adherent to the abdominal wall. These impulses cause pain of the sharp type directly over the irritated peritoneum in the right lower quadrant of the abdomen. Cross section of the spinal cord, showing principal ascending tracts on the right and principal descending tracts on theleft. All motor functions are blocked on the side of the transection in all segments below the level of the transection. Yet, only some of the modalities of sensation are lost on the transected side, and others are lost on the opposite side. The sensations of pain, heat, and cold-sensations served by the spinothalamic pathway-are lost on the opposite side of the body in all dermatomes two to six segments below the level of the transection. By contrast, the sensations that are transmitted only in the dorsal and dorsolateral columns-kinesthetic and position sensations, vibration sensation, discrete localization, and two-point discrimination-are lost on the side of the transection in all dermatomes below the level of the transection. Discrete "light touch" is impaired on the side of the transection because the principal pathway for the transmission of light touch, the dorsal column, is transected. That is, the fibers in this column do not cross to the opposite side until they reach the medulla of the brain. Conversely, tugging on the venous sinuses around the brain, damaging the tentorium, or stretching the dura at the base of the brain can cause intense pain that is recognized as headache. Also, almost any type of traumatizing, crushing, or stretching stimulus to the blood vessels of the meninges can cause headache. An especially sensitive structure is the middle meningeal artery, and neurosurgeons are careful to anesthetize this artery specifically when performing brain operations with use of local anesthesia. Conversely, pain impulses from beneath the tentorium enter the central nervous system mainly through the glossopharyngeal, vagal, and second cervical nerves, which also supply the scalp above, behind, and slightly below the ear. Subtentorial pain stimuli cause "occipital headache" referred to the posterior part of the head. One of the most severe headAreas of the Head to Which Intracranial Headache Is Referred. Stimulation of pain receptors in the cerebral Headache Headaches are a type of pain referred to the surface of the head from deep head structures. Some headaches result from pain stimuli arising inside the cranium, but others result from pain arising outside the cranium, such as from the nasal sinuses.
Generic 30mg procardia otc
Speech is composed of two mechanical functions: (1) phonation screening cardiovascular disease icd 9 best buy for procardia, which is achieved by the larynx, and (2) articulation, which is achieved by the structures of the mouth. The vocal cords protrude from the lateral walls of the larynx toward the center of the glottis; they are stretched and positioned by several specific muscles of the larynx itself. During phonation, the cords move together so that passage of air between them will cause vibration. The pitch of the vibration is determined mainly by the degree of stretch of the cords, but also by how tightly the cords are approximated to one another and by the mass of their edges. Immediately inside each cord is a strong elastic ligament called the vocal ligament. The vocal cords can be stretched by either forward rota tion of the thyroid cartilage or posterior rotation of the arytenoid cartilages, activated by muscles stretching from the thyroid cartilage and arytenoid cartilages to the cricoid cartilage. Muscles located within the vocal cords lateral to the vocal ligaments, the thyroarytenoid muscles, can pull the arytenoid cartilages toward the thyroid cartilage and, therefore, loosen the vocal cords. Also, slips of these muscles within the vocal cords can change the shapes and masses of the vocal cord edges, sharpening them to emit highpitched sounds and blunting them for the more bass sounds. They need not be discussed in detail because we are all familiar with their movements during speech and other vocalizations. The resonators include the mouth, the nose and associated nasal sinuses, the pharynx, and even the chest cavity. For instance, the function of the nasal resonators is demonstrated by the change in voice quality when a person has a severe cold that blocks the air passages to these resonators. The high-pressure, low-flow circulation supplies systemic arterial blood to the trachea, the bronchial tree (including the terminal bronchioles), the supporting tissues of the lung, and the outer coats (adventitia) of the pulmonary arteries and veins. The bronchial arteries, which are branches of the thoracic aorta, supply most of this systemic arterial blood at a pressure that is only slightly lower than the aortic pressure. The pulmonary artery (which receives blood from the right ventricle) and its arterial branches carry blood to the alveolar capillaries for gas exchange, and the pulmonary veins then return the blood to the left atrium to be pumped by the left ventricle though the systemic circulation. In this chapter we discuss the special aspects of the pulmonary circulation that are important for gas exchange in the lungs. Blood also flows to the lungs through small bronchial arteries that originate from the systemic circulation, amounting to 1 to 2 percent of the total cardiac output. This bronchial arterial blood is oxygenated blood, in contrast to the partially deoxygenated blood in the pulmonary arteries. It supplies the supporting tissues of the lungs, including the connective tissue, septa, and large and small bronchi. After this bronchial and arterial blood passes through the supporting tissues, it empties into the pulmonary veins and enters the left atrium, rather than passing back to the right atrium. Therefore, the flow into the left atrium and the left ventricular output are about 1 to 2 percent greater than that of the right ventricular output. The pulmonary artery extends only portive tissues of the lung, beginning in the connective tissue spaces that surround the terminal bronchioles, coursing to the hilum of the lung, and then mainly into the right thoracic lymph duct. Particulate matter entering the alveoli is partly removed by way of these channels, and plasma protein leaking from the lung capillaries is also removed from the lung tissues, thereby helping to prevent pulmonary edema. Lymph vessels are present in all the sup- 5 centimeters beyond the apex of the right ventricle and then divides into right and left main branches that supply blood to the two respective lungs. The pulmonary arterial branches are short, and all the pulmonary arteries, even the smaller arteries and arterioles, have larger diameters than their counterpart systemic arteries. This aspect, combined with the fact that the vessels are thin and distensible, gives the pulmonary arterial tree a large compliance, averaging almost 7 ml/mm Hg, which is similar to that of the entire systemic arterial tree. This large compliance allows the pulmonary arteries to accommodate the stroke volume output of the right ventricle. These curves are contrasted with the much higher aortic pressure curve shown in the upper portion of the figure. The systolic pressure in the right ventricle of the normal human averages about 25 mm Hg, and the diastolic pressure averages about 0 to 1 mm Hg, values that are only one fifth those for the left ventricle. The pressure measured through the catheter, called the "wedge pressure," is about 5 mm Hg. Because all blood flow has been stopped in the small wedged artery, and because the blood vessels extending beyond this artery make a direct connection with the pulmonary capillaries, this wedge pressure is usually only 2 to 3 mm Hg greater than the left atrial pressure. When the left atrial pressure rises to high values, the pulmonary wedge pressure also rises. Therefore, wedge pressure measurements can be used to study changes in pulmonary capillary pressure and left atrial pressure in patients with congestive heart failure. Approximately 70 milliliters of this pulmonary blood volume is in the pulmonary capillaries, and the remainder is divided about equally between the pulmonary arteries and the veins. The importance of this low capillary pressure is discussed in detail later in the chapter in relation to fluid exchange functions of the pulmonary capillaries. The mean pressure in the left atrium and the major pulmonary veins averages about 2 mm Hg in the recumbent human being, varying from as low as 1 mm Hg to as high as 5 mm Hg. However, the left atrial pressure can be estimated with moderate accuracy by measuring the so-called pulmonary wedge pressure. This measurement is achieved by inserting a catheter first through a peripheral vein to the right atrium, then through physiological and pathological conditions, the quantity of blood in the lungs can vary from as little as one-half normal up to twice normal. For instance, when a person blows out air so hard that high pressure is built up in the lungs, such as when blowing a trumpet, as much as 250 milliliters of blood can be expelled from the pulmonary circulatory system into the systemic circulation. Also, loss of blood from the systemic circulation by hemorrhage can be partly compensated for by the automatic shift of blood from the lungs into the systemic vessels. Because the volume of the systemic circulation is about nine times that of the pulmonary system, a shift of blood from one system to the other affects the pulmonary system greatly but usually has only mild systemic circulatory effects. Cardiac Pathology May Shift Blood From the Systemic Circulation to the Pulmonary Circulation. Therefore, the factors that control 510 Chapter 39 PulmonaryCirculation,PulmonaryEdema,PleuralFluid cardiac output-mainly peripheral factors, as discussed in Chapter 20-also control pulmonary blood flow. Under most conditions, the pulmonary vessels act as distensible tubes that enlarge with increasing pressure and narrow with decreasing pressure. For adequate aeration of the blood to occur, the blood must be distributed to the segments of the lungs where the alveoli are best oxygenated. Decreased Alveolar Oxygen Reduces Local Alveolar Blood Flow and Regulates Pulmonary Blood Flow Distribution. This effect is opposite to the effect observed in systemic vessels, which dilate rather than constrict in response to low O2 levels. Although the mechanisms that promote pulmonary vasoconstriction during hypoxia are not completely understood, low O2 concentration may stimulate release of vasoconstrictor substances or decrease release of a vasodilator, such as nitric oxide, from the lung tissue. Some studies suggest that hypoxia may directly induce vasoconstriction by inhibition of oxygen-sensitive potassium ion channels in pulmonary vascular smooth muscle cell membranes. With low partial pressures of oxygen, these channels are blocked, leading to depolarization of the cell membrane and activation of calcium channels, causing influx of calcium ions. The rise of calcium concentration then causes constriction of small arteries and arterioles. The increase in pulmonary vascular resistance as a result of low O2 concentration has the important function of distributing blood flow where it is most effective. That is, if some alveoli are poorly ventilated and have a low O2 concentration, the local vessels constrict. This constriction causes the blood to flow through other areas of the lungs that are better aerated, thus providing an automatic control system for distributing blood flow to the pulmonary areas in proportion to their alveolar O2 pressures. That is, the pulmonary arterial pressure in the uppermost portion of the lung of a standing person is about 15 mm Hg less than the pulmonary arterial pressure at the level of the heart, and the pressure in the lowest portion of the lungs is about 8 mm Hg greater. Such pressure differences have profound effects on blood flow through the different areas of the lungs. Note that in the standing position at rest, there is little flow in the top of the lung but about five times as much flow in the bottom. Therefore, any time the lung alveolar air pressure becomes greater than the capillary blood pressure, the capillaries close and there is no blood flow. This difference is caused by hydrostatic pressure-that is, by the weight of the blood itself in the blood vessels. Therefore, continuous flow occurs through the alveolar capillaries, or zone 3 blood flow.
Buy generic procardia 30mg line
The result is a widespread reaction throughout the body called the alarm or stress response cardiovascular nutrition buy procardia 30mg amex, which is discussed shortly. At other times, activation occurs in isolated portions of the sympathetic nervous system. During the process of heat regulation, the sympathetics control sweating and blood flow in the skin without affecting other organs innervated by the sympathetics. Many "local reflexes" involving sensory afferent fibers travel centrally in the peripheral nerves to the sympathetic ganglia and spinal cord and cause highly localized reflex responses. For instance, heating a skin area causes local vasodilation and enhanced local sweating, whereas cooling causes opposite effects. Many of the sympathetic reflexes that control gastrointestinal functions operate by way of nerve pathways that do not even enter the spinal cord, merely passing from the gut mainly to the paravertebral ganglia, and then back to the gut through sympathetic nerves to control motor or secretory activity. For instance, parasympathetic cardiovascular reflexes usually act only on the heart to increase or decrease its rate of beating. Likewise, other parasympathetic reflexes cause secretion mainly by the mouth glands, and in other instances secretion is mainly by the stomach glands. Finally, the rectal emptying reflex does not affect other parts of the bowel to a major extent. For instance, although salivary secretion can occur independently of gastric secretion, these two also often occur together, and pancreatic secretion frequently occurs at the same time. Also, the rectal emptying reflex often initiates a urinary bladder emptying reflex, resulting in simultaneous emptying of both the bladder and the rectum. Some of the most important factors controlled in the brain stem are arterial pressure, heart rate, and respiratory rate. Motor and Integrative Neurophysiology Pharmacology of the Autonomic Nervous System Parasympathetic Water balance Feeding control Hypothalamus Pituitary gland Mammillary body Urinary bladder control Pneumotaxic center Cardiac acceleration and vasoconstriction Cardiac slowing Respiratory center Heat control Sympathetic Drugs That Act on Adrenergic Effector Organs-Sympathomimetic Drugs From the foregoing discussion, it is obvious that intravenous injection of norepinephrine causes essentially the same effects throughout the body as sympathetic stimulation. Epinephrine and methoxamine are also sympathomimetic drugs, and there are many others. They differ from one another in the degree to which they stimulate different sympathetic effector organs and in their duration of action. Norepinephrine and epinephrine have actions as short as 1 to 2 minutes, whereas the actions of some other commonly used sympathomimetic drugs last for 30 minutes to 2 hours. Important drugs that stimulate specific adrenergic receptors are phenylephrine (alpha receptors), isoproterenol (beta receptors), and albuterol (only beta2 receptors). Their effect is to cause release of norepinephrine from its storage vesicles in the sympathetic nerve endings. Adrenergic activity can be blocked at several points in the stimulatory process, as follows: 1. The synthesis and storage of norepinephrine in the sympathetic nerve endings can be prevented. Two drugs that block both alpha1 and alpha2 adrenergic receptors are phenoxybenzamine and phentolamine. Selective alpha1 adrenergic blockers include prazosin and terazosin, whereas yohimbine blocks alpha2 receptors. Sympathetic activity can be blocked by drugs that block transmission of nerve impulses through the autonomic ganglia. They are discussed in a later section, but an important drug for blockade of both sympathetic and parasympathetic transmission through the ganglia is hexamethonium. Drugs That Act on Cholinergic Effector Organs Parasympathomimetic Drugs (Cholinergic Drugs). Conversely, transection immediately below the medulla causes the arterial pressure to fall to less than one-half normal. Closely associated with the cardiovascular regulatory centers in the brain stem are the medullary and pontine centers for regulation of respiration, which are discussed in Chapter 42. Although regulation of respiration is not considered to be an autonomic function, it is one of the involuntary functions of the body. Signals from the hypothalamus and even from the cerebrum can affect the activities of almost all the brain stem autonomic control centers. For instance, stimulation in appropriate areas-mainly of the posterior hypothalamus-can activate the medullary cardiovascular control centers strongly enough to increase arterial pressure to more than twice normal. Likewise, other hypothalamic centers control body temperature, increase or decrease salivation and gastrointestinal activity, and cause bladder emptying. To some extent, therefore, the autonomic centers in the brain stem act as relay stations for control activities initiated at higher levels of the brain, especially in the hypothalamus. In Chapters 59 and 60, it is pointed out also that many of our behavioral responses are mediated through (1) the hypothalamus, (2) the reticular areas of the brain stem, and (3) the autonomic nervous system. Indeed, some higher areas of the brain can alter function of the whole autonomic nervous system or of portions of it strongly enough to cause severe autonomicinduced disease such as peptic ulcer of the stomach or duodenum, constipation, heart palpitation, or even heart attack. Yet a number of other drugs that are not so rapidly destroyed can produce typical widespread parasympathetic effects; they are called parasympathomimetic drugs. They are the same drugs as those discussed in Chapter 7 that potentiate the effect of acetylcholine at the neuromuscular junction. They inhibit acetylcholinesterase, thus preventing rapid destruction of the acetylcholine liberated at parasympathetic nerve endings. As a consequence, the quantity of acetylcholine increases with successive stimuli, and the degree of action also increases. These drugs do not affect the nicotinic action of acetylcholine on the postganglionic neurons or on skeletal muscle. Drugs That Stimulate or Block Sympathetic and Parasympathetic Postganglionic Neurons Drugs That Stimulate Autonomic Postganglionic Neurons. The preganglionic neurons of both the parasymDrugs That Block Cholinergic Activity at Effector Organs-Antimuscarinic Drugs. Atropine and similar Drugs That Have a Parasympathetic Potentiating Effect-Anticholinesterase Drugs. Drugs that block impulse transmission from the autonomic preganglionic neurons to the postganglionic neurons include tetraethyl ammonium ion, hexamethonium ion, and pentolinium. These drugs block acetylcholine stimulation of the postganglionic neurons in both the sympathetic and the parasympathetic systems simultaneously. They are often used for blocking sympathetic activity but seldom for blocking parasympathetic activity because their effects of sympathetic blockade usually far overshadow the effects of parasympathetic blockade. The ganglionic blocking drugs especially can reduce the arterial pressure rapidly, but they are not very useful clinically because their effects are difficult to control. Dajas-Bailador F, Wonnacott S: Nicotinic acetylcholine receptors and the regulation of neuronal signalling. Furthermore, injected acetylcholine can also stimulate the postganglionic neurons of both systems, thereby causing at the same time both sympathetic and parasympathetic effects throughout the body. Nicotine is another drug that can stimulate postganglionic neurons in the same manner as acetylcholine because the membranes of these neurons all contain the nicotinic type of acetylcholine receptor. Therefore, drugs that cause autonomic effects by stimulating postganglionic neurons are called nicotinic drugs. Some other drugs, such as methacholine, have both nicotinic and muscarinic actions, whereas pilocarpine has only muscarinic actions. Nicotine excites both the sympathetic and parasympathetic postganglionic neurons at the same time, resulting in strong sympathetic vasoconstriction in the abdominal organs and limbs but at the same time resulting in parasympathetic effects such as increased gastrointestinal activity. However, this is far from true because abnormalities of any of these aspects can profoundly affect brain function. For instance, total cessation of blood flow to the brain causes unconsciousness within 5 to 10 seconds because lack of oxygen delivery to the brain cells nearly shuts down metabolism in these cells. Also, on a longer time scale, abnormalities of the cerebrospinal fluid, either its composition or its fluid pressure, can have equally severe effects on brain function. Excesses of Carbon Dioxide or Hydrogen Ion Concen tration Increase Cerebral Blood Flow. The penetrating vessels are separated slightly from the brain tissue by an extension of the subarachnoid space called the Virchow-Robin space. The penetrating vessels dive down into the brain tissue, giving rise to intracerebral arterioles, which eventually branch into capillaries where exchange among the blood and the tissues of oxygen, nutrients, carbon dioxide, and metabolites occurs. Thus, the brain constitutes only about 2 percent of the body weight but receives 15 percent of the resting cardiac output. As in most other tissues, cerebral blood flow is highly related to the tissue metabolism. Thus, the oxygen mechanism for local regulation of cerebral blood flow is an important protective response against diminished cerebral neuronal activity and, therefore, against derangement of mental capability. The hydrogen ions then cause vasodilation of the cerebral vessels, with the dilation being almost directly proportional to the increase in hydrogen ion concentration up to a blood flow limit of about twice normal.
Vitis vinifera (Grape). Procardia.
- Preventing heart disease, treating varicose veins, hemorrhoids, constipation, cough, attention deficit-hyperactivity disorder (ADHD), chronic fatigue syndrome (CFS), diarrhea, heavy menstrual bleeding (periods), age-related macular degeneration (ARMD), canker sores, poor night vision, liver damage, high cholesterol levels, and other conditions.
- Dosing considerations for Grape.
- What is Grape?
- Are there any interactions with medications?
- How does Grape work?
- Hayfever and seasonal nasal allergies.
- Are there safety concerns?
- Decreasing certain types of eye stress.
- Circulation problems, such as chronic venous insufficiency that can cause the legs to swell.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96481
Buy line procardia
Yet water continues to be reabsorbed blood vessels in your nose purchase cheap procardia on-line, causing the tubular hemoglobin concentration to rise so high that the hemoglobin precipitates and blocks many of the kidney tubules. Thus, renal vasoconstriction, circulatory shock, and renal tubular blockage together cause acute renal shutdown. If the shutdown is complete and fails to resolve, the patient dies within a week to 12 days, as explained in Chapter 32, unless he or she is treated with an artificial kidney. Some of the different cellular tissues and organs that have been transplanted as allografts, either experimentally or for therapeutic purposes, from one person to another are skin, kidney, heart, liver, glandular tissue, bone marrow, and lung. With proper "matching" of tissues between persons, many kidney allografts have been successful for at least 5 to 15 years, and allograft liver and heart transplants for 1 to 15 years. The following specific procedures have met with some degrees of clinical or experimental success. Consequently, foreign cells transplanted anywhere into the body of a recipient can produce immune reactions. A transplant of a tissue or whole organ from one part of the same animal to another part is called an autograft; from one identical twin to another, an isograft; from one human being to another or from any animal to another animal of the same species, an allograft; and from a non-human animal to a human being or from an animal of one species to one of another species, a xenograft. At the other extreme, immune reactions almost always occur in xenografts, causing death of the cells in the graft within 1 day to 5 weeks after transplantation unless Transplantation of Cellular Tissues. Development of significant immunity against any of these antigens can cause graft rejection. The lymphocytes are mixed with appropriate antisera and complement; after incubation, the cells are tested for membrane damage, usually by testing the rate of transmembrane uptake by the lymphocytic cells of a special dye. Therefore, a precise match of some antigens between donor and recipient is not always essential to allow allograft acceptance. By obtaining the best possible match between donor and recipient, the grafting procedure has become far less hazardous. The best success has been with tissue-type matches between siblings and between parent and child. The match in identical twins is exact, so transplants between identical twins are almost never rejected because of immune reactions. Prevention of Graft Rejection by Suppressing the Immune System If the immune system were completely suppressed, graft rejection would not occur. However, in the normal person, even with the best possible tissue typing, allografts seldom resist rejection for more than a few days or weeks without use of specific therapy to suppress the immune system. Furthermore, because the T cells are mainly the portion of the immune system important for killing grafted cells, their suppression is much more important than suppression of plasma antibodies. Some of the therapeutic agents that have been used for this purpose include the following: 1. Various drugs that have a toxic effect on the lymphoid system and, therefore, block formation of antibodies and T cells, especially the drug azathioprine. Cyclosporine and tacrolimus, which inhibit formation of T-helper cells and, therefore, are especially efficacious in blocking the T-cell rejection reaction. These agents have proved to be highly valuable drugs because they do not depress some other portions of the immune system. Use of these agents often leaves the person unprotected from infectious disease; therefore, sometimes bacterial and viral infections become rampant. In addition, the incidence of cancer is several times greater in an immunosuppressed person, presumably because the immune system is important in destroying many early cancer cells before they can begin to proliferate. Transplantation of living tissues in human beings has had important success mainly because of the development of drugs that suppress the responses of the immune system. With the introduction of improved immunosuppressive agents, successful organ transplantation has become much more common. The current approach to immunosuppressive therapy attempts to balance acceptable rates of rejection with moderation in the adverse effects of immunosuppressive drugs. SafiniaN,LeechJ,Hernandez-FuentesM,etal:Promotingtransplantation tolerance; adoptive regulatory T cell therapy. Whenever a vessel is severed or ruptured, hemostasis is achieved by several mechanisms: (1) vascular constric tion, (2) formation of a platelet plug, (3) formation of a blood clot as a result of blood coagulation, and (4) even tual growth of fibrous tissue into the blood clot to close the hole in the vessel permanently. Physical and Chemical Characteristics of Platelets Platelets (also called thrombocytes) are minute discs 1 to 4 micrometers in diameter. They are formed in the bone marrow from megakaryocytes, which are extremely large hematopoietic cells in the marrow; the megakaryocytes fragment into the minute platelets either in the bone marrow or soon after entering the blood, especially as they squeeze through capillaries. The normal concentra tion of platelets in the blood is between 150,000 and 300,000 per microliter. Platelets have many functional characteristics of whole cells, even though they do not have nuclei and cannot reproduce. On the platelet cell membrane surface is a coat of glycoproteins that repulses adherence to normal endothelium and yet causes adherence to injured areas of the vessel wall, especially to injured endothelial cells and even more so to any exposed collagen from deep within the vessel wall. In addition, the platelet membrane contains large amounts of phospholipids that activate multiple stages in the bloodclotting process, as we discuss later. The contraction results from (1) local myogenic spasm, (2) local autacoid factors from the traumatized tissues and blood platelets, and (3) nervous reflexes. The ner vous reflexes are initiated by pain nerve impulses or other sensory impulses that originate from the trauma tized vessel or nearby tissues. However, even more vasoconstriction probably results from local myogenic contraction of the blood vessels initiated by direct damage to the vascular wall. And, for the smaller vessels, the platelets are responsible for much of the vasoconstric tion by releasing a vasoconstrictor substance, thromboxane A2. The more severely a vessel is traumatized, the greater the degree of vascular spasm. The spasm can last for many minutes or even hours, during which time the processes of platelet plugging and blood coagulation can take place. To understand this process, it is important that we first discuss the nature of platelets themselves. More than one half of the platelets are removed by mac rophages in the spleen, where the blood passes through a latticework of tight trabeculae. Platelets agglutinate Mechanism of the Platelet Plug Platelet repair of vascular openings is based on several important functions of the platelet. When platelets come in contact with a damaged vascular surface, especially with collagen fibers in the vascular wall, the platelets rapidly change their own characteristics drastically. Therefore, at the site of a puncture in a blood vessel wall, the damaged vascular wall activates successively increasing numbers of platelets that attract more and more additional platelets, thus forming a platelet plug. This plug is loose at first, but it is usually successful in blocking blood loss if the vascular opening is small. These threads attach tightly to the platelets, thus constructing an unyielding plug. Indeed, multiple small holes through the endothelial cells themselves are often closed by platelets actually fusing with the endothelial cells to form additional endo thelial cell membrane. Literally thousands of small hem orrhagic areas develop each day under the skin and throughout the internal tissues of a person who has few blood platelets. The clot begins to develop in 15 to 20 seconds if the trauma to the vascular wall has been severe and in 1 to 2 minutes if the trauma has been minor. Activator substances from the traumatized vascular wall, from platelets, and from blood proteins adhering 484 to the traumatized vascular wall initiate the clotting process. Within 3 to 6 minutes after rupture of a vessel, the entire opening or broken end of the vessel is filled with Chapter 37 HemostasisandBloodCoagulation clot if the vessel opening is not too large. After 20 minutes to an hour, the clot retracts, which closes the vessel still further. Platelets also play an important role in this clot retraction, as discussed later. The usual course for a clot that forms in a small hole of a vessel wall is invasion by fibroblasts, beginning within a few hours after the clot is formed (which is promoted at least partially by growth factor secreted by platelets). This process continues to complete organization of the clot into fibrous tissue within about 1 to 2 weeks.
Procardia 30 mg overnight delivery
If the dominant eye then becomes blinded cardiovascular system in order order procardia 30 mg on-line, vision in the repressed eye can develop only to a slight extent in adults but far more in young children. This demonstrates that visual acuity is highly dependent on proper development of central nervous system synaptic connections from the eyes. In fact, even anatomically, the numbers of neuronal connections diminish in the visual cortex areas that would normally receive signals from the repressed eye. The parasympathetic preganglionic fibers arise in the EdingerWestphal nucleus (the visceral nucleus portion of the third cranial nerve) and then pass in the third nerve to the ciliary ganglion, which lies immediately behind the eye. There, the preganglionic fibers synapse with postganglionic parasympathetic neurons, which in turn send fibers through ciliary nerves into the eyeball. These nerves excite (1) the ciliary muscle that controls focusing of the eye lens and (2) the sphincter of the iris that constricts the pupil. The sympathetic innervation of the eye originates in the intermediolateral horn cells of the first thoracic segment of the spinal cord. From there, sympathetic fibers enter the sympathetic chain and pass upward to the superior cervical ganglion, where they synapse with postganglionic neurons. Postganglionic sympathetic fibers from these then spread along the surfaces of the carotid artery and successively smaller arteries until they reach the eye. Contraction causes increased refractive power of the lens, as explained in Chapter 50, and relaxation causes decreased power. Accommodation of the lens is regulated by a negative feedback mechanism that automatically adjusts the refractive power of the lens to achieve the highest degree of visual acuity. When the eyes have been focused on some far object and must then suddenly focus on a near object, the lens usually accommodates for best acuity of vision within less than 1 second. Although the precise control mechanism that causes this rapid and accurate focusing of the eye is unclear, the following features are known. The Special Senses First, when the eyes suddenly change distance of the fixation point, the lens changes its strength in the proper direction to achieve a new state of focus within a fraction of a second. Second, different types of clues help to change the lens strength in the proper direction: 1. That is, red light rays focus slightly posteriorly to blue light rays because the lens bends blue rays more than red rays. The eyes appear to be able to detect which of these two types of rays is in better focus, and this clue relays information to the accommodation mechanism with regard to whether to make the lens stronger or weaker. The neural mechanisms for convergence cause a simultaneous signal to strengthen the lens of the eye. Because the fovea lies in a hollowed-out depression that is slightly deeper than the remainder of the retina, the clarity of focus in the depth of the fovea is different from the clarity of focus on the edges. This difference may also give clues about which way the strength of the lens needs to be changed. The degree of accommodation of the lens oscillates slightly all the time at a frequency up to twice per second. The visual image becomes clearer when the oscillation of the lens strength is changing in the appropriate direction and becomes poorer when the lens strength is changing in the wrong direction. This could give a rapid clue as to which way the strength of the lens needs to change to provide appropriate focus. The brain cortical areas that control accommodation closely parallel those that control fixation movements of the eyes. Edinger-Westphal nucleus and, finally, back through parasympathetic nerves to constrict the sphincter of the iris. Conversely, in darkness, the reflex becomes inhibited, which results in dilation of the pupil. The function of the light reflex is to help the eye adapt extremely rapidly to changing light conditions, as explained in Chapter 51. Therefore, because light brightness on the retina increases with the square of pupillary diameter, the range of light and dark adaptation that can be brought about by the pupillary reflex is about 30 to 1- that is, up to as much as 30 times change in the amount of light entering the eye. Conversely, stimulation of the sympathetic nerves excites the radial fibers of the iris and causes pupillary dilation, which is called mydriasis. When light is shone into the eyes, the pupils constrict, a reaction called the pupillary light reflex. When light impinges on the retina, a few of the resulting impulses pass from the optic nerves to the pretectal nuclei. From here, secondary impulses pass to the damage nerve transmission of visual signals from the retinas to the Edinger-Westphal nucleus, thus sometimes blocking the pupillary reflexes. Such blocks may occur as a result of central nervous system syphilis, alcoholism, encephalitis, and so forth. The block usually occurs in the pretectal region of the brain stem, although it can result from destruction of some small fibers in the optic nerves. The final nerve fibers in the pathway through the pretectal area to the Edinger-Westphal nucleus are mostly of the inhibitory type. When their inhibitory effect is lost, the nucleus becomes chronically active, causing the pupils to remain mostly constricted, in addition to their failure to respond to light. Yet the pupils can constrict a little more if the EdingerWestphal nucleus is stimulated through some other pathway. For instance, when the eyes fixate on a near object, the signals that cause accommodation of the lens and those that cause convergence of the two eyes cause a mild degree of pupillary constriction at the same time. A pupil that fails to respond to light but does respond to accommodation and is also very small (an Argyll Robertson pupil) is an important diagnostic sign of a central nervous system disease such as syphilis. This syndrome consists of the following effects: First, because of interruption of sympathetic nerve fibers to the pupillary dilator muscle, the pupil remains persistently constricted to a smaller diameter than the pupil of the opposite eye. Second, the superior eyelid droops because it is normally maintained in an open position during waking hours partly by contraction of smooth muscle fibers embedded in the superior eyelid and innervated by the sympathetics. Therefore, destruction of the sympathetic nerves makes it impossible to open the superior eyelid as widely as normally. Third, the blood vessels on the corresponding side of the face and head become persistently dilated. Hikosaka O, Takikawa Y, Kawagoe R: Role of the basal ganglia in the control of purposive saccadic eye movements. Instead, the system actually reduces the distance but increases the force of movement about 1. In addition, the surface area of the tympanic membrane is about 55 square millimeters, whereas the surface area of the stapes averages 3. Because fluid has far greater inertia than air does, increased amounts of force are necessary to cause vibration in the fluid. Therefore, the tympanic membrane and ossicular system provide impedance matching between the sound waves in air and the sound vibrations in the fluid of the cochlea. Indeed, the impedance matching is about 50 to 75 percent of perfect for sound frequencies between 300 and 3000 cycles/sec, which allows utilization of most of the energy in the incoming sound waves. In the absence of the ossicular system and tympanic membrane, sound waves can still travel directly through the air of the middle ear and enter the cochlea at the oval window. However, the sensitivity for hearing is then 15 to 20 decibels less than for ossicular transmission- equivalent to a decrease from a medium to a barely perceptible voice level. The malleus is bound to the incus by minute ligaments, so whenever the malleus moves, the incus moves with it. The opposite end of the incus articulates with the stem of the stapes, and the faceplate of the stapes lies against the membranous labyrinth of the cochlea in the opening of the oval window. The tip end of the handle of the malleus is attached to the center of the tympanic membrane, and this point of attachment is constantly pulled by the tensor tympani muscle, which keeps the tympanic membrane tensed. This tension allows sound vibrations on any portion of the tympanic membrane to be transmitted to the ossicles, which would not be true if the membrane were lax. The ossicles of the middle ear are suspended by ligaments in such a way that the combined malleus and incus act as a single lever, having its fulcrum approximately at the border of the tympanic membrane. The articulation of the incus with the stapes causes the stapes to (1) push forward on the oval window and on the cochlear fluid on the other side of window every time the tympanic membrane moves inward and (2) pull backward on the fluid every time the malleus moves outward. The Auditory canal Tympanic membrane amplitude of movement of the stapes faceplate with each sound vibration is only three fourths as much as the amplitude of the handle of the malleus. The Special Senses Attenuation of Sound by Contraction of the Tensor Tympani and Stapedius Muscles. When loud sounds Basilar Spiral organ membrane of Corti Spiral ligament Vestibular membrane Scala vestibuli Stria vascularis are transmitted through the ossicular system and from there into the central nervous system, a reflex occurs after a latent period of only 40 to 80 milliseconds to cause contraction of the stapedius muscle and, to a lesser extent, the tensor tympani muscle. The tensor tympani muscle pulls the handle of the malleus inward while the stapedius muscle pulls the stapes outward. These two forces oppose each other and thereby cause the entire ossicular system to develop increased rigidity, thus greatly reducing the ossicular conduction of low-frequency sound, mainly frequencies below 1000 cycles/sec.
Order 30 mg procardia mastercard
The electrically stimulated patients told their thoughts evoked by the stimulation glomerular capillaries function order generic procardia from india, and sometimes they experienced movements. Occasionally they spontaneously emitted a sound or even a word or gave some other evidence of the stimulation. This figure shows the major primary and secondary premotor and supplementary motor areas of the cortex, as well as the major primary and secondary sensory areas for somatic sensation, vision, and hearing, all of which are discussed in earlier chapters. The primary motor areas have direct connections with specific muscles for causing discrete muscle movements. The primary sensory areas detect specific sensations-visual, auditory, or somatic- transmitted directly to the brain from peripheral sensory organs. These areas are called association areas because they receive and analyze signals simultaneously from multiple regions of both the motor and sensory cortices, as well as from subcortical structures. Important association areas include (1) the parieto-occipitotemporal association area, (2) the prefrontal association area, and (3) the limbic association area. As would be expected, it provides a high level of interpretative meaning for signals from all the surrounding sensory areas. Locations of major association areas of the cerebral cortex, as well as primary and secondary motor and sensory areas. This area receives visual sensory information from the posterior occipital cortex and simultaneous somatosensory information from the anterior parietal cortex. From all this information, it computes the coordinates of the visual, auditory, and body surroundings. We discuss this area more fully later; it is the most important region of the entire brain for higher intellectual function because almost all such intellectual functions are language based. The Angular Gyrus Area Is Needed for Initial Processing of Visual Language (Reading). The major area for language comprehension, of thoughts, and it is said to store on a short-term basis "working memories" that are used to combine new thoughts while they are entering the brain. This so-called angular gyrus area is needed to make meaning out of the visually perceived words. In its absence, a person can still have excellent language comprehension through hearing but not through reading. In the most lateral portions located partly in the posterior lateral prefrontal cortex and partly in the premotor area. It is here that plans and motor patterns for expressing individual words or even short phrases are initiated and executed. This area also works in close association with the Wernicke language comprehension center in the temporal association cortex, as we discuss more fully later in the chapter. An especially interesting discovery is the following: When a person has already learned one language and then learns a new language, the area in the brain where the new language is stored is slightly removed from the storage area for the first language. If both languages are learned simultaneously, they are stored together in the same area of the brain. This area is found in the anterior pole of the temporal lobe, in the ventral portion of the frontal lobe, and in the cingulate gyrus lying deep in the longitudinal fissure on the midsurface of each cerebral hemisphere. We discuss in Chapter 59 that the limbic cortex is part of a much more extensive system, the limbic system, that includes a complex set of neuronal structures in the midbasal regions of the brain. This limbic system provides most of the emotional drives for activating other areas of the brain and even provides motivational drive for the process of learning itself. The names are learned mainly through auditory input, whereas the physical natures of the objects are learned mainly through visual input. Prefrontal Association Area As discussed in Chapter 57, the prefrontal association area functions in close association with the motor cortex to plan complex patterns and sequences of motor movements. To aid in this function, it receives strong input through a massive subcortical bundle of nerve fibers connecting the parieto-occipitotemporal association area with the prefrontal association area. Through this bundle, the prefrontal cortex receives much preanalyzed sensory information, especially information on the spatial coordinates of the body that is necessary for planning effective movements. The prefrontal association area is also essential to carrying out "thought" processes. This characteristic presumably results from some of the same capabilities of the prefrontal cortex that allow it to plan motor activities. It seems to be capable of processing nonmotor and motor information from widespread areas of the brain and therefore to achieve nonmotor types of thinking, as well as motor types. In fact, the prefrontal association area is frequently described simply as important for elaboration 740 Area for Recognition of Faces An interesting type of brain abnormality called prosopagnosia is the inability to recognize faces. Loss of these face recognition areas, strangely enough, results in little other abnormality of brain function. One may wonder why so much of the cerebral cortex should be reserved for the simple task of face recognition. However, most of our daily tasks involve associations with other people, and thus one can see the importance of this intellectual function. Likewise, the person may be able to read words from the printed page but be unable to recognize the thought that is conveyed. The types of thoughts that might be experienced include complicated visual scenes that one might remember from childhood, auditory hallucinations such as a specific musical piece, or even a statement made by a specific person. This area of confluence of the different sensory interpretative areas is especially highly developed in the dominant side of the brain-the left side in almost all right-handed people-and it plays the greatest single role of any part of the cerebral cortex for the higher comprehension levels of brain function that we call intelligence. Therefore, the person may be able to see words and even know that they are words but not be able to interpret their meanings. Loss of this area in an adult usually leads thereafter to a lifetime of almost demented existence. Therefore, it is easy to understand why the left side of the brain might become dominant over the right side. However, if for some reason this left side area is damaged or removed in very early childhood, the opposite side of the brain will usually develop dominant characteristics. The following theory can explain the capability of one hemisphere to dominate the other hemisphere. The attention of the "mind" seems to be directed to one principal thought at a time. Presumably, because the left posterior temporal lobe at birth is usually slightly larger than the right lobe, the left side normally begins to be used to a greater extent than is the right side. In about 95 percent of all people, the left temporal lobe and angular gyrus become dominant, and in the remaining 5 percent, either both sides develop simultaneously to have dual function or, more rarely, the right side alone becomes highly developed, with full dominance. This speech area is responsible for formation of words by exciting simultaneously the laryngeal muscles, respiratory muscles, and muscles of the mouth. The motor areas for controlling hands are also dominant in the left side of the brain in about 9 of 10 persons, thus causing right-handedness in most people. Although the interpretative areas of the temporal lobe and angular gyrus, as well as many of the motor areas, are usually highly developed in only the left hemisphere, these areas receive sensory information from both hemispheres and are also capable of controlling motor activities in both hemispheres. For this purpose, they use mainly fiber pathways in the corpus callosum for communication between the two hemispheres. This unitary, cross-feeding organization prevents interference between the two sides of the brain; such interference could create havoc with both mental thoughts and motor responses. This close relation probably results from the fact that the first introduction to language is by way of hearing. Many other types of interpretative capabilities, some of which use the temporal lobe and angular gyrus regions of the opposite hemisphere, are retained. Thus, even though we speak of the "dominant" hemisphere, this dominance is primarily for languagebased intellectual functions; the so-called nondominant hemisphere might actually be dominant for some other types of intelligence. Yet efforts to show that the prefrontal cortex is more important in higher intellectual functions than other portions of the brain have not been successful. The prefrontal areas do, however, have less definable but nevertheless important intellectual functions of their own. These functions can best be explained by describing what happens to patients in whom the prefrontal areas have become damaged, as follows. For instance, when we read a book, we do not store the visual images of the printed words but instead store the words themselves or their conveyed thoughts, often in language form. This procedure was performed by inserting a blunt, thin-bladed knife through a small opening in the lateral frontal skull on each side of the head and slicing the brain at the back edge of the prefrontal lobes from top to bottom.
Buy procardia with visa
Inflammation usually increases cell membrane permea bility cardiovascular emergencies chapter 4 order procardia 30 mg without prescription, allowing sodium and other ions to diffuse into the interior of the cell, with subsequent osmosis of water into the cells. One reason for this phenomenon is that hypernatremia promotes intense thirst and stimu lates secretion of antidiuretic hormone, which both protect against a large increase in plasma and extracel lular fluid sodium, as discussed in Chapter 29. However, severe hypernatremia can occur in patients with hypotha lamic lesions that impair their sense of thirst, in infants who may not have ready access to water, in elderly patients with altered mental status, or in persons with diabetes insipidus. Correction of hypernatremia can be achieved by administering hypoosmotic sodium chloride or dextrose solutions. However, it is prudent to correct the hyperna tremia slowly in patients who have had chronic increases in plasma sodium concentration because hypernatremia also activates defense mechanisms that protect the cell from changes in volume. These defense mechanisms are opposite to those that occur for hyponatremia and consist of mechanisms that increase the intracellular concentra tion of sodium and other solutes. There are two general causes of extracellular edema: (1) abnormal leakage of fluid from the plasma to the interstitial spaces across the capillaries, and (2) failure of the lymphatics to return fluid from the interstitium back into the blood, often called lymphedema. The most common clinical cause of interstitial fluid accumulation is excessive capillary fluid filtration. Factors That Can Increase Capillary Filtration To understand the causes of excessive capillary filtration, it is useful to review the determinants of capillary filtra tion discussed in Chapter 16. In most instances, edema occurs mainly in the extracellular fluid compartment, but it can involve intra cellular fluid as well. The rise in protein concentration raises the colloid osmotic pressure of the interstitial fluid, which draws even more fluid out of the capillaries. Blockage of lymph flow can be especially severe with infections of the lymph nodes, such as occurs with infec tion by filaria nematodes (Wuchereria bancrofti), which are microscopic, threadlike worms. The adult worms live in the human lymph system and are spread from person to person by mosquitoes. People with filarial infections can have severe lymphedema and elephantiasis and men can have swelling of the scrotum, called hydrocele. Lymphatic filariasis affects more than 120 million people in 80 countries throughout the tropics and subtropics of Asia, Africa, the Western Pacific, and parts of the Caribbean and South America. Lymphedema can also occur in persons who have certain types of cancer or after surgery in which lymph vessels are removed or obstructed. For example, large numbers of lymph vessels are removed during radical mastectomy, impairing removal of fluid from the breast and arm areas and causing edema and swelling of the tissue spaces. A few lymph vessels eventually regrow after this type of surgery, and thus the interstitial edema is usually temporary. Congenital absence or abnormality of lym phatic vessels Edema Caused by Heart Failure. The following is a partial list of conditions that can cause extracellular edema by these two types of abnormalities: I. Failure of venous pumps (a) Paralysis of muscles (b) Immobilization of parts of the body (c) Failure of venous valves C. In heart failure, the heart fails to pump blood normally from the veins into the arteries, which raises venous pressure and capillary pressure, causing increased capillary filtra tion. In addition, the arterial pressure tends to fall, causing decreased excretion of salt and water by the kidneys, which causes still more edema. Thus, in persons with untreated heart failure, all these factors acting together cause serious generalized extracellular edema. In patients with leftsided heart failure but without significant failure of the right side of the heart, blood is pumped into the lungs normally by the right side of the heart but cannot escape easily from the pulmonary veins to the left side of the heart because this part of the heart has been greatly weakened. Consequently, all the pulmo nary vascular pressures, including pulmonary capillary pressure, rise far above normal, causing serious and life threatening pulmonary edema. When untreated, fluid accumulation in the lungs can rapidly progress, causing death within a few hours. Most sodium chloride added to the blood remains in the extracellular compartment, and only small amounts enter the cells. Therefore, in kidney diseases that compromise urinary excretion of salt and water, large amounts of sodium chloride and water are added to the extracellular fluid. Most of this salt and water leaks from 317 Unit V the Body Fluids and Kidneys the blood into the interstitial spaces, but some remains in the blood. The main effects of this are (1) widespread increases in interstitial fluid volume (extracellular edema) and (2) hypertension because of the increase in blood volume, as explained in Chapter 19. As an example, in children who have acute glomerulonephritis, in which the renal glomeruli are injured by inflammation and therefore fail to filter adequate amounts of fluid, serious extracel lular fluid edema also develops; along with the edema, severe hypertension usually develops. This leads to increased capillary filtration throughout the body and extracellular edema. One of the most important causes of decreased plasma protein concentration is loss of proteins in the urine in certain kidney diseases, a condition referred to as nephrotic syndrome. Multiple types of renal diseases can damage the membranes of the renal glomeruli, causing the membranes to become leaky to the plasma proteins and often allowing large quantities of these proteins to pass into the urine. When this loss exceeds the ability of the body to synthesize proteins, a reduction in plasma protein concentration occurs. Serious generalized edema occurs when the plasma protein concentration falls below 2. Cirrhosis of the liver is another condition that causes a reduction in plasma protein concentration. Cirrhosis means development of large amounts of fibrous tissue among the liver parenchymal cells. One result is failure of these cells to produce sufficient plasma proteins, leading to decreased plasma colloid osmotic pressure and the generalized edema that goes with this condition. Another way liver cirrhosis causes edema is that the liver fibrosis sometimes compresses the abdominal portal venous drainage vessels as they pass through the liver before emptying back into the general circulation. Blockage of this portal venous outflow raises capillary hydrostatic pressure throughout the gastrointestinal area and further increases filtration of fluid out of the plasma into the intraabdominal areas. When this occurs, the combined effects of decreased plasma protein concentra tion and high portal capillary pressures cause transuda tion of large amounts of fluid and protein into the abdominal cavity, a condition referred to as ascites. Failure negative pressure range, (2) the ability of lymph flow to increase 10 to 50fold, and (3) "washdown" of interstitial fluid protein concentration, which reduces interstitial fluid colloid osmotic pressure as capillary filtration increases. Safety Factor Caused by Low Compliance of the Interstitium in the Negative Pressure Range In Chapter 16, we noted that interstitial fluid hydrostatic pressure in most loose subcutaneous tissues of the body is slightly less than atmospheric pressure, averaging about -3 mm Hg. Therefore, in the negative pressure range, the compliance of the tissues, defined as the change in volume per millimeter of mercury pressure change, is low. How does the low compliance of the tissues in the negative pressure range act as a safety factor against edema When intersti tial fluid hydrostatic pressure increases, this increased pressure tends to oppose further capillary filtration. Therefore, as long as the interstitial fluid hydrostatic pres sure is in the negative pressure range, small increases in interstitial fluid volume cause relatively large increases in interstitial fluid hydrostatic pressure, opposing further filtration of fluid into the tissues. Because the normal interstitial fluid hydrostatic pres sure is -3 mm Hg, the interstitial fluid hydrostatic pres sure must increase by about 3 mm Hg before large amounts of fluid will begin to accumulate in the tissues. Therefore, the safety factor against edema is a change of interstitial fluid pressure of about 3 mm Hg. Once interstitial fluid pressure rises above 0 mm Hg, the compliance of the tissues increases markedly, allowing large amounts of fluid to accumulate in the tissues with relatively small additional increases in interstitial fluid hydrostatic pressure. Thus, in the positive tissue pressure range, this safety factor against edema is lost because of the large increase in compliance of the tissues. Importance of Interstitial Gel in Preventing Fluid Accumulation in the Interstitium. Importance of the Proteoglycan Filaments as a "Spacer" for the Cells and in Preventing Rapid Flow of Fluid in the Tissues. That is, the fluid is bound in a proteoglycan mesh work so that there are virtually no "free" fluid spaces larger than a few hundredths of a micrometer in diameter. The importance of the gel is that it prevents fluid from flowing easily through the tissues because of impediment from the "brush pile" of trillions of proteoglycan fila ments. Also, when the interstitial fluid pressure falls to very negative values, the gel does not contract greatly because the meshwork of proteoglycan filaments offers an elastic resistance to compression. In the negative fluid pressure range, the interstitial fluid volume does not change greatly, regardless of whether the degree of suction is only a few millimeters of mercury negative pressure or 10 to 20 mm Hg negative pressure. In other words, the compliance of the tissues is very low in the negative pres sure range. By contrast, when interstitial fluid pressure rises to the positive pressure range, there is a tremendous accumula tion of free fluid in the tissues. In this pressure range, the tissues are compliant, allowing large amounts of fluid to accumulate with relatively small additional increases in interstitial fluid hydrostatic pressure.
