
Discount 5mg prochlorperazine fast delivery
Over the past several years medicine you cannot take with grapefruit purchase prochlorperazine 5 mg without a prescription, use of pneumococcal conjugate vaccines has significantly reduced the rate of disease. Legionellosis has been on the rise in the United States since 2000, with 6000 cases reported in 2015; while some of this increase is attributable to increased use of diagnostic testing and better reporting, this also likely reflects a true increase in the frequency of disease. Examples of this phenomenon include human disease associated with avian influenza viruses, especially highly pathogenic avian influenza A(H5N1) and avian influenza A(H7N9),127,128 and extensively drug-resistant tuberculosis129 (see "Antimicrobial Resistance" earlier). Acute respiratory tract infection constitutes a broad category of diseases that include infections of both the upper and lower respiratory tracts, such as acute pharyngitis, epiglottitis, bronchitis, pneumonia, and influenza. Globally, 42% of all deaths from lower respiratory tract infections (mostly due to pneumonia) occur in children younger than 5 years of age. The four most common etiologies were Streptococcus pneumoniae, Haemophilus influenzae, respiratory syncytial virus, and influenza. In many regions, the burden has increased in people older than age 65 and because of growing and aging populations, global mortality due to lower respiratory tract infections has remained relatively stable. The outbreak, which involved substantial transmission in health care settings, was contained within 4 months of recognition, primarily through the employment of standard public health measures such as droplet and contact precautions in hospitals, community isolation, and quarantine. Illness has been characterized by severe respiratory distress and pneumonia often requiring mechanical ventilation, and some cases have been accompanied by renal insufficiency. Both cases were health care providers who had lived and worked in Saudi Arabia, where they are believed to have been infected. Both had traveled to the United States, and both were hospitalized in the United States and later discharged after fully recovering. The largest outbreak outside of the Arabia peninsula occurred in the Republic of Korea in 2015, with 186 cases and 36 deaths; 184 of the patients were infected nosocomially. Infection can produce either upper or lower respiratory tract infection and in children is often accompanied by wheezing. Influenza viruses have a segmented genome-eight separate genes coding for one or more proteins necessary for constructing a functional influenza virus. Influenza virus nomenclature categorizes influenza A viruses into subtypes on the basis of the antigenic characteristics of these two surface proteins. This characteristic of influenza viruses allows them to find ways to evade host immunity, returning each year to infect the same population repeatedly. Influenza A viruses have three main reservoirs: birds, humans, and swine; however, transmission is also maintained in dogs, horses, bats, and other mammals. Over the last 100 years, influenza A viruses circulating among humans have been limited to H1N1, H2N2, and H3N2 subtypes. Domestic poultry, such as chickens, ducks, and geese, also maintain circulation of influenza A viruses. This protein signature is associated with increased replication of the virus and systemic spread with multiorgan failure, presenting as higherseverity illness in domestic poultry and sometimes in infected mammals. Compared with humans and birds, swine have a much greater ability to be infected with either bird or human influenza A viruses due to the presence of a more diverse set of receptors in the swine respiratory tract. Avian influenza A viruses have a strong affinity for receptors with an (2,3)-linked sialic acid, which are more abundant on bird respiratory and enteric epithelial cells. Human influenza A viruses prefer receptors with an (2,6)-linked sialic acid, which are more abundant in the upper respiratory tract of humans. Swine, however, have both type of receptors, allowing infection with either bird or human influenza A viruses. Because of this, swine have been called the "mixing vessel" for influenza A viruses. More importantly, pigs can be coinfected with avian, Part I Basic Principles in the Diagnosis and Management of Infectious Diseases Human Bocaviruses Reservoirs of Influenza A Emerging Influenza Viruses Influenza viruses are one of the most challenging infectious diseases for clinicians, researchers, and public health and agricultural officials. The viruses are constantly changing, spread rapidly in populations, and can cause significant illness. Of the four main types of influenza viruses-A, B, C, and D-only influenza A viruses circulate in multiple animal and human reservoirs, sometimes spilling over to cause illness in other species and adapting and exchanging genes to generate new influenza viruses with potential to cause pandemics. This significant adaptive change in influenza A viruses when a human is infected is referred to as antigenic shift, and represents a fitness advantage that may allow the virus to transmit efficiently in humans, potentially emerging to cause a global pandemic. In the last 100 years, there have been four antigenic shift events leading to reassortant influenza A viruses that caused pandemics in humans. The most devastating of these pandemics was the 1918 H1N1 "Spanish" pandemic, which caused at least 50 million deaths globally. The pandemic emerged during World War I and impacted young adults disproportionately, ultimately killing more soldiers than died in combat. Most likely, this virus moved back and forth between humans and swine, becoming increasingly adapted to humans189,190 and eventually achieved sustained and efficient human-to-human transmission, thus igniting the pandemic in 2009. Early detection of these viruses is a critical component of pandemic preparedness and response. The expanding number of pig and poultry operations, including live animal markets, that are located in or near densely populated areas provides new opportunities for human exposure to avian influenza A viruses. In addition, international air travel now makes it possible to travel to almost any place on the globe within the incubation period of influenza virus infection. This convergence of humans, animals, and transportation may be an important reason for the significant rise in human cases due to two novel influenza A viruses of recent concern: H5N1 and H7N9. In May 1997, a young child in Hong Kong developed acute febrile respiratory illness and died of multiorgan failure. Overall, 18 virologically confirmed A(H5N1) virus infections with 6 deaths were reported in Hong Kong during 1997. Each year, sporadic human infections have been reported in some countries, typically during colder temperature months. Although human infections have generally declined since 2006, a surge in A(H5N1) virus infections occurred in Egypt during 2014 and 2015. Graph includes avian H4, H5, H6, H7, H9, and H10; and swine H1 and H3 (not pH1N1). Influenza at the animal-human interface: a review of the literature for virological evidence of human infection with swine or avian influenza viruses other than A(H5N1). In the early spring of 2013, the first three human infections with A(H7N9) virus were identified in eastern China. This Asian-lineage A(H7N9) virus was a reassortant virus with the H7 and N9 genes derived from other avian influenza A viruses and six genes derived from A(H9N2) viruses circulating among poultry. During the spring of 2013, most A(H7N9) virus infections were sporadic and occurred in older men with a recent history of exposure to poultry in urban areas of eastern China. The reasons for the dramatic reduction in human cases are unknown, although multiple factors may have contributed, including widespread H5/H7 vaccination of commercial sector poultry in China. Swine influenza A viruses that have infected humans are referred to as "variant viruses" and denoted with "v" after the subtype. The high error rate of virus replication, coupled with the ability to exchange gene segments among avian, swine, and human viruses, allows the virus to continue evading host immunity, to spill over and cause disease across species, and to periodically introduce pandemic viruses into the human population. Maintaining surveillance in humans, birds, and swine is critical to identifying, preventing, and controlling emerging novel influenza A viruses with pandemic potential. Enteric diseases encompass all the attributes of emerging and reemerging infectious diseases, and their emergence and spread is influenced by microbial, human, and environmental factors, as discussed previously. Enteric pathogens are constantly changing in their ability to survive in their reservoir environments and in their ability to infect and harm the human host. In addition to increased international travel and mass production (including huge farms and dairies), increased international trade in food is expanding the number and types of foods that may serve as vehicles for foodborne diseases. For example, in the United States, imports of fruit and nuts more than doubled and imports of fish and seafood increased over 60% during 1998 to 2007. Other factors that facilitate the spread of enteric diseases include wars, social disruption, and associated population migrations, which often result in the breakdown of basic public health and health care services, leading to reemergence of ancient scourges such as cholera, with devastating consequences. Weather events can also increase human exposures to enteric pathogens, especially with the dramatic destruction and flooding from hurricanes and typhoons associated with waterborne diseases. These effects were evident in an outbreak of Vibrio parahaemoliticus infections due to contaminated oysters in 2004.
Order cheap prochlorperazine on line
Emerging viral diseases from a vaccinology perspective: preparing for the next pandemic 911 treatment for hair cheap 5 mg prochlorperazine with mastercard. The global One Health paradigm: challenges and opportunities for tackling infectious diseases at the human, animal, and environment interface in low-resource settings. Lessons learned from research and surveillance directed at highly pathogenic influenza A viruses in wild birds inhabiting North America. Rat fall surveillance coupled with vector control and community education as a plague prevention strategy in the West Nile Region, Uganda. Genomic epidemiology: whole-genome-sequencing-powered surveillance and outbreak investigation of foodborne bacterial pathogens. The Global Public Health Intelligence Network and early warning outbreak detection: a Canadian contribution to global public health. Involvement of gut microbiome in human health and disease: brief overview, knowledge gaps and research opportunities. Part I Basic Principles in the Diagnosis and Management of Infectious Diseases 15 Bioterrorism: An Overview Noreen A. Borioa Exposures to biological agents, such as microbes and toxins, are usually unintentional. Notably, these agents can be used as weapons to cause intentional harm to humans, animals, or plants as well as to contaminate the environment. Unlike nuclear, radiologic, chemical, and explosive threat agents, the diseases and conditions caused by biological agents as well as their treatment could be encountered during the practice of medicine. Similarly, the surveillance of and response to these agents is within the purview of many public health systems. This feature of encountering these biological agents in practice highlights the importance of understanding which of the biological agents are associated with the greatest health consequences (Table 15. Although there is no universally accepted definition of these three terms, the underlying motivation and objectives for intentional use of these biological agents has been suggested as a way to distinguish biological warfare, bioterrorism, and biocrimes. Descriptions of each may help guide clinicians and public health professionals in determining when interactions with law enforcement personnel may be anticipated. A biocrime, on the other hand, occurs when a biological agent is used by a person or group against an individual or small group, often for revenge or extortion, in the absence of an underlying ideology; the perpetrator(s) are often believed to have underlying psychopathology. Biological warfare occurs when a state actor uses a biological agent as part of its armamentarium in waging war. Importantly, biological agents have been used intentionally in all three settings-bioterrorism, biocrime, and biological warfare. It began in 1915, with documented use of anthrax against animals being shipped for use by Allied forces. Although the Geneva Protocol, which had been officially agreed to by 137 State Parties as of March 15, 2013,10 banned the use of biological weapons, it did not proscribe the research, production, or possession of biological weapons, and many of the State Parties to the treaty reserved the right to retaliate in kind should they or their allies be attacked. In addition, no provision was made for verification, and compliance was voluntary. A number of countries agreeing to the Geneva Protocol began or continued biological weapons programs after signing the treaty, including Canada, France, Germany, Italy, Japan, Poland, the United Kingdom, and the Soviet Union (see Table 15. The United States did not ratify the Geneva Protocol until 1975, after it had ended its biological weapons program. Its biological weapons program-organized at its Unit 731 and based in Harbin, China-used multiple biological agents and employed more than 3000 scientists plus smaller units at a number of other sites in China, which were under Japanese occupation. Use by the governments of Rhodesia and South Africa were internally directed against insurgents seeking regime change. They may not use any means of delivery of such agents or toxins for hostile purposes and must take necessary measures to prohibit or prevent such activities in their territories. Further, State Parties should destroy or divert to peaceful purposes all agents, toxins, weapons, equipment, and means of delivery and not transfer to any recipient or in any way assist, encourage, or induce to manufacture or otherwise acquire biological agents, toxins, weapons, equipment, or means of delivery. In 1973, a large, science-based research and development program to address offensive issues related to biological agents, 184 called Biopreparat, was created in the civilian sector, complementary to a less sophisticated program in the Ministry of Defense. It was reportedly able to produce upwards of 20 tons of smallpox virus annually, primarily for delivery via intercontinental ballistic missile as a strategic weapon. Subsequently, Iraq admitted to "a far more extensive biological warfare programme" than previously admitted, including weaponization. The biological agents were delivered in food in nine (60%) of the confirmed intentional incidents, five (33%) by injection, and one by an unknown delivery mechanism; all but one of the perpetrators was trained or practicing in a health-related field (Table 15. Although there were no deaths among the 751 persons who became ill, 45 were hospitalized. It was not until 1 year after the outbreak that dissension among the perpetrators led law enforcement officials to discover that the contamination was deliberate with the ultimate goal of disrupting the local election. They present a unique, complex, and growing challenge with respect to the development and use of biological weapons. During the 20th century, confirmed or threatened use of biological weapons against humans was more common by criminals than by terrorists. Notably, some experts classify it as a crime rather than an act of terrorism due to assessed motivation by the alleged perpetrator. Physicians provided the initial evaluation that led to diagnosis and needed treatment. Public health professionals responded to the situation with the outbreak investigative skills needed. When a deliberate etiology of the outbreak was suspected, law enforcement expertise was required to identify the perpetrator(s) and to stop further attacks, if possible. Over the subsequent 8 years, law enforcement carried out the so-called Amerithrax Investigation. Bioterrorism and Biocrimes: the Illicit Use of Biological Agents since 1900 (Revised). The third list of biological agents, the Select Agents and Toxins List, are those that are monitored by the mandated Federal Select Agent Program. The scrutinized agents may be possessed or transferred by nonclinical locations, such as research laboratories, and have the potential to pose a severe threat to the public, animal, or plant health if released. This is a regulatory program with established regulations; program personnel inspect locations in possession of these agents, set compliance standards, and conduct investigations when noncompliance is suspected. A proposed impact measure helps to put the outcomes of biological weapons use in perspective. Using this impact typing system, deliberately caused bioterrorism incidents and biocrimes have fallen into the lowest impact tier, Individual level (type A), affecting less than 1000 persons. It reflects the 1999 initial assessment undertaken by a multidisciplinary group of experts and the Working Group on Civilian Biodefense consensus panel. One was a threat assessment to evaluate the likelihood that a particular intentional bioterrorism event will occur given estimated capabilities and intentions of the potential perpetrator(s). The risk assessment is used to estimate the probability of adverse public health impacts from each biological agent under specified exposure conditions, to identify the production capabilities needed, and to examine person-to-person transmissibility, the estimated public level of concern/ panic should there be a bioterrorism event involving each pathogen, and if special preparation is needed, and at what level, in advance of a bioterrorism event to minimize casualties. Category A agents are those with the highest priority, specifically defined as those that (1) are most likely to have the highest consequence to individuals and populations due to their ease of dissemination or ease of person-to-person transmission, (2) may result in high mortality rates and have the potential for a major public health impact, (3) may cause associated public panic, and (4) require special actions to attain public health preparedness. The Category B agents are considered to have lower associated adverse health outcomes. This category also captures the possibility that a newly emerging infection or condition could be used in nefarious ways. The definition of synthetic biology is often debated but generally is thought to encompass either the redesign of existing natural biological systems or the design and creation of new biological systems or parts for useful purposes. The power of synthetic biology is exemplified in the creation and then production of synthetic artemisinin for treatment of Plasmodium falciparum following shortage of the naturally grown Artemisia annua plant in Asia.
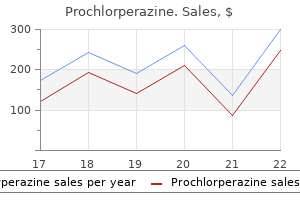
| Comparative prices of Prochlorperazine | ||
| # | Retailer | Average price |
| 1 | Barnes & Noble | 237 |
| 2 | Ahold USA / Royal Ahold | 812 |
| 3 | Stater Bros. Holdings | 369 |
| 4 | H-E-B | 797 |
| 5 | Nordstrom | 494 |
| 6 | Alimentation Couche-Tard | 991 |
| 7 | Publix | 690 |
| 8 | Save Mart | 425 |
Order discount prochlorperazine line
With the initial cloning of human papillomaviruses and bovine papillomavirus 1 (cf treatment pancreatitis purchase 5 mg prochlorperazine with mastercard. Notably, John Kreider, Mary Kay Howett and colleagues at Penn State-Hershey Medical Center were able to transform human cervical epithelial cells with papillomavirus recovered from a cervical condyloma and experimentally generate dysplastic changes comparable to those defining clinical lesions [97]. Interestingly, the viral genome was disrupted at the end of the "early region" into two portions in each integrated copy. These findings stimulated intense research activities as to how the viral genes, E6 and E7, might provoke such devastating consequences for the infected host. These findings offered a rational explanation as to why only certain papillomaviruses can trigger the pathogenesis of human cancer. The research culminated in the discovery of the significance of the p53 protein with his post-doctoral researcher David Lane [126] and further work on tumorigenesis, oncogenes, and cancer control. The transforming genes of bovine papillomavirus are E7 and E5, while the cancer drivers of certain rabbit papillomaviruses are E7 plus an alternative reading frame that overlaps the E6 gene. Rather the viral sequences are lost and the tumor is presumably a result of a "hit and run" mechanism in which the initiating events included viral caused mutagenesis of host cell regulatory genes (Hasche et al. Thus there is no single pathway or process by which different animal or human papillomaviruses trigger carcinogenesis. Over the years, comprehensive understanding of the interaction partners of E6 and E7 and the mechanisms of oncogenic action have been achieved (cf. Without understanding the normal functions of the E6 and E7 proteins in the viral reproductive cycle, it would be difficult to explain their aberrant actions during neoplastic progression and cancer (for review, see [149]). Papillomavirus infections can introduce foreign viral genes into epithelial cells that may become integrated and become part of the genome of the emerging cancer cells. These genes clearly have oncogenic activities and largely explain the complex biology of these cancers caused by a virus that is not able to reproduce and multiply once integrated and partially deleted. In his textbook [158] he wrote that, "in one state in Australia detained promiscuous girls are under legal compulsion to submit to bacteriological examination of the vagina and opportunity was taken with permission to undertake colposcopy/biopsy. Coppleson took biopsies and commented that he was observing "the initial moment of the complicated sequence leading to the development of squamous cancer. Results showed that in the early post menarcheal years mucus had "open channels" that possibly facilitated entry of a coital mutagen to the epithelium. Epidemiologic, social, and behavioral data pointed to our hypothesis [162] of the "high risk male" whose partners were at an increased risk of developing cervical cancer. To the left is the cover of a meeting held in the Cold Spring Harbor Laboratory in 1986 and the inset shows some of the attendees. Cancer etiology: variation in cancer risk among tissues can be explained by the number of stem cell divisions. Fatti statistici relativi alle malattie cancerose che servivono di base alle poche cose dette dal dottore. A radioautographic analysis of cellular proliferation in dysplasia and carcinoma in situ of the uterine cervix. Cytological changes preceding the appearance of in situ carcinoma of the uterine cervix. The significance of noncondylomatous wart virus infection of the cervical transformation zone: a review with discussion of two illustrative cases. A transplantable rabbit carcinoma originating in a virus-induced papilloma and containing the virus in masked or altered form. Conditional neoplasms and subthreshold neoplastic states: a study of the tar tumors of rabbits. Induction of tumors in domestic rabbits with nucleic acid preparations from partially purified Shope papilloma virus and from extracts of the papillomas of domestic and cottontail rabbits. A vaccination procedure which increases the frequency of regressions of Shope papillomas of rabbits. Isolation and propagation of human papillomavirus type 16 in human xenografts implanted in the severe combined immunodeficiency mouse. Isolation of three novel rat and mouse papillomaviruses and their genomic characterization. An experimental study of the relationship between Trichomonas vaginalis and dysplasia in the uterine cervix. Perspectives on the epidemiology of cervical cancer with special reference to the herpesvirus hypothesis. Antibody to genital herpes simplex virus: association with cervical atypia and carcinoma in situ. A comparison review of key epidemiological studies in cervical cancer related to current searches for transmissible agents. Comparative study of cultured Burkitt tumor cells by immunofluorescence, autoradiography, and electron microscopy. Nearest neighbour base sequence analysis of the deoxyribonucleic acids of a further three mammalian viruses: Simian virus 40, human papilloma virus and adenovirus type 2. Chromatin-like structures obtained after alkaline disruption of bovine and human papillomaviruses. Epidermodysplasia verruciformis as a model in studies on the role of papovaviruses in oncogenesis. Molecular cloning and biochemical characterization of human papillomavirus 3a, 8, 10, and 12 genomes. Characterization of two types of human papillomaviruses in lesions of epidermodysplasia verruciformis. The primary structure and genetic organization of the bovine papillomavirus type 1 genome. Detection and mapping of conserved nucleotidic sequences between the genomes of human papillomavirus 1a and bovine papillomavirus 1 by electron microscope heteroduplex analysis. Evidence of an association between subclinical papillomavirus infection and cervical malignancy. Morphological transformation in vivo of human uterine cervix in papillomavirus from condylomata acuminata. Enzymatic amplification of beta-globin genomic sequences and restriction site analysis for diagnosis of sickle cell anemia. Use of polymerase chain reaction amplification for the detection of genital human papillomaviruses. Detection of human papilloma virus in paraffin-embedded tissue using the polymerase chain reaction. The use of general primers in the polymerase chain reaction permits the detection of a broad spectrum of human papillomavirus genotypes. Structure and transcription of human papillomavirus sequences in cervical carcinoma cells. Correlation of modified human papilloma virus early gene expression with altered growth properties in C4-1 cervical carcinoma cells. The E7 open reading frame of human papillomavirus type 16 encodes a transforming gene. Cellular targets of the oncoproteins encoded by the cancer associated human papillomaviruses. In vitro biological activities of the E6 and E7 genes vary among human papillomaviruses of different oncogenic potential. Inhibition of cervical carcinoma cell line proliferation by the introduction of a bovine papillomavirus regulatory gene. An emerging issue in oncogenic virology: the role of beta human papillomavirus types in the development of cutaneous squamous cell carcinoma. Human papillomavirus type 16 alters human epithelial cell differentiation in vitro. Production of human papillomavirus and modulation of the infectious program in epithelial raft cultures.
Order discount prochlorperazine
T cells specific for tetanus toxoid peptides pair up with this polysaccharide-specific B cell and provide the necessary help to drive isotype switching and formation of memory cells medications prescribed for anxiety purchase prochlorperazine 5mg free shipping. The first signal comes from antigen, and the second signal usually comes from T cells. Some antigens can provide a type of second signal to the B cell without the participation of T cells. Their repetitive structure and flexible backbone allow them to interact with multiple membrane IgM molecules that aggregate into a single focus and deliver a potent signal to the B cell. These B cells respond to bloodborne pathogens such as bacteria that are trapped by macrophages located around the marginal zone. Because they do not require the participation of T cells, marginal-zone B cells provide a pseudoinnate response to bacteremia by quickly releasing IgM antibodies. Sequestration of antigen deprives B cells of the activating signal they require to survive. Because they recognize epitopes unique to a particular Downregulation of Antibody Production 46 clone, they can modulate B cells in a highly selective manner. Antiidiotypes interacting with membrane IgM, before the immature B cell expresses IgD, can suppress antibody production. With persistent activation, T cells begin to express both Fas and its ligand, FasL. Reciprocal interactions between activated T cells expressing both Fas and FasL lead to mutual apoptotic death. Finally, as antigen becomes scarce, fewer T cells and B cells receive the antigen signals necessary for continued activation and survival. The "usual" B cells discussed until now are called B2 cells to distinguish them from B1 cells. B1 cells appear to regenerate continuously in the periphery rather than in the bone marrow. Their antigen-binding clefts are encoded directly by germline sequences without further modification, and the antigens they recognize tend to be microbial polysaccharides and effete or denatured host proteins. Antibodies produced by B1 cells may serve a housekeeping function by facilitating the clearance of cellular debris and denatured proteins. These antibodies are present in low levels even in individuals who have not been deliberately immunized. Animals that have been raised in "germ-free" environments have low levels of circulating natural antibodies that react with a variety of commensal organisms, suggesting that B1 cells may be part of the endogenous immune system. Hypersensitivity reactions are immune responses that cause tissue injury and morbidity for the host. In some cases, an aberrant autoimmune response is specifically directed to host antigens and host cells. In many other cases, an exuberant immune response to an infectious agent injures host cells that are innocent bystanders. The Gell and Coombs classification divides hypersensitivity reactions into four types based on their underlying mechanism of action. Although few diseases can be uniquely attributed to a single Gell and Coombs class, the classification scheme is a useful foundation for understanding pathogenetic mechanisms. It should also be noted that the term hypersensitivity reaction is often used, in a potentially paradoxical manner, to describe defense mechanisms that are actually beneficial to the host. They also produce leukotrienes, prostaglandins, cytokines such as tumor necrosis factor-, and proteases. Local release of mast cell contents causes wheal-and-flare reactions, urticaria, and hives. Massive simultaneous degranulation of large numbers of mast cells throughout the body causes anaphylaxis, resulting in reduced blood pressure, a loss of fluids through permeable vessel walls, and constriction of smooth muscle. Mast cells can be degranulated by cross-linking of IgE antibodies held in FcRs on the mast cell surface. This can be carried out by antigens with multiple repetitive epitopes or by antibodies to the IgE molecules or the FcR. Opioids and contrast dyes can also degranulate mast cells without acting through IgE or the FcR. As a result, the responses they trigger are referred to as anaphylactoid reactions. Fragments from the third and fifth complement proteins (C3a and C5a) can also degranulate mast cells, and these molecules are referred to as 47 anaphylatoxins. The clinician struggling to deal with IgE-mediated reactions to harmless substances such as penicillin or ragweed recalls with difficulty that type I responses have a beneficial role in the defense against intestinal parasites. The B cell displays those diverse peptides, in large numbers, along with costimulatory signals presumably induced by a coexistent inflammatory stimulus. Although tissues decorated with complexes are too large to be ingested, the phagocytes nonetheless try, and in the process they release injurious proteolytic enzymes and proinflammatory cytokines. Immune complexes can also activate complement, which deposits on the cell surface. Host cells usually protect themselves from complement attack with proteins that block formation of the membrane attack complex and accelerate the inactivation of complement components. However, when immune complexes activate complement through the classical pathway, the host may be unable to produce inactivator proteins at a sufficient rate. For example, complexes of antibodies and hepatitis antigens cause vasculitis when they deposit in blood vessel walls and glomerulonephritis when they deposit in the kidney. When antibody is in excess, antigen is covered with antibody, and complexes are still small. However, when antigen and antibody are present in near-equivalence, antibodies will cross link to contiguous antigen molecules and the ensuing lattice forms a large immune complex. Antibodies with low affinities release antigen quickly and tend to form small complexes regardless of their relative abundance. Rheumatoid factors are antibodies that react with human (autologous) IgG and are a frequent component of immune complexes. Cryoglobulinemia is a vasculitis triggered by complexes of rheumatoid factors and IgG that deposit preferentially in sites of reduced body temperature. The mechanism is thought to be bystander activation of B cells, because few of the antibodies produced are specific for antigens associated with the infectious agent. Epstein-Barr virus is also associated with elevated immunoglobulin levels, because the virus infects and activates a wide array of B cells, which then produce antibodies of diverse (polyclonal) specificities. Cells decorated with antibodies may be lysed by activated complement or phagocytosed by neutrophils or monocyte-macrophages. For example, autoimmune hemolytic anemia can be caused by antibodies to red blood cell antigens. For example, patients with antibodies to penicillin can develop hemolytic anemia when penicillin binds to their red blood cells. It may be helpful, at this point, to review the mechanisms that prevent the development of autoimmunity and how these processes can be circumvented. Early in their development, B cells are induced to undergo apoptosis or to become unresponsive if they encounter cognate antigen. This reaction occurs during the window of vulnerability that persists while immature B cells express IgM and before they express IgD. Such B cells are likely to be situated in the bone marrow, or in early transition into the periphery, and any antigens they encounter are likely to be self-antigens. As B cells move into the periphery, where they are likely to encounter foreign antigen, they lose their IgD and interaction with antigen becomes an activating, life-prolonging stimulus. However, central induction of tolerance appears to be only partially effective, because virtually all people have circulating B cells that can be driven, in vitro, to produce antibodies reactive with autoantigens. It is important to recognize that mature B cells in germinal centers undergo somatic hypermutation and generate new antigen-binding sites well after they are no longer vulnerable to the regulatory mechanisms that apply to pre-B cells in the bone marrow.
Buy 5mg prochlorperazine amex
Vancomycin trough concentration as a predictor of clinical outcomes in patients with Staphylococcus aureus bacteremia: A meta-analysis of observational studies treatment dynamics florham park purchase prochlorperazine 5 mg free shipping. Systematic review and metaanalysis of vancomycin-induced nephrotoxicity associated with dosing schedules that maintain troughs between 15 and 20 milligrams per liter. A quasi-experiment to study the impact of vancomycin area under the concentration-time curve-guided dosing on vancomycinassociated nephrotoxicity. Comparison of acute kidney injury during treatment with vancomycin in combination with piperacillin-tazobactam or cefepime. Risk of acute kidney injury in patients on concomitant vancomycin and piperacillin-tazobactam compared to those on vancomycin and cefepime. Azithromycin-related ototoxicity in patients infected with human immunodeficiency virus. Clinically significant hearing loss in renal allograft recipients treated with intravenous erythromycin. Inappropriate prescribing of aminoglycosides: Risk factors and impact of an antibiotic control team. Comparison of the prevalence of convulsions associated with the use of cefepime and meropenem. Cefepime neurotoxicity in the intensive care unit: A cause of severe, underappreciated encephalopathy. Linezolid-associated peripheral and optic neuropathy, lactic acidosis, and serotonin syndrome. Serotonergic and adrenergic drug interactions associated with linezolid: A critical review and practical management approach. Serotonin toxicity associated with the use of linezolid: A review of postmarketing data. The removal of antibiotics in critically ill patients is complex, influenced by factors such as the mode of renal support used, if any; drug characteristics such as solubility, molecular weight, and protein binding; and patient characteristics, including cardiovascular status and infection. Pharmacokinetics and pharmacodynamics of antibiotics in critically ill acute kidney injury patients. Mandell, Douglas and Bennetts Principles and Practice of Infectious Disease (8th ed. As with fever, leukocytosis may be due to non-infectious or infectious causes and is not, per se, indicative of an infectious etiology. Since leukocytosis is reflective of stress due to any cause, most cases of leukocytosis with a left shift are due to non-infectious events/causes of fever [4,5]. While antibiotics may penetrate into a phlegmon before the abscess is fully formed/walled off, few antibiotics are able to penetrate into the abscess and sterilize the abscess cavity. Therefore, antibiotics are adjunctive in the treatment of abscesses, and care requires adequate abscess drainage. First, colonization may rarely precede infection (the exception and not the rule), but nearly always, there is no progression from colonization to infection. Second, it is more difficult to eradicate colonization (no inflammatory component) than infection. The fever response to appropriate antimicrobial therapy has diagnostic importance, i. Dosing should be with the highest recommended dose while avoiding toxicity to minimize resistance potential. If the antibiotic selected has the appropriate spectrum (by body site) and is being dosed optimally, then consideration should be given to re-assessment of the interpretation of in vitro susceptibility data (organism/pathogen specific) vs. Even though all streptococci are routinely reported as aminoglycoside "susceptible," aminoglycosides. When penicillin or ampicillin is given with gentamicin, the synergistic combination is clinically effective [8]. Therefore, in vitro susceptibility may be misleading for non-bloodstream infections. Stenotrophomonas maltophilia Erysipelothrix rhusiopathiae Mycobacterium tuberculosis Streptococci, Salmonella sp. The other important determinant of tissue penetration is lipid solubility, as measured by the volume of distribution (Vd). First, when treating pneumonia, virtually all antibiotics achieve therapeutic levels in the lungs. However, daptomycin lung levels are therapeutic, but the drug is inactivated by lung surfactant. It is a common misconception that aminoglycosides do not penetrate the lung well, but they do. The effect of local pH on antimicrobial activity should be considered when no other explanation suffices to explain antibiotic failure, particularly in the treatment of cystitis and prostatitis. The activity of some antibiotics is enhanced in an acid urine (and decreased in an alkaline urine), while others are most active in an alkaline pH (and decreased in an acid urine). Inadequate urinary levels (with renal eliminate antibiotics) may result from decreased renal function. First, chronic prostatitis has no inflammatory component to facilitate antibiotic penetration. Second, the prostate is a multiseptate lipid gland laden, which prevents therapeutic levels of water-soluble antibiotic (Vd ~ H2O). Drug fever should be suspected when fever is accompanied by relative bradycardia and the patient looks "relatively well" (in light of underlying pathology). Leukocytosis with a left shift may lead the unwary away from considering the diagnosis of drug fever. Otherwise-unexplained relative bradycardia (provided patient is not on a -blocker, verapamil, or diltiazem or has a pacemaker rhythm) is the cardinal clue to drug fever. The diagnostic test is to discontinue the most likely medication causing drug fever, and the temperature will decrease to normal after 3 days [1,8] (Tables 38. Note: Relative bradycardia refers to heart rates that are inappropriately slow relative to body temperature (pulse must be taken simultaneously with temperature elevation). If more than one drug may be responsible for the drug fever, discontinue one at a time to identify the medication responsible. Clinical failure with and without empiric atypical bacteria coverage in hospitalized adults with community-acquired pneumonia: A systematic review and meta-analysis. Predictors of polymyxin B treatment failure in gram-negative healthcare associated infections among critically ill patients. Fever is an important host defense mechanism and provides diagnostic clues to the etiology of the fever. The usual approach to fever continues to be reflex pan culture of blood, wounds, respiratory secretions, and urine, without regard, for carefully considering clues indicating the likely source of the fever (infectious and non-infectious) [5,8]. Tigecycline dosing is critical in preventing tigecycline resistance because relative resistance is, in part, concentration dependent. Nitrofurantoin safety and effectiveness in treating acute uncomplicated cystitis in hospitalized adults with renal insufficiency: Antibiotic stewardship implications. Severe adenoviral pneumonia in an immunocompetent host with persistent fevers treated with multiple empiric antibiotics for presumed bacterial co-infection: An antibiotic stewardship perspective of de-excalation derailed. Predicting in vivo effectiveness from in vitro susceptibility: A step closer to performing testing of uropathogens in human urine. Effectivenes of achievable urinary concentrations of tetracyclines against "tetracycline-resistant" pathogenic bacteria. Serum versus urinary antimicrobial concentration in cure of urinary tract infections. Index Note: Page numbers in bold and italics refer to tables and figures, respectively. Background Cytogenetics studies the architecture of chromosomes in cells and their role in heredity.
Syndromes
- Eat a healthy diet full of fruits and vegetables, which contain important vitamins and minerals, especially vitamin E.
- Watery nasal drainage (rhinorrhea)
- Toxins and poisons
- Uterine fibroids
- Seizures
- Feeling tense, restless, or frustrated
Buy prochlorperazine in india
Comparison of 30-min and 3-h infusion regimens for imipenem/cilastatin and for meropenem evaluated by Monte Carlo simulation treatment lead poisoning buy cheap prochlorperazine on line. Clinical outcomes with extended or continuous versus short-term intravenous infusion of carbapenems and piperacillin/ tazobactam: a systematic review and meta-analysis. Steady-state plasma and intrapulmonary concentrations of levofloxacin and ciprofloxacin in healthy adult subjects. Effect of procalcitoninguided antibiotic treatment on mortality in acute respiratory infections: a patient level meta-analysis. Source control in the management of severe sepsis and septic shock: an evidence-based review. Predictors of efficacy and health resource utilization in treatment of complicated intra-abdominal infections: evidence for pooled clinical studies comparing tigecycline with imipenem-cilastatin. Inadequate source control and inappropriate antibiotics are key determinants of mortality in patients with intraabdominal sepsis and associated bacteremia. Septic shock attributed to Candida infection: importance of empiric therapy and source control. Mortality rate and antibiotic resistance in complicated diverticulitis: report of 272 consecutive patients worldwide: a prospective cohort study. Effectiveness and safety of short-course vs long-course antibiotic therapy for group a beta hemolytic streptococcal tonsillopharyngitis: a meta-analysis of randomized trials. Short-term late-generation antibiotics versus longer term penicillin for acute streptococcal pharyngitis in children. Antibiotics and the human gut microbiome: dysbioses and accumulation of resistances. Clinical relevance of bacteriostatic versus bactericidal mechanisms of action in the treatment of gram-positive bacterial infections. Comparison of tigecycline with imipenem/cilastatin for the treatment of hospital-acquired pneumonia. Effects of clindamycin in combination with rifampicin on clindamycin-susceptible and clindamycin-resistant Staphylococcus aureus. Linezolid as rescue treatment for left-sided infective endocarditis: an observational, retrospective, multicenter study. Daptomycin compared to standard therapy for the treatment of native valve endocarditis. Clindamycinrifampin combination therapy for staphylococcal periprosthetic joint infections: a retrospective observational study. Successful treatment of necrotizing fasciitis and streptococcal toxic shock syndrome with the addition of linezolid. Influences of linezolid, penicillin, and clindamycin, alone and in combination, on streptococcal pyrogenic exotoxin a release. Effectiveness of clindamycin and intravenous immunoglobulin, and risk of disease in contacts, in invasive group A streptococcal infections. Macrofilaricidal activity after doxycycline treatment of Wuchereria bancrofti: a double-blind, randomised placebo-controlled trial. Combination antibiotic therapy versus monotherapy for Pseudomonas aeruginosa bacteraemia: a meta-analysis of retrospective and prospective studies. Colistin alone versus colistin plus meropenem for treatment of severe infections caused by carbapenem-resistant gram-negative bacteria: an open-label, randomised controlled trial. Effect of empirical treatment with moxifloxacin and meropenem vs meropenem on sepsis-related organ dysfunction in patients with severe sepsis: a randomized trial. Mortality associated with bacteremia due to colistin-resistant Klebsiella pneumoniae with high-level meropenem resistance: importance of combination therapy without colistin and carbapenems. Predictors of mortality in bloodstream infections caused by Klebsiella pneumoniae carbapenemase-producing K. Suppression of emergence of resistance in pathogenic bacteria: keeping our powder dry, part 1. Suppression of emergence of resistance in pathogenic bacteria: keeping our powder dry, part 2. Position paper: recommended design features of future clinical trials of anti-bacterial agents for community-acquired pneumonia. Recommended design features of future clinical trials of antibacterial agents for hospital-acquired bacterial pneumonia and ventilator-associated bacterial pneumonia. Acute endocarditis due to Staphylococcus aureus successfully treated with penicillin. Bacteremia owing to gram-negative bacilli: experiences in the treatment of 137 patients in a 15-year period. Optimisation of empirical antimicrobial therapy in patients with haematological malignancies and febrile neutropenia (how long study): an open-label, randomised, controlled phase 4 trial. Part I Basic Principles in the Diagnosis and Management of Infectious Diseases 107. Opal and Aurora Pop-Vicas Genetic variability is essential for microbial evolution to occur. The fitness of a microorganism depends on its capacity to adapt to changing environmental conditions. Point mutations may occur at a nucleotide base pair (bp), which is referred to as microevolutionary change. These mutations can alter enzyme substrate specificity or the target binding site of an antimicrobial agent, interfering with its activity. These large-scale alterations of the bacterial genome are frequently generated by specialized genetic elements such as integrons, transposons, or insertion sequences, which have the capacity to move and insert independently throughout the bacterial genome. Large-scale transfer of resistance genes for different classes of antibiotics as a single event also occurs among enteric bacteria within the gut microbiota by conjugal transfer of large R plasmids. Whole-scale acquisition of many antibiotic-resistance genes at the same time is referred to as "evolution by quantum leaps,"5 and provides a major advantage for bacteria residing in patients receiving multiple courses of different classes of antibiotics. When an antibiotic-resistance gene evolves, this gene can spread between bacteria by transformation, transduction, conjugation, or transposition. Favored clones of bacteria may proliferate in the microbiota of patients who receive antibiotics. Therefore, antibiotics left in the microenvironment by dormant bacteria are avoided as potentially toxic to competitors yet serve as a ready source of carbon (food) for the next generation of the antibiotic-producing bacterial strain once the growth phase begins again. Environmental levels of multiple classes of antimicrobial agents are now so common in soil and water samples that multiple bacterial genera have strains that subsist entirely on antibiotics as their sole carbon source. Aquatic environments are particularly rich with bacterial populations replete with antibiotic-resistance genes. These resistant populations proliferate and spread antibiotic-resistance genes vertically to subsequent generations and horizontally to susceptible strains of related bacteria, or even between species or different genera. This allows favorable, but sometimes "costly," antibiotic-resistance genes to be held in reserve in the absence of antibiotic selection pressure yet express their resistance potential on reexposure to antibiotics. Maintaining the fidelity of the host genome, while permitting limited variation by microevolutionary and macroevolutionary changes, allows pathogens to strike a balance between genomic stability and plasticity in rapidly changing microenvironments. This observation led to a classification scheme of plasmids based on incompatibility (Inc) groups. Plasmids must also retain a set of genes that facilitate their stable maintenance in host bacteria. Some small plasmids may be able to transfer to other bacteria via the use of the conjugation apparatus provided by coresident conjugative plasmids or even conjugative transposons. Many plasmidencoded functions enable bacterial strains to persist in the environment by resisting noxious agents, such as heavy metals. Mercury released from dental fillings may increase the number of antibiotic-resistant bacteria in the mouth. This explains the problem of lingering persistence of resistance genes in patients, even after good antibiotic stewardship programs are working to curtail unnecessary antibiotic use. Readers interested in practical recommendations to limit the spread of antibiotic-resistance genes in clinical settings are referred to Chapters 14, 51, and 298. Transposons differ from insertion sequences in that they encode functional genes that mediate a recognizable phenotypic characteristic, such as an antibioticresistance marker. This generally results in transfer of homologous genes located on the chromosome by recombination enzymes (RecA). Self-transferable plasmids mediate direct contact by forming a mating bridge between cells.
Cheap 5 mg prochlorperazine otc
In parallel medications when pregnant purchase genuine prochlorperazine line, anecdotal reports of rare malignant conversion of genital warts into squamous cell carcinomas were reported [4]. These studies were carried out in two countries with contrasting rates of cervical cancer, Colombia having an incidence rate of about eight times higher than Spain. For invasive cancer, the adjusted odd ratios and 95% confidence intervals were 46. Subsequently, several studies have been published on the distribution of types in cervical lesions. These estimates were similar to the most updated systematic review reported by de Martel and colleagues [19]. The main studies that provided these epidemiological evidence have been summarized in this chapter. A type-by-type evaluation proves to be very difficult and stretches epidemiology to its limits and carcinogenicity is solely based on phylogenetic relatedness. These vaccines have been shown to have high efficacy for the prevention of high-grade precancerous lesions of the cervix. Public heath action can only be advocated after rigorous evaluation of the scientific evidence based both on laboratory and epidemiological studies. From causality to prevention - the example of cervical cancer: my personal contribution to this fascinating history. Comparison of ViraPap, e Southern hybridization, and polymerase chain reaction methods for human papillomavirus identification in an epidemiological investigation of cervical cancer. Epidemiologic classificae e tion of human papillomavirus types associated with cervical cancer. Human papillomavirus type distribution in 30,848 invasive cervical cancers worldwide: variation by geographical region, histological type and year of publication. Human papillomavirus genotype attribution in invasive e cervical cancer: a retrospective cross-sectional worldwide study. Worldwide human papillomavirus e genotype attribution in over 2000 cases of intraepithelial and invasive lesions of the vulva. Large contribution of human papillomavirus in vaginal neoplastic lesions: a worldwide study in 597 samples. Classification of weakly carcinogenic human papillomavirus types: addressing the limits of epidemiology at the borderline. The first is based on establishing long-term persistence and production of viral progeny only when the survival of the host organism is jeopardized. This is epitomized by bacteriophages, such as the lambda phage, which inserts its genome into the bacterial chromosome during its lysogenic, dormant phase. The activation of the lytic, virulent phase of the life cycle is engaged under conditions of cellular stress and involves excision of the phage genome and synthesis of infectious phage particles. The infected cell undergoes lysis and the newly synthesized phage progeny can infect a new, healthy host cell [1]. After the initial infection, they establish life-long latency in immune privileged, postmitotic cells with occasional bouts of reactivation and virus production, when the host organism encounters various forms of stress [2]. A second strategy is to establish a productive infection with ample production and release of infectious viral progeny. This requires vigorous suppression of host immune responses but allows for infection of new hosts before the original infective lesion is eliminated by the immune system or the demise of the host. Many papillomaviruses cause large, productive lesions, warts, which, at least in an immunocompetent host organism, spontaneously regress at a high rate. Viral genomes are shown as circles and infectious viral progeny is represented by stars. In order to limit the risk of viral genome loss during mitosis, they constrain division of infected basal epithelial cells and viral proteins which may trigger innate and adaptive immune responses that cause the elimination of persistently infected cells, are expressed at low levels. Despite the fact that all papillomaviruses face similar challenges for completing their replicative life cycles in squamous epithelia and that their genomic organization is remarkably conserved, they evolved strikingly different replication strategies that all appear to be evolutionarily successful. The different replication strategies may reflect whether their life cycles evolved to favor long-term persistent infections as opposed to generating large infectious lesions that facilitate efficient infection of new hosts. We will also discuss how this strategy creates cellular vulnerabilities that provide unique opportunities for developing therapeutic approaches. In addition, expression of cytokines and chemokines is activated, which can trigger recruitment of antigen presenting cells that elicit induction of effective adaptive immune responses [6,7]. Nuclear entry of the virus-containing transport vesicles is during mitosis after breakdown of the nuclear matrix and involves vesicle transport on microtubules [11]. This effectively shields the invading virus from recognition by intracellular innate immune surveillance mechanisms. Since the nuclear envelope breaks down during mitosis, every round of cell division poses a danger of viral genome loss. To minimize the possibility that, after the nuclear envelope has re-formed, viral genomes end up in the cytoplasm where they may be sensed and trigger innate immune responses, the viral E2 protein tethers viral genomes to mitotic chromosomes [37,38]. Basal epithelial cells can divide asymmetrically, giving rise to one basal and one differentiating suprabasal daughter cell. Hence, it will be interesting to determine whether there are mechanisms that regulate equal or unequal genome partitioning as a means to controlling the persistent versus infectious phases of the viral life cycle. Epithelial stem cells, for example, only divide infrequently and when there is a need to regenerate the basal layers of the epithelium in response to obliterative trauma. Interestingly, E6 and E7 have each been reported to modulate gene expression and/or steadystate levels of proteins that control aspects of cellular stemness [49,50]. Senescent cells remain metabolically active but have terminally withdrawn from the cell division cycle [60]. Growth factor deprivation creates a situation of conflicting growth signals; a pro-proliferative stimulus generated by oncogene expression conflicts with an antiproliferative signal due to lack of extrinsic growth factors. E7 also induces synthesis of supernumerary centrosomes, which can give rise to multipolar mitoses and aneuploidy. The expression pattern of the different isoforms is cell type specific, but expression increases in response to interferon [94]. Deamination of cytidine residues can give rise to Cto-T and C-to-G mutations within the genome of the invading pathogen but also within the genome of the host cell. All papillomaviruses need to reprogram terminally differentiated postmitotic epithelial cells to support viral progeny synthesis. Activation and pathogenic manipulation of the sensors of the innate immune system. Human papillomavirus-driven immune deviation: challenge and novel opportunity for immunotherapy. Cruising the cellular highways: How human papillomavirus travels from the surface to the nucleus. Toll-like receptors: Important immune checkpoints in the regression of cervical intra-epithelial neoplasia 2. The human papillomavirus type 16 E6 and E7 oncoproteins independently induce numerical and structural chromosome instability. Implication for the E7-mediated immune evasion mechanism in cervical carcinogenesis. Human papillomavirus 16 E6 oncoprotein binds to interferon regulatory factor-3 and inhibits its transcriptional activity. The human papillomavirus E7 oncoprotein abrogates signaling mediated by interferon-alpha. Asymmetric cell divisions promote stratification and differentiation of mammalian skin. A discrete population of squamocolumnar junction cells implicated in the pathogenesis of cervical cancer. Changing stem cell dynamics during papillomavirus infection: potential roles for cellular plasticity in the viral lifecycle and disease. Synergism with germ line transcription factor Oct-4: viral oncoproteins share the ability to mimic a stem cell-specific activity. Human papillomavirus carcinogenesis: an identity crisis in the retinoblastoma tumor suppressor pathway. Ink4a/Arf and oncogeneinduced senescence prevent tumor progression during alternative colorectal tumorigenesis.
Purchase cheapest prochlorperazine and prochlorperazine
Exfoliative dermatitis and StevensJohnson syndrome are rare forms of allergic reactions to penicillins medicine 219 buy cheap prochlorperazine 5mg online. The morbilliform eruptions that develop after penicillin therapy probably are due to IgM antibodies to the benzyl penicilloyl hapten and to the minor determinants. In many patients these rashes disappear, even if the penicillin is continued, owing to the production of IgG-blocking antibody. There is a risk, however, that the rash could progress to generalized desquamation. Another allergic reaction to penicillins is that of allergic vasculitis with the development of cutaneous and visceral lesions similar to that found with polyarteritis nodosa. The clinical syndrome is one of fever, macular rash, eosinophilia, proteinuria, eosinophiluria, and hematuria. Initially the reaction is one of nonoliguric renal failure with a decrease in CrCl and a rise in serum urea nitrogen and serum creatinine concentrations. Abnormalities in liver function test results, such as elevation of the alkaline phosphatase and aminotransferase levels, have been reported, most often after the use of oxacillin and flucloxacillin. Penicillin G remains the primary agent for treatment of infections due to Streptococcus pyogenes, penicillin-susceptible strains of Streptococcus pneumoniae, and penicillin-susceptible strains of S. None of the semisynthetic penicillins or agents in other classes has been shown to be more effective. This hierarchy of activity of the penicillins is maintained against penicillin-resistant strains of S. Neisseria gonorrhoeae strains frequently are resistant to penicillin, which is no longer recommended for treatment of gonorrhea. Puerperal infections due to anaerobic streptococci or group B streptococci (Streptococcus agalactiae), as well as genital clostridial infections, are treated with penicillin G. Infections produced by anaerobic oral microbiota, including gram-positive and gram-negative cocci and actinomycetes, can be treated with penicillin G, although penicillin-resistant strains of Prevotella melaninogenica that produce -lactamase are encountered. Discontinuation of the penicillin results in the return of renal function to normal in most cases. Administration of massive doses of any penicillin may result in hypokalemia, owing to the large dose of nonreabsorbable anion presented to the distal renal tubules, which alters hydrogen ion excretion and secondarily results in potassium loss. Among the penicillinase-resistant penicillins, nafcillin may carry higher risk of hypokalemia than oxacillin. The ureidopenicillins, particularly piperacillin, are active against many strains of Klebsiella spp. However, the activity of piperacillin against many of the gram-negative species, such as P. Intrapartum prophylaxis with penicillin is recommended at the time of labor or rupture of membranes to prevent early-onset S. Amoxicillin is recommended as a single 2-g (adults) or 50-mg/kg (children) oral dose for prophylaxis of bacterial endocarditis among those with the highest risk of adverse outcome. Because penicillin G is unstable in acid, penicillin V or amoxicillin should be used for oral administration. It is available as sterile dry powder in vials containing 5 or 20 million units per vial. Repository penicillins provide tissue depots from which the drug is absorbed over hours in the case of penicillin G procaine or over days in the case of benzathine penicillin G. Penicillin G procaine is a mixture of equal-molar parts of procaine and penicillin G. The use of this suspension delays the peak of activity to 2 to 4 hours after injection and provides serum and tissue levels for 24 hours. To increase the peak level, it is necessary to use two body sites, as is done in the treatment of gonorrhea, for example, with 2. Benzathine penicillin G is a repository form of penicillin G that combines penicillin G and dibenzylethylenediamine. Serratia marcescens Morganella morganii Pseudomonas aeruginosa Acinetobacter baumannii Providencia spp. The usual dosage for children is 25 to 50 mg/kg/day and for adults is 1 to 4 g/day in three or four divided doses. Penicillin V can be substituted for penicillin G in most situations in which it is reasonable to treat an infection by the oral route. However, penicillin V is less active than penicillin G against Haemophilus and Neisseria spp. None are active against methicillin-resistant staphylococci, high-level penicillinresistant streptococci, enterococci, L. Methicillin Methicillin (2,6-dimethoxyphenylpenicillin) was the first of several penicillinase-resistant penicillins developed. Methicillin is the least active of the penicillinase-resistant penicillins by weight; it is acid labile and therefore can be administered only parenterally; and it is more likely to cause interstitial nephritis. They are active against methicillin-susceptible strains of staphylococci; penicillin-susceptible strains of streptococci, Nafcillin (2-ethoxy-1-naphthylpenicillin) has more intrinsic activity than methicillin against susceptible organisms. For adults a dosage of 125 to 500 mg every 6 hours can be given, depending on the severity of the infection. Flucloxacillin and dicloxacillin are similar in pharmacokinetics, activity, and indications. Flucloxacillin is available as a sodium salt in an oral suspension (125 mg/5 mL or 500 mg/5 mL), capsules (250 and 500 mg), and in powder form for reconstitution for parenteral administration. The usual dosage of nafcillin is 6 to 12 g/day, depending on the severity of the infection, and 100 to 200 mg/kg/day for children. For practical purposes the activity of aminopenicillins is virtually identical to that of penicillin G against penicillin-susceptible organisms, except that aminopenicillins are slightly more active against enterococci. Ampicillin is moderately well absorbed after oral administration, but peak levels are delayed and lowered if it is ingested with food. Ampicillin is well distributed to body compartments and after parenteral administration achieves therapeutic concentrations in cerebrospinal, pleural, joint, and peritoneal fluids in the presence of inflammation. The drug undergoes enterohepatic circulation, and significant levels appear in bile and stool. Peritoneal dialysis is ineffective in removing the drug, but hemodialysis removes approximately 35% in a 4-hour period. The half-life of ampicillin is about 3 hours during continuous venovenous hemofiltration. Ampicillin is available for oral use as the sodium salt as 250-mg or 500-mg capsules and oral suspensions of 125 or 250 mg/5 mL. For most indications, oral ampicillin has been abandoned in favor of oral amoxicillin because of the greater bioavailability of the latter. Ampicillin is effective for upper and lower respiratory tract infections caused by S. Dicloxacillin and flucloxacillin yield the highest total drug serum concentrations, but because of differences in protein binding, free-drug concentrations are similar for all three compounds (see Table 20. The isoxazolyl penicillins undergo some metabolism but are excreted primarily by the kidney, with slight biliary excretion. Oxacillin undergoes more rapid degradation in the body than does cloxacillin or dicloxacillin. The adult dosage is 6 to 12 g/day, and for children it is 100 to 200 mg/kg/day given every 4 to 6 hours. Oxacillin may be associated with a higher incidence of hepatotoxicity and rash than nafcillin or other antistaphylococcal agents. The dosage for children is 50 to 100 mg/kg/day given as four equal doses, and the dosage for adults is 1 to 2 g/day given as four equal doses. Dosage varies with the age of the patient, the status of renal function, and the severity of the disease.

Order 5 mg prochlorperazine visa
The pulmonary alveoli are just a ventilated part medicine vs dentistry purchase prochlorperazine pills in toronto, like in incomplete atelectasis around a pleural effusion or pulmonary consolidation. In pulmonary parenchyma consolidation areas and with other areas of incomplete atelectasisdbronchopneumonia. When air and a small quantity of inflammatory exudates coexist inside the pulmonary alveoli, such as in pulmonary congestion and the resorption phase of consolidation pneumonia. The pathological noises originate in the alveoli, bronchi, pulmonary cavities, and pleural cavity. This produces a condition that will produce the appearance of these added sounds: crackles. Pulmonary congestion Red phase of hepatization Gray phase of hepatization Resorption phase Crackles appear in the congestion phase and resorption phase of pneumonia because in these phases there exist specific conditions (air and liquid inflammatory exudates) inside the pulmonary alveoli. Fine crackles are discontinuous, high-pitched, and similar to the sound of rubbing a lock of hair in front of the ear or the noise from walking on snow. Crackles can be heard in the late phase of inspiration (at the end of inspiration) in pneumonia, fibrosis, or atelectasis. Compared with fine crackles they are louder, stronger, and higher, and have a low pitch and last longer. Coarse crackles are formed inside the pulmonary alveoli if there exist conditions for developing this type of sound. The condition exists when air and a small quantity of liquid such as transudate, exudate, or blood are inside the pulmonary alveoli. This liquid, at the end of expiration, when the alveoli are collapsed, will make the alveoli walls stick together. Opening of the walls of the alveoli on inspiration due to the passing of air that invades the pulmonary alveoli, at the end of inspiration, will produce audible sounds. These sounds are audible at the end of inspiration, like crackling equal to each other. The sounds can be reproduced by rubbing a strand of hair in front of the ear or when we walk on fresh snow. Crackles can be heard well, after the patient performs a few deep respiration movements (inspirations and expirations) and then coughs. After these maneuvers, at the end of expiration, the walls of the pulmonary alveoli stick 4. Coarse crackles appear in the following diseases: pneumonia in the phase of pulmonary congestion, pneumonia in the phase of resorption, bronchopneumonia, acute left ventricular failure, acute pulmonary edema, pulmonary infarction consecutive to pulmonary embolism, and pulmonary atelectasis. In the second phase of pneumoniadthe consolidation phasedall the alveoli are full of inflammatory exudates, without air inside; this is not a condition for crackles, and in this phase we hear pathologic bronchial sound. The Objective Examination of the Thorax In the second phase of pneumonia, all the pulmonary alveoli are full of pulmonary exudates, without air inside, and this will not create a condition for crackles. In this phase, the consolidation area of the lobe of the lung is full of pulmonary exudates, without air inside, and works like a resonance box and facilitates the transmission of the larynxetracheal sound from the lateralecervical area of the neck to the chest wall of the thorax. This situation is pathologic and the physician will hear the bronchial sound on the chest, which is called the pathologic bronchial sound. This sound in the area of the chest is common and coincides with the consolidated lobe of the lung. This represents an advanced phase of pneumonia, when the patient will neglect him- or herself, and does not start antibiotic therapy on time, as early as possible, and the inflammatory exudates occupy all the pulmonary alveoli. In the end, after therapy, if the entire quantity of inflammatory exudate was resorbed and only air exists inside the pulmonary alveoli, the crackles will disappear and we will hear normal vesicular sound again. The persistence of a few crackles after the antibiotic therapy protocol signifies that inside the pulmonary alveoli a small quantity of inflammatory exudate persisted, and for this reason, we hear crackles and the pneumonia is resorbed completely. In conclusion, in bronchopneumonia many pulmonary alveoli contain air and inflammatory exudate and also inflammatory exudate is inside the small bronchi, and for this reason, after auscultation of the lung, we will detect many areas with crackles and also areas with wheeze; sometimes it can be dissemination over the total thorax. In this situation, the patient has severe dyspnea, cough, and expectoration with mucus (productive cough), and will need hospitalization because it is considered an emergency. For a patient with cardiac failure, bronchopneumonia aggravates the decompensation of the heart, and this can also induce severe cardiac arrhythmia in the context of hypoxia. Hypoxia is a very dangerous risk factor for severe arrhythmia, cardiac arrest, and sudden death. The Objective Examination of the Thorax Acute left ventricular failure represents the situation in which the left ventricle becomes insufficient; it cannot pump enough blood inside the systemic circulation and secondarily there appears stasis of the blood in the pulmonary circulation (pulmonary stasis). The pulmonary stasis will increase the hydrostatic pressure, and this determines the migration of transudate first in the interstitial space and then inside the pulmonary alveoli. This situation exists when air and fluid (pulmonary transudate) exist inside the pulmonary alveoli, which is the condition for crackles at the auscultation of the lung. Pulmonary stasis is present symmetrically at both bases of the lungs, and transudate will be present (together with air) inside the pulmonary alveoli at the level of the bases of the lungs, so the crackles will be present at both bases of the lungs. Clinically, the patient will present with nocturnal paroxysmal dyspnea and dry cough (cardiac cough of stasis) and will adopt an orthopnea position. Because of pulmonary stasis the hydrostatic pressure will increase, and transudate appears first in the interstitial space and then inside the pulmonary alveoli. At first air and transudate exist inside the pulmonary alveoli at both bases of the lungs, but if patients do not start the correct therapy and neglect themselves, the transudate will invade all the pulmonary alveoli and the alveoli will be full of fluid (transudate). The patient in acute pulmonary edema will have crackles symmetrically at both hemithoraxes; they will increase from the bottom up, which is how the transudate invades the pulmonary alveoli, so the crackles will be present in a severe form throughout the thorax. Clinically, the patient will present with an extreme form of dyspnea, cyanosis, and an orthopnea position. The Objective Examination of the Thorax Pulmonary infarction represents the necrosis of the lung consecutive to pulmonary embolism, and the complication of a deep vein thrombosis. In the preceding images we have a patient with a right deep vein thrombosis, who suffers from complication of pulmonary embolism and consecutive acute obstruction. Pulmonary infarctiond necrotic pulmonary tissuedappears with the embolus of a pulmonary artery, indicated by the triangular area on the posterior chest of the patient; it corresponds to the pulmonary lobe of the lung. In this situation, inside the pulmonary alveoli a small quantity of air and fluid consecutive to necrosis of tissue of the lung is present. In the area with pulmonary infarction crackles will be present at the auscultation of the lung and on the area of the pulmonary lobe with pulmonary infarction. This is one of the most dangerous emergencies in medical practice because without a fast and correct protocol management the patient can suffer a sudden death. The patient will have severe dyspnea, chest pain, dry cough, and specific expectoration with dark blood, with very increased viscosity and adherent to the walls of the collection receptacle. The patient has to be hospitalized immediately with arteriography, embolectomy, or thrombolytic therapy to dissolve the embolus. Young women who use contraceptive pills have a risk of developing deep vein thrombosis as a side effect of these pills, and secondarily further complications with pulmonary embolism can occur. Pregnancy poses another risk factor for women for deep vein thrombosis, pulmonary embolism, and secondary pulmonary infarction. Women can lose their life very easily in these conditions and have to be informed, as most of them do not know anything about these dangerous risks. If a woman is obese, a smoker, and over 35 years of age and takes contraceptive pills, she has many associated risk factors for deep vein thrombosis, pulmonary embolism, and consecutive pulmonary infraction. A deep vein thrombosis, syncope, and really sudden death can appear unexpectedly any time. The presence of crackles in the lung during auscultation of a patient with deep vein thrombosis can be a very dangerous sign that can suggest a pulmonary infarction. In this situation, in the area of the thorax relative to the lung with atelectasis crackles will be present at the auscultation of the lung. Crackles in atelectasis can appear without any liquid inside the alveoli, but can disappear after cough. This situation is typical when a complete obstruction of bronchi with a foreign body or a tumor inside the bronchi exists and secondarily resorption of the air from the pulmonary alveoli occurs. It is possible for them to appear inside the big or medium or small bronchi and in this condition there can be secretions inside the bronchi at these levels. The auscultation features of these rales are comparable to a sound produced when "blowing with a straw in water" as shown in the image below: these types of rales appear most commonly: small bullous rales suggesting bronchiolitis, pulmonary congestion, or resorption phase of pneumonia.
Discount prochlorperazine 5mg fast delivery
Discuss a perspective for treating patients with traditional Chinese herbal medicine medications band 5 mg prochlorperazine fast delivery, nutritional supplements, and/or pharmaceutical drugs in the recovery and prevention stages. Background Atherosclerosis is the diseased condition of the arteries around the heart and in the peripheral body. Atheroma is a soft substance made up of cholesterol and other substances found in the blood. It builds on the artery walls over decades, eventually reducing or blocking the flow of oxygenated blood. Breakage of the plaque can spill the soft sticky center content into the artery, causing cell fragments and platelets to stick to the content and form clots. Herbal, Bio-nutrient and Drug Titration According to Disease Stages in Integrative Cardiovascular Chinese Medicine. Obvious treatment principles are to balance yin and yang, clear heat, transform turbidity, expel toxins, dispel phlegm, and invigorate blood. It is a last resort effort used for end-stage diseased coronary arteries or arteries of the legs. Healthy arteries or veins are selected and harvested from other areas of the body and attached at safe distances around the diseased and narrowed arteries so that blood can bypass it and flow. Traditional Chinese medicine Traditional Chinese medicine formulas for arrhythmia Herbal medicine Yue jian cao you jiao wan Bao jian mei jian fei cha Pu ji xiao du yin wan Gan mao ling Xi huang wan Zhi gan cao decoction Shen fu decoction Gui pi decoction Action Invigorates blood, dispels phlegm Invigorates blood, dispels phlegm Clears toxic bacterial and viral heat Clears toxic bacterial and viral heat Clears heat, invigorates blood, protects the heart Recovers from illness, regulates heart functioning Recovers after an illness, warms yang Nourishes blood Nutritional supplements Alpha lipoic acid Nutritional constituents: Lipoic acid Benefits: Targets nerve cells, kidney, liver, lowers blood pressure, prevents cell damage to improve insulin use Caution: May lower blood sugar too much; avoid in pregnancy and nursing Cod liver oil Nutritional constituents: Vitamins A, D, and omega-3 fatty acids (fish oils, flax seed, primrose, borage, and flaxseed oils) Benefits: Reduces cardiometabolic risk factors, protects sudden cardiac death after myocardial infarction, reduces raised 110 Chapter 8 Atherosclerosis: the acute, chronic, recovery and prevention stages plasma triglycerides, reduces blood pressure, and ameliorates atherogenic effects Caution: High doses required for reduction of blood pressure may have side effects. Bile acid sequestrants these drugs bind to bile acids in the small intestines to lower the acid, because it requires cholesterol to create it. Reduce blood clots Antiplatelets and aspirin are blood thinners, which prevent blood from forming atheromas and other clots. Ticagrelor and prasugrel are drugs used to prevent clots from forming inside of artery stents. Drugs to reduce high blood pressure Adrenergic agent this drug is for mild hypertension and is often used with other antihypertensive drugs for more severe hypertension. Alpha blockers these drugs selectively block postsynaptic alpha1 -adrenergic receptors and lower blood pressure by dilating arterioles and veins. Chapter 8 Atherosclerosis: the acute, chronic, recovery and prevention stages 113 Angiotensin converting enzyme Inhibitors these drugs are used in patients with hypertension, chronic kidney disease, and proteinuria. They are often considered strong when used alone without a diuretic but can be combined with one. Calcium channel blockers these drugs are either dihydropyridines or nondihydropyridines. Some bind to L-type calcium channels, causing vasodilatation and a decrease in blood pressure. Acute and chronic stages Patients at risk for life-threatening symptoms associated with atherosclerosis should be treated only with western medicine methods and approaches. Nonalcoholic fatty liver disease represents a greater metabolic burden in patients with atherosclerosis: A cross-sectional study. Interleukin-12p35 deficiency reverses the Th1/Th2 Imbalance, aggravates the Th17/Treg imbalance, and ameliorates atherosclerosis in ApoE-/- mice. Endothelial dysfunction induces atherosclerosis: increased aggrecan expression promotes apoptosis in vascular smooth muscle cells. Intercepting the lipid-induced integrated stress response reduces atherosclerosis. Nicotine dependence as an independent risk factor for atherosclerosis in the National Lung Screening Trial. Introduce cardiac rhythm disease conditions as seen in integrative cardiovascular Chinese medicine 2. Traditional Chinese medicine formulas for arrhythmia Herbal medicine An xin ning xin formula Fu mai decoction Shen fu decoction Si ni decoction Wen dan decoction Ling gui shu gan decoction Xue fu zhu yu decoction Tao hong si wu decoction Zhi gan cao decoction Gui pi decoction Action Soothes the spirit Qi and blood deficiency Recovers after an illness, warms yang Warms coldness Regulates qi and transforms phlegm Phlegm retention Blood stagnation and stasis Invigorate blood Recovers from illness, regulates heart functioning Nourishes blood Cardiac rhythm diseases 155 Nutritional supplements Cod liver oil Nutritional constituents: Vitamins A, D, and omega-3 fatty acids (fish oils, flax seed, primrose, borage, and flaxseed oils) Benefits: Reduces cardiometabolic risk factors, protects sudden cardiac death after myocardial infarction, reduces raised plasma triglycerides, reduces blood pressure, and ameliorates atherogenic effects Caution: High doses required for reduction of blood pressure may have side effects Coenzyme Q10 Benefits: Heart, muscle, liver, and lungs; improves glycemic index, myocardial energy. However, when patients visit for traditional Chinese medicine practitioners, they usually do so at complicated periods of western medicine treatment. Often these patients are sent home from emergency visits without medication and a referral back to the attending physician who denies the withdrawal and effects. The weaning schedules are for curtailing or alleviating reported withdrawal symptoms such as brain zaps. Incidence, risk factors, and outcome of cardiac arrhythmia postcardiac surgery in children. Know key areas of the patients body to check for signs and symptoms during physical examination; 3. Understand the blood tests and imaging involved in monitoring heart failure; understand the basic Western medicine treatment approaches for heart failure, including pharmaceutical drugs; 5. Understand the basic traditional Chinese herbal formulas indicated for patients with heart failure; 6. Understand the nutritional supplements indicated for patients with heart failure; 7. Describe whether a basic plan including integrating herbs, nutritional supplements, and drugs is indicated for chronic patients and what the risk factors to look for are. Background Heart failure is an advanced weak condition when initially the ventricle then atria spreading to both sides can no longer efficiently pump enough blood through the body. Characteristic signs are tiredness and shortness of breath caused by fluid congestion in the lungs and lower leg, foot, and ankle edema. Common causes are hypertension, coronary artery disease, diabetes, thyroid diseases, hemochromatosis, amyloidosis, bacterial and viral infections, certain medications, and systemic immune diseases. This fluid backup can lead to scarring, which makes it more difficult for the liver to function properly. Intake of potassium far outweighs the kidneys ability to remove it, or if kidney function decreases, there can be too much potassium, and hyperkalemia may occur. Potassium and sodium concentrations play a crucial role in electric signal functioning of the hearts middle thick muscle layer, known as the myocardium. If your blood pressure is high, your heart has to work harder than it should to circulate blood throughout your body. Over time, this extra exertion can make your heart muscle too stiff or too weak to effectively pump blood. Myocarditis is an inflammation of the heart muscle most commonly caused by a virus and can lead to left-sided heart failure. Heart failure can reduce the blood flow to your kidneys, which can eventually cause kidney failure if left untreated. Regular monitoring of the blood will reflect progress or debilitation of the heart, specifically the left ventricle, and vascular system. The purpose of the tests are to measure levels in the blood in order to detect and evaluate heart failure and to help determine blood volume. It has tubes that route blood from the ventricle to the aorta to be injected out to the rest of the body. Lead wires are connected to a device to monitor the heart rate while the pacemaker emits electricity to correct the heart rate. A stent is inserted to permanently hold the artery open, then the catheter is removed. The purpose is to reduce or eliminate blood clots and to ensure that blood reaches the heart, lungs, brain, and out to the entire body. Angiotensin-receptor neprilysin inhibitors Candesartan (Atacand) Losartan (Cozaar) Sacubitril/Valsartan Valsartan (Diovan) Beta blockers See Chapter 11. Chronic stages Most patients at risk of life-threatening symptoms associated with heart failure should be treated only with western medicine methods and approaches. Another reason is because patients are likely being monitored using complicated combinations of pharmaceutical drugs and hospital visits resulting in surgical intervention. If lifestyle changes can reduce the health risk and improve and maintain quality of life for the duration, then such changes must be implemented immediately on a regimen with intervals to note progress. These patients may become indicated for the benefits of nutritional supplements and herbal medicines integrated with pharmaceutical drugs with very close observation. The herbal medicines would require careful choosing of herbs and formulated not to negatively interact with drug therapy. Two major syndromes from which the patient may benefit noticeably are hypertension and anemia.
