
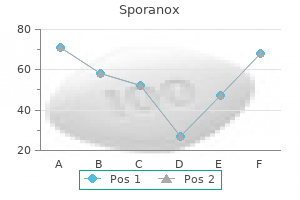
Sporanox 100 mg visa
Is dyspnea caused by chemoreceptor activation or by stimulation of receptors associated with the lung and chest wall Stretch receptors Receptors active during exercise and smoke inhalation: Exercise: Primarily muscle and joint receptors and airway stretch receptors fungus gnats peroxide order sporanox with a visa. Muscle spindles plus stretch and tension receptors in joints inform the respiratory centers about chest wall position and effort required for breathing movements. Stretch receptors are slow-adapting sensory fibers in airway walls that provide information about lung volume during inspiration. Nerve endings located in the larger conducting airways and C-fibers in alveolar walls respond to irritants, although they are also sensitive to lung inflation. Dyspnea is a term used to describe breathing discomfort, which may involve numerous physiologic and psychologic contributing factors. Although dyspnea can be induced by chemoreceptor activation alone, the other pulmonary (and systemic) receptors contribute, particularly to sensations of chest "tightness. Receptors in the alveolar walls (J receptors) respond to chemicals and alveolar inflation. Joint and muscle receptors: these measure joint position and muscle tension (spindles). They receive 90% of renal arterial blood and outnumber juxtamedullary nephrons by the same degree. Polycystic kidney disease is an inherited disorder that causes fluid-filled cysts to form within the kidney and other organs. The cysts progressively enlarge until they compromise kidney function and precipitate organ failure. The capillary walls are highly fenestrated and capillary hydrostatic pressure is relatively high to facilitate ultrafiltration. Peritubular capillaries also carry away water and other materials reabsorbed by the tubule. In practice, this means that the glomerular resistance vessels control flow through both networks. What are the four principal forces governing ultrafiltrate flow across the filtration barrier, and how are they related Capillary endothelium: has fenestrations that create a molecular filter preventing proteins of 70 nm or larger from entering the Bowman space 2. Why is inulin used in studies of clearance, and how is clearance related to filtered load Decreased inhibition of the micturition reflex due to a defect in the pontine micturition center may be one possible cause. What might the lines indicated by boxed numerals represent, and why does inulin concentration increase Transporter numbers are finite and once maximal transporter capacity (Tm) has been reached, secretion saturates. Splay reflects the presence of two or more transporter classes with differing transport maxima and also nephron heterogeneity. What is the mechanism by which glucose causes diuresis in patients with untreated diabetes mellitus The loop of Henle and collecting ducts also handle urea, but these pathways are primarily concerned with maintaining the osmotic gradients that facilitate water recovery, as discussed in the following answer. Urea recycling helps maintain and enhance the corticopapillary osmotic gradient used to recover water from the renal tubule and collecting ducts. It then enters the loop of Henle and is carried through the distal segments back to the collecting ducts. What is the main site for regulated Ca2 reabsorption, and how is reabsorption controlled What is the main site for regulated Mg2 reabsorption, and how is Mg2 reabsorption regulated Claudin-16 forms a specific pathway (paracellin-1) for paracellular Mg2 and Ca2 reabsorption in the thick ascending limb. Disrupting this pathway prevents normal Mg2 and Ca2 recovery, so urinary concentrations of both ions may rise to the point where their respective salts precipitate and grow as renal or ureteral calculi. What is the main site for regulated phosphate reabsorption, and how is it regulated What are the symptoms of severe hypophosphatemia, often associated with chronic alcoholism or excessive antacid ingestion A small percentage (10%) is recovered by the distal convoluted tubule and the rest excreted to help buffer nonvolatile acid (see 6. Symptoms include a general muscle weakness affecting the myocardium, diaphragm, gastrointestinal tract, and skeletal musculature. The distal segments normally secrete K into the tubule, but, when intake is restricted, these same segments reabsorb K. The distal segments also actively reabsorb K when intake is restricted, as discussed in the following answer. K reabsorption in the distal segments is the responsibility of -intercalated cells. When K intake is restricted, pump activity is upregulated to facilitate K reabsorption. Hypokalemia thus promotes H excretion and potentiates the metabolic alkalosis caused by H moving into cells. This movement helps buffer plasma K levels until the kidney can compensate by excreting the K excess. K secretion is regulated by aldosterone, which is released from the adrenal cortex in response to hyperkalemia. Hyperkalemia (7 mmol/L) causes skeletal muscle weakness and cardiac conduction abnormalities and dysrhythmias. The thick ascending limb absorbs Na paracellularly, and transcellularly via an apical Na -K -2Cl cotransporter. Aldosterone regulates Na reabsorption through changes in the expression levels of various Na channels and Na pumps. Liddle syndrome is characterized by increased renal Na reabsorption, causing hypertension. Some patients may also show hypokalemia and metabolic alkalosis through concurrent aldosterone-stimulated changes in K handling by principal cells. H2O is prevented from reentering the tubule, so it rejoins the circulation and is carried away by the vasa recta. The gradient is required for water recovery in the loop of Henle and the distal segments.
Sporanox 100 mg on-line
Plasma colloid oncotic pressure (c) Starling law of the capillary: Q Kf [(Pc Pif) (c if)] 1 Where Q net fluid flow fungus plant cheap 100 mg sporanox visa, Kf is a filtration constant, Pif is interstitial hydrostatic pressure, and if is interstitial colloid oncotic pressure. Blood enters and leaves glomerular capillaries at much higher pressure than c (Pc 60 mm Hg), causing massive fluid filtration into the renal tubule. The rise in c that accompanies filtration is subsequently used by the peritubular capillary network to recover fluid from the tubule lumen. In time, the tissues undergo the inflammatory hardening and thickening characteristic of elephantiasis. Metabolic: Rising metabolite levels cause resistance vessels to dilate and thereby increase blood flow to dependent capillaries. Angina pectoris is chest pain associated with inadequate O2 supply to the myocardium. Stress levels increase with flow velocity to the point where they can damage the endothelium, so vasodilation simultaneously decreases flow velocity (V Q a) and the associated shear stress and facilitates flow to tissues whose increased need for blood precipitated the velocity increase. The former reduces left ventricular afterload, whereas the latter reduces preload. What three receptor groups are involved in arterial baroreflexes, and where are the receptors located Orthostatic hypotension is a common condition among older adults and may become incapacitating if not treated. Arterial baroreceptors: Stretch-sensitive neurons in the wall of the aorta and carotid sinus are the primary pressure sensors. Cardiopulmonary receptors: Located in the low-pressure areas of the cardiovascular system (atria and pulmonary vasculature), they monitor vascular fullness. Chemoreceptors: Chemoreceptor cells located in aortic and carotid bodies monitor blood gas composition and provide information about flow rates, which reflects arterial pressure. Orthostatic hypotension is a fall in blood pressure that occurs upon standing, causing symptoms associated with cerebral hypoperfusion (dizziness, light-headedness, syncope). It reflects an impaired ability to sense and compensate for pooling of venous blood in the lower extremities upon standing, resulting in reduced ventricular preload and output. Cardiopulmonary receptors: located in atria, pulmonary artery and vein, and vena cavae; atrial receptors are sensitive to atrial wall tension (A receptors) and stretch (B receptors) 3. Chemoreceptors: located in aortic and carotid bodies; monitor blood gases Integrator Brainstem medulla oblongata contains the cardiovascular control center and is organized into three functional regions: 1. Veins: vasoconstriction forces blood toward the heart and preloads the ventricles 4. Two drugs commonly used to treat hypertension target the pathway shown by what mechanism of action Aldosterone upregulates Na channel and Na pump expression by the renal tubule, thereby increasing Na recovery. They are typically superficial veins of the lower extremities that become enlarged and tortuous. Venodilation can render their valves incompetent, which allows retrograde flow and further increases venous pressure in the lower regions. In pregnant women, the gravid uterus compresses and impedes flow through veins returning blood from the feet and legs, which increases the likelihood of varicose vein formation. Patients in congestive heart failure are typically to reduce the volume load and given a to reduce heart rate and cardiac workload. Patients in congestive heart failure are typically diuresed to reduce the volume load and given a beta blocker to reduce heart rate and cardiac workload. Hemorrhagic: Cerebral or subarachnoid hemorrhage allows blood to accumulate in the brain, compressing arterial supply vessels and impeding flow. Ischemic: Emboli or thrombi block arterial supply vessels and impair brain function. Ischemic stroke can also result from cerebral hypoperfusion caused by systemic arterial pressure inadequacy. Left ventricular infarction often damages the subendocardial regions to a greater extent than subepicardial areas. The left ventricle must generate luminal pressures that exceed aortic pressure (AoP) to eject blood. Individual myocytes contract and bear down on each other, the force increasing progressively toward the lumen. Blood is forced backward in early systole, with maximal forward flow occurring when the compressive forces are removed during diastole. Myocytes in the subendocardial regions suffer the greatest compressive forces and blood flow deprivation during systole. Therefore, myocardial recovery proceeds from the epicardium inward toward the lumen. The electrical dipole generated during this time yields an upward T wave, rather than a downward one as might be expected if recovery followed the direction of excitation. Because myocytes in the subendocardial regions suffer maximal flow deprivation during systole, they are more likely to necrose when a supply vessel is occluded. Myocytes in the subepicardial regions maintain flow throughout the cardiac cycle and are, thus, more likely to survive ischemia caused by supply vessel occlusion. Lippincott Illustrated Reviews Flash Cards: Physiology Contracting myocytes collapse vessels. Autoregulatory escape refers to the observation that while mild sympathetic stimulation curtails blood flow through splanchnic resistance vessels, the resulting rise in metabolite levels cause a reflexive dilation and normal flow resumes. Thus, local autoregulatory mechanisms allow the tissue to escape from central control. Postprandial hypotension is due to impaired baroresponses or other autonomic dysfunction that prevents normal compensation for the fall in splanchnic vascular resistance that occurs during a meal. Elderly patients commonly experience light-headedness and syncope following a meal as a result of impaired compensation. Although larger airways are wider than smaller airways, the latter are far more numerous so their collective cross-sectional area is proportionally greater. When allowed to accumulate, these inhaled irritants cause epithelial inflammation and infection, thereby predisposing smokers to coughing and bronchitis. What effect does aspirating freshwater have on pulmonary function, as seen in a case of nonfatal drowning Type I pneumocyte: creates a thin barrier between air and the pulmonary interstitium 3. The compliance effects are due to water entering the pulmonary vasculature under the influence of colloid oncotic pressure (c). Capillary hydrostatic pressure is very low in the pulmonary circulation, so c dominates. Surface tension favors alveolar collapse, but collapse concentrates the surfactant molecules which negates the effects of surface tension. Immature lungs secrete inadequate amounts of surfactant, so work of breathing is high. Such infants show signs of respiratory distress and hypoxia, including tachypnea, use of accessory respiratory muscles, and cyanosis. Surfactant Water molecules Surfactant molecules interpose themselves between water molecules and reduce surface tension. Right pleural space [Note: the right and left lungs are completely enclosed within their own pleura.
Diseases
- Escherichia coli infection
- Canine distemper
- Autoimmune hepatitis
- Al Gazali Al Talabani syndrome
- Sanderson Fraser syndrome
- M?bius axonal neuropathy hypogonadism
- Neuropathy hereditary with liability to pressure palsies
- Toxopachyoteose diaphysaire tibio peroniere
- MRKH Syndrome (M?llerian agenesis)
Buy discount sporanox 100 mg on-line
In addition to removing pathogens and necrotic debris fungus spots on skin buy sporanox 100mg with visa, macrophages take up and process microbes and present antigens to lymphocytes. These cells can also differentiate into dendritic cells, which are highly efficient antigen-presenting cells. Keywords: Congestive heart failure, heart failure cells 38 the answer is E: Phagocytosis. The peripheral blood smear shows a large, agranular cell with a markedly indented nucleus. The nuclear indentation is filled with membranes of the Golgi apparatus and centrioles. Monocytes exit the circulation and migrate into all tissues and organs to become resident macrophages. In response to inflammatory mediators, they also accumulate at sites of acute and chronic inflammation. Macrophages recognize, internalize, and digest foreign materials, microorganisms, and cellular debris. None of the other mechanisms of inflammation describe the primary function of macrophages. Asthma is a chronic lung disease caused by increased responsiveness of the airways to a variety of stimuli. Bronchial hyperresponsiveness in asthma is believed to be an inflammatory reaction to diverse stimuli, either extrinsic Blood and Hematopoiesis. Histologic examination of lung from a patient who died in status asthmaticus often shows increased numbers of eosinophils. Eosinophils participate in allergic responses, and their peripheral blood count may be elevated in patients with severe asthma. The peripheral blood count of the other cells would not be expected to change significantly in patients with bronchial asthma. The peripheral blood smear shows a large lymphocyte and a basophilic granulocyte (arrow, shown on the image). Basophils and tissue mast cells express cell surface receptors for the Fc domain of IgE. When IgE-primed basophils and mast cells encounter multivalent antigens, their Fc receptors are clustered in the plane of the membrane. This clustering event triggers degranulation and the release of a variety of inflammatory mediators. Histamine is a primary mediator of increased vascular permeability during inflammation. Histamine binds specific H1 receptors in the vascular wall, inducing endothelial cell contraction, gap formation, and local edema. Basophils do not have cell surface receptors for the other immunoglobulin classes. A thrombus is an aggregate of clotted blood that contains platelets, fibrin, and trapped blood cells. Detachment and movement of a thrombus through the circulatory system (arterial or venous) is referred to as thromboembolism. Collagen (choice A), elastin (choice B), and laminin (choice E) are extracellular matrix proteins. Keratin (choice D) is an intermediate filament protein synthesized by epidermal cells of the skin, nails, and hair. A specific fraction of HbA in circulating erythrocytes is modified by the addition of carbohydrate. This glycosylated subtype of hemoglobin (hemoglobin A1c) is measured routinely to monitor the overall degree of hyperglycemia that occurred during the preceding 6 to 8 weeks. Nonenzymatic glycosylation (glycation) of hemoglobin is irreversible, and the level of hemoglobin A1c, therefore, serves as a marker for glycemic control. Glycemic control is essential, because complications of diabetes are related to the severity and chronicity of hyperglycemia. Megakaryocytes in the bone marrow mature into multilobed giant cells by a number of endomitotic cell divisions. After reaching a certain size and ploidy, megakaryocyte cytoplasm is released into bone marrow sinusoids in long, plateletcontaining ribbons. After their release from the bone marrow, platelets circulate with a life span of about 10 days. They help maintain the integrity of the vascular endothelium by initiating thrombosis and delivering growth factors that stimulate tissue regeneration and repair. Platelets can be observed in a peripheral blood smear (examined at high magnification) as small (2 to 3 m) anucleate particles. Platelets can be readily observed in the blood smear shown for Questions 6 and 38). None of the other cells undergo endomitotic divisions or appear as multinucleated giant cells. The blood smear displays elliptical erythrocytes, as well as a normal segmented neutrophil. Neutrophils are the most abundant leukocyte present in the peripheral blood (40 to 73 relative %). None of the other cells display the distinctive polymorphonuclear morphology of segmented neutrophils. The recognition, binding, and internalization of pathogens by phagocytes are greatly enhanced by coating the pathogens with specific plasma components, particularly immunoglobulins and the C3b fragment of complement. The clinical and laboratory data suggest that this patient has a systemic blood infection. Septicemia (bacteremia) denotes the clinical condition in which bacteria are found in the circulation. This glycoprotein causes direct cytotoxic damage to capillary endothelial cells resulting in a failure to maintain adequate blood supply to the microcirculation (shock). Fever and neutrophilia are systemic manifestations of 70 Chapter 5 acute inflammation. The other diseases are not typically associated with hypotension, fever, and neutrophilia. Hemophilia A is the most frequently encountered inherited bleeding disorder (1 per 5,000 to 10,000 males). It is an X-linked recessive disorder of blood clotting that results in spontaneous bleeding, particularly into joints, muscles, and internal organs. A deficiency of the other plasma proteins would not cause a familial bleeding disorder. Identify the lines that bisect the light-stained I bands (arrows, shown in the image). Which of the following physiologic changes underlies muscle enlargement in this woman A biopsy of calf muscle reveals muscle fiber necrosis, regenerating fibers, and fibrosis. This X-linked recessive disease is caused by mutations in the gene for which of the following muscle proteins Which of the following tissues in the embryo provides stem cells for the development of limb musculature Physical examination reveals double vision (diplopia) and drooping eyelids (ptosis). The symptoms of muscle weakness in this patient are caused by autoantibodies directed against which of the following cellular components Which of the following statements describes an important feature of cardiac muscle that helps distinguish cardiac from skeletal muscle in routine H&E slide preparations These elongated cells (myocytes) are organized into parallel arrays to form muscle tissue. In skeletal muscle, a muscle fiber is a multinucleated syncytium formed by the fusion of several embryonic myoblasts. In longitudinal sections, skeletal muscle cells appear as long cylindrical fibers with multiple, long oval nuclei located at the periphery of the cells. Myofibrils (choice C) are longitudinal arrays of contractile filaments in the cytoplasm of muscle cells.
Purchase sporanox 100mg on-line
In contrast to the 2 agonists antifungal base coat sporanox 100 mg with mastercard, muscarinic antagonists do not cause tremor or arrhythmias. Prototypes and Pharmacokinetics All the corticosteroids are potentially beneficial in severe asthma (see Chapter 39). However, because of their toxicity, systemic (oral) corticosteroids (usually prednisone) are used chronically only when other therapies are unsuccessful. In contrast, local aerosol administration of surface-active corticosteroids (eg, beclomethasone, budesonide, dexamethasone, flunisolide, fluticasone, mometasone) is relatively safe, and inhaled corticosteroids have become common first-line therapy for individuals with moderate to severe asthma. Important intravenous corticosteroids for status asthmaticus include prednisolone (the active metabolite of prednisone) and hydrocortisone (cortisol). It has also been suggested that the glucocorticoid corticosteroids increase the responsiveness of adrenoceptors in the airway and they probably act by other mechanisms as well. Prototypes and Pharmacokinetics Atropine and other naturally occurring belladonna alkaloids were used for many years in the treatment of asthma but have been replaced by ipratropium, a quaternary antimuscarinic agent designed for aerosol use (see Chapter 8). This drug is delivered to the airways by pressurized aerosol and has little systemic action. The major systemic toxicities of the glucocorticoids described in Chapter 39 are much more likely to occur when systemic treatment is required for more than 2 weeks, as in severe refractory asthma. Regular use of inhaled steroids does cause mild growth retardation in children, but these children eventually reach full predicted adult stature. Although their value has been established, they are not as effective as corticosteroids in severe asthma. These drugs are orally active and have been shown to be effective in preventing exercise-, antigen-, and aspirininduced bronchospasm. Rare reports of Churg-Strauss syndrome, allergic granulomatous angiitis, have appeared, but an association with these drugs has not been established. Lipoxygenase Inhibitor Zileuton is an orally active drug that selectively inhibits 5-lipoxygenase, a key enzyme in the conversion of arachidonic acid to leukotrienes. The drug is effective in preventing both exercise- and antigen-induced bronchospasm. It is also effective against "aspirin allergy," the bronchospasm that results from ingestion of aspirin by individuals who apparently divert all eicosanoid production to leukotrienes when the cyclooxygenase pathway is blocked (Chapter 18). The toxicity of zileuton includes occasional elevation of liver enzymes, and this drug is therefore less popular than the receptor blockers. Clinical Use and Toxicity Inhaled glucocorticoids are now considered appropriate (even for children) in most cases of moderate asthma that are not fully responsive to aerosol agonists. It is believed that such early use may prevent the severe, progressive inflammatory changes characteristic of long-standing asthma. This is a shift from the earlier belief that steroids should be used only in severe refractory asthma. In such cases of severe asthma, patients are usually hospitalized and stabilized on daily systemic prednisone and then switched to inhaled or alternate-day oral therapy before discharge. In status asthmaticus, parenteral steroids are lifesaving and apparently act more promptly than in ordinary asthma. More commonly, deposition of inhaled drug droplets in the pharynx causes changes in oropharyngeal flora that result in candidiasis. Prototypes and Pharmacokinetics Cromolyn (disodium cromoglycate) and nedocromil are unusually insoluble chemicals, so even massive doses given orally or by aerosol result in minimal systemic blood levels. They are given by aerosol for asthma but are now rarely used in the United States. Mechanism of Action and Effects the mechanism of action of these drugs is poorly understood but may involve a decrease in the release of mediators (such as leukotrienes and histamine) from mast cells. Because they are not absorbed from the site of administration, cromolyn and nedocromil have only local effects. Similar actions have been demonstrated after local application in the conjunctiva and the nasopharynx for allergic IgE-mediated reactions in these tissues. Clinical Uses and Toxicity Asthma (especially in children) was the most important use for cromolyn and nedocromil. Nasal and eyedrop formulations of cromolyn are available for hay fever, and an oral formulation is used for food allergy. Cromolyn and nedocromil may cause cough and irritation of the airway when given by aerosol. She has a heart rate of 125 bpm, a respiratory rate of 40 breaths/min, and a peak expiratory flow <50% of the predicted value. After successful treatment of the acute attack, the patient was referred to the outpatient clinic for follow-up treatment for asthma. A 22-year-old man is brought to the emergency department after suffering seizures resulting from an overdose of a drug he has been taking. His friends state that he took the drug orally and sometimes had insomnia after taking it. Which of the following is a direct bronchodilator that is most often used in asthma by the oral route and is capable of causing insomnia and seizures It binds to the IgE on sensitized mast cells and prevents activation by asthma trigger antigens and subsequent release of inflammatory mediators. Although approved in 2003 for the prophylactic management of severe asthma, experience with this drug is limited because it is very expensive and must be administered parenterally. One effect that theophylline, nitroglycerin, isoproterenol, and histamine have in common is (A) Direct stimulation of cardiac contractile force (B) Tachycardia (C) Bronchodilation (D) Postural hypotension (E) Throbbing headache 2. A 23-year-old woman is using an albuterol inhaler for frequent acute episodes of asthma and complains of symptoms that she ascribes to the albuterol. A 10-year-old child has severe asthma and was hospitalized 5 times between the ages of 7 and 9. He is now receiving outpatient medications that have greatly reduced the frequency of severe attacks. Which of the following is most likely to have adverse effects when used daily over long periods for severe asthma Which of the following in its parenteral form is life-saving in severe status asthmaticus and acts, at least in part, by inhibiting phospholipase A2 Which of the following has a slow onset but long duration of action and is always used in combination with a corticosteroid by inhalation Oral medications are popular for the treatment of asthma in children because young children may have difficulty with the proper use of aerosol inhalers. Although extremely important in severe chronic asthma and status asthmaticus, corticosteroids do not have a demonstrable direct bronchodilator action. Histamine does not appear to play a significant role in asthma, and antihistaminic drugs, even in high doses, are of little or no value. Blockade of leukotriene receptors with montelukast; inhibition of phospholipase with corticosteroids; and inhibition of mediator release with the IgE antibody are also useful. Parenteral corticosteroids such as prednisolone (the active metabolite of prednisone) are lifesaving in status asthmaticus. Salmeterol is a 2-selective agonist that has a slow onset and long duration of action. Used alone, it increases asthma mortality, but in combination with inhaled corticosteroids prophylactic use improves asthma control. Zileuton is an inhibitor of the lipoxygenase enzyme involved in the synthesis of leukotrienes. Montelukast and zafirlukast are leukotriene antagonists at the leukotriene receptor. Not all asthma patients have vagal reflex output to the bronchi as a major contributor to the bronchospasm, and these patients will not respond well to an antimuscarinic. On the other hand, a patient with severe cardiac disease may be very sensitive to the arrhythmogenic effects of agonists and therefore tolerate these agents poorly, while antimuscarinic agents rarely cause arrhythmias. Nitroglycerin does not cause direct cardiac stimulation but does evoke a compensatory sympathetic reflex. Albuterol is a 2-selective receptor agonist, but in moderate to high doses it produces 1 cardiac effects as well as 2-mediated smooth and skeletal muscle effects. If oral corticosteroids must be used, alternate-day therapy is preferred because it interferes less with normal growth and metabolism in children.
Order genuine sporanox on line
In childhood fungus unity trusted sporanox 100mg, obesity results from increases in the size (hypertrophy) of adipocytes, as well as the formation of new adipocytes (hyperplasia). In adults, obesity principally involves accumulation of lipid within existing adipocytes (hypertrophy). Multilocular adipose tissue (choices A and B), termed brown adipose tissue, is mainly found in newborns. Unilocular adipose tissue with cellular hyperplasia (choice C) occurs in early childhood but does not contribute to the pathogenesis of adult obesity. The meshwork of polygonal strands seen in the image shown in Question 30 consists of the cytoplasm of two adjacent adipocytes and the thin layer of the extracellular matrix that is located between them. Rich supply of blood vessels and nerves are found in the extracellular spaces between the crowded adipocytes. Elastic fibers and collagen fibers are also present in the extracellular matrix between adipocytes, but unlike reticular fibers, they do not form an interwoven network. Skeletal and smooth muscle fibers (choices D and E) are not found in white adipose tissue. A variety of hormones, growth factors, and cytokines are produced in white adipose tissue. Leptin (discussed earlier in this chapter) is a polypeptide hormone secreted by adipocytes that helps regulate food intake and body weight control. Therefore, adipose tissue is not only an organ for energy storage; it also serves as an endocrine organ. Keywords: Obesity, systemic hypertension White adipose tis34 the answer is D: Periorbital space. When caloric intake is reduced, as in this case of anorexia nervosa (a disorder with irrational fear of gaining weight and extreme restriction of food), lipids within adipocytes are broken down and mobilized to provide energy. White adipose tissue in most regions of the body (choices A, B, C, and E) is depleted of lipid. In this connection, articular cartilage acts as an excellent shock absorber and provides resilience against load. This critical biomechanical function is attributed chiefly to which of the following components of cartilage Which of the following best describes the pathogenesis of joint pain in this patient The articular cartilage shown in the image differs from hyaline cartilage in which of the following ways The tumor and tissue margin containing bronchial cartilage are resected, and the specimen is examined by light microscopy (shown in the image). The tissue/substance present within the rectangular box is best described as which of the following The surgical specimen includes normal bronchial cartilage tissue and malignant cells. Which of the following histologic features in this photomicrograph is most useful for determining the specific type of cartilage In considering this case, you recall that the epiglottis at the entrance to the larynx is composed 19 A herniated intervertebral disc was removed surgically from the lumbar region of a 48-year-old man. Before cutting the costal cartilage to open the chest cavity, the surgeon is mindful that healing of cartilage is problematic. She understands that hyaline cartilage has a limited capacity to undergo repair and regeneration due to which of the following intrinsic attributes X-ray of the leg reveals a thickened bone shaft and a mass with poorly defined borders. Based on morphology, which of the following is the most likely diagnosis for this malignant neoplasm The epidural hematoma developing in this patient forms between which of the following two anatomic structures Identify the thin lines indicated by the arrows and the structures that occupy this space. Which of the following best describes the epithelium (indicated by arrows) that lines the surface of bone spicules in spongy bone and the internal surface of compact bone The light-stained line indicated by the arrows represents which of the following bone structures The diagnosis is osteopetrosis, a rare genetic disorder caused by dysfunction of which of the following cell types A femoral head obtained from another patient with this condition reveals attenuated bony trabeculae (shown in the image on the right). Which of the following best explains the pathogenesis of osteopenia in this postmenopausal woman Measurements taken in the office indicate that the patient has grown 15 cm over the past year. Which of the following cells in epiphyseal growth plates was chiefly responsible for the longitudinal growth of long bones in this patient Histologically, the humeral head shows bony trabeculae that are covered by a thicker than normal layer of osteoid (shown in the image). In this section, the osteoid is stained red, and mineralized bone is stained black. Which of the following best describes the pathogenesis of osteomalacia in this patient Longitudinal sections of the epiphyseal growth plate reveal evidence of zonation (shown in the image). Physical examination reveals uneven back musculature and a prominent left scapula caused by rotation of the thoracic ribcage. This developmental abnormality is most likely caused by asymmetric growth of which of the following musculoskeletal structures Which of the following best describes the primary tissue mass in the newly formed bony callus at the site of fracture Extracellular (interstitial) water accounts for 60% to 80% of the wet weight of cartilage and provides resilience to pressure loads applied to the cartilage matrix. None of the other choices contributes significantly to the resiliency of cartilage against pressure. Keywords: Articular cartilage, interstitial water 2 the answer is B: Glycosaminoglycans. None of the other components plays a significant role in binding extracellular water in cartilage. Keywords: Articular cartilage, glycosaminoglycans, proteoglycans 3 the answer is C: Degeneration of articular cartilage. Articular cartilage covers the articular surface of bones and helps reduce friction during joint movement. With advancing age, articular cartilage may undergo progressive degeneration and be worn away, resulting in chronic osteoarthritis. Inflammation of synovium with pannus formation (choice B) occurs in patients with rheumatoid arthritis. None of the other choices are involved in the pathogenesis of degenerative osteoarthritis. Keywords: Degenerative osteoarthritis 4 the answer is B: Absence of perichondrium. Unlike hyaline cartilage, articular cartilage does not have a superficial perichondrium. Aside from this difference, the histologic features of articular and hyaline cartilage are the same and include absence of blood vessels in cartilage matrix (choice A), presence of an amorphous matrix (choice C), and arrangement of differentiated chondrocytes in isogenous groups and lacunae (choices D and E). Collagen fibrils have a refractive index similar to matrix ground substance and are therefore not identifiable in routine histochemical preparations. For this reason, hyaline cartilage typically appears amorphous by light microscopy. Aggrecan is the most abundant proteoglycan core protein found in hyaline cartilage. Hydrophilic proteoglycan aggregates bind interstitial (extracellular) water to the matrix, which accounts for the ability of cartilage to resist compressive forces associated with wear and tear.
Syndromes
- Allergic reaction to the drug used in a stent that releases medicine into your body
- The name of the product (ingredients and strengths, if known)
- In rare cases, a pump may be inserted into the spinal fluid to directly deliver medicine to the nervous system.
- Seizures
- Aplastic anemia
- NSAIDs relieve fever and pain. They also reduce swelling from arthritis or a muscle sprain or strain.
- Eyebrows and lashes appear.
Discount 100mg sporanox overnight delivery
Active screening is fungus link to diabetes buy sporanox 100 mg line, of course, only worthwhile if there is a therapeutic option available. Access to therapy has also been a problem, with a shortage of trained psychologists even in many developed healthcare economies. It is not surprising, therefore, that frequent but unpredictable attacks of breathlessness may ultimately lead to a persistently anxious state. With the development of new treatments, and indeed a fresh look at some of the old, we have managed to move beyond the old nihilistic mindset. The application of each needs to be considered carefully for every patient and integrated into an overall comprehensive individualised management plan. If this can be achieved, it will have a far greater impact on long-term prognosis than any other intervention. Although lung function never returns to normal, it is clear that the patient will be far better off than if they had continued to smoke. Year on year, they will experience fewer symptoms and a better quality of life, as well, of course, as living longer. Smoking cessation therefore remains one of the most important components of management. All patients still smoking, regardless of age, should be encouraged to stop, and offered help to do so, at every opportunity. Without a firm commitment by the individual, smoking-cessations aids will achieve little. Pharmacotherapy for smoking cessation Small doses of nicotine produce predominantly stimulant effects, such as arousal, whereas larger doses produce mainly depressant effects, such as relaxation and relief of stress. Nicotine withdrawal can cause irritability, restlessness, anxiety, insomnia and a craving for cigarettes. Nicotine replacement therapy approximately doubles the success rates of attempts at smoking cessation and smokers should be encouraged to use it to avoid withdrawal symptoms. Typically, a heavy smoker is given transdermal nicotine patches 21 mg/day for 4 weeks, reducing to 14 mg/day for 2 weeks and then 7 mg/day for 2 weeks. Patients who experience marked cravings for cigarettes may benefit from using nicotine chewing gum, lozenges, inhalators or nasal sprays, which provide more rapid peak blood levels from absorption of the nicotine through the buccal or nasal mucosa. Many patients are well down the slippery slope before the diagnosis is established. The graph also demonstrates the effect of smoking cessation on disease progression. Although it is clear that the lung function lost is never regained (emphysema is permanent damage), smoking cessation changes the course of the disease. Clearly, the earlier smoking cessation can 146 Chronic obstructive pulmonary disease stimulating -adrenoreceptors. Short-acting anticholinergic drugs, such as ipratropium, produce bronchodilatation by blocking the bronchoconstrictor effect of vagal nerve stimulation of the bronchial smooth muscle. Although some bronchodilatation is in fact achievable, it is the impact on breathlessness that is of most relevance. These old, long-established drugs are reasonably effective short-term symptom relievers. Bupropion (amfebutamone) is an antidepressant drug that significantly improves the success of attempts at smoking cessation, although its mode of action is uncertain. It has some significant side effects, most notably a 1 in 1000 risk of epileptic seizures, such that it is contraindicated in patients with convulsive disorders, central nervous system disease, bulimia or anorexia nervosa and in patients experiencing symptoms of withdrawal from alcohol or benzodiazepines. As such, it both reduces cravings for and decreases the pleasurable effects of cigarettes, and through these mechanisms it can assist some patients in quitting smoking. Side effects include nausea (common), headache, difficulty sleeping and abnormal dreams. Electronic cigarettes (e-cigarettes) are batterypowered devices designed to resemble a cigarette. They generally use a heating element, known as an atomizer, which vaporizes a liquid solution containing nicotine and a mixture of other chemicals. Whilst some doctors (quite rightly) argue that they are significantly safer than smoking cigarettes, they are not without problems. They are made by the tobacco companies, who, of course, have no incentive to reduce nicotine addiction: the devices generally deliver a large dose of nicotine (accounting for their popularity) and so only reinforce nicotine addiction. Only by breaking addiction to nicotine does an individual have any prospect of remaining a sustained quitter long-term. At present, they remain entirely unregulated, so there is no control at all on what other chemicals are inhaled along with the nicotine. It is also difficult to see how the use of flavours such as bubble gum can do anything other than attract children to the market and increase nicotine addiction. They have greater affinity and a slower rate of dissociation from muscarinic receptors than ipratropium. Their duration of action is at least 24 hours, giving them a convenient once-daily dosage. They also outperform the short-acting ipratropium on all important indices, effectively superseding it as a maintenance therapy in chronic stable disease. Aclidinium has a shorter duration of action and needs to be delivered twice daily but it has the advantage of having fewer anticholinergic side effects. Undoubtedly more efficacious then either agent alone, its place in routine clinical practice will inevitably ultimately be determined by its perceived cost-effectiveness. The combination typically produces a 30% reduction in exacerbation frequency, with a positive knock-on effect in reducing hospital admission rates. These important benefits are seen principally in moderate to severe disease; at the mild end of the spectrum there are usually fewer exacerbations to prevent. This is not usually the fault of the patient but of the prescriber who failed to spend time teaching and checking inhaler technique. Whenever an inhaler is prescribed, care must be taken to coach (and then test) inhaler technique. Theophylline should only be used after a trial of short- and long-acting bronchodilators. The dose should be reduced if a macrolide or fluroquinolone antibiotic is prescribed. Mucolytics are drugs that increase the expectoration of sputum by reducing its viscosity. Treatment strategy In relation to inhaled therapies, the treatment strategy differs depending on the severity of the disease. In mild disease (other than smoking cessation support, for which benefit is prognostic), treatment is principally aimed at short-term symptom control. They are usually effective; if they are not, it is likely to be evident within the first month and they should be stopped. Although symptom control remains important, there is, in addition, evidence of prognostic benefit from certain treatments. In contrast to the symptom controllers in mild disease, prognostic treatments should not be stopped if the patient reports no perceived benefit in the first month. The principle of prognostic treatment is, of course, well understood and accepted in other clinical contexts, such as blood pressure control, hypercholesterolaemia and the use of -blockers post acute coronary syndrome. Patients with advanced disability may have difficulty in performing daily tasks, such as climbing stairs, shopping and washing, and may benefit from assessment by an occupational therapist with regard to home aids such as stair lifts and bath aids. Assessment by a social worker will allow a patient to obtain appropriate allowances. Depression and social isolation are common and can be helped by psychological support focusing on restoring coping skills. Some patients, however, are overweight, because of reduced activity and overeating. Pulmonary rehabilitation is an enormously valuable intervention, but if the patient does not continue to exercise after completion of the formal programme, the benefits in exercise performance are likely to be lost gradually over the following 6 months. Ideally, patients should be encouraged to continue regular exercise; many such opportunities exist in local sports centres and gyms. Patients also benefit in this context from being on appropriate inhaled medication. Typically, a pulmonary rehabilitation programme involves the skills of doctors, respiratory nurse specialists, physiotherapists, dieticians, social workers and occupational therapists.
Buy cheap sporanox 100mg line
This is: A usually treated by fluid restriction B often associated with hypercalcaemia C an indication of metastases to the adrenal gland D an indication of metastases to the pituitary gland E characterised by hypernatraemia 12 fungus scalp discount sporanox 100 mg fast delivery. Small-cell carcinoma accounts for approximately 20% and non-small-carcinoma for 80% (comprising squamous carcinoma, 45%, adenocarcinoma, 20%, and undifferentiated carcinoma, 15%). Mediastinoscopy gives access to the mediastinal nodes but not to nodules in the lung. Radiotherapy and chemotherapy are not appropriate, as they offer a much lower chance of cure for stage I carcinoma. Average survival without treatment is approximately 6 weeks, improving to 8 months with chemotherapy, but long-term survival is extremely unlikely. Patients with these diseases typically present with progressive breathlessness, a dry cough, lung crackles and diffuse infiltrates on chest X-ray. In many cases, this allows a diagnosis to be made with reasonable certainty, but it may sometimes be useful to proceed to biopsy of the lung parenchyma in order to study the histological pattern of the disease. Larger samples can be obtained by surgical biopsy under general anaesthesia by video-assisted thoracoscopy. In many cases, the histological features are characteristic of a particular disease. Bronchoalveolar lavage may be performed through the bronchoscope at the same time as transbronchial biopsy. Aliquots of saline are instilled via the bronchoscope, which is held in a wedged position in a subsegmental bronchus, and fluid is then aspirated for cell analysis. Some of these diseases are characterised in their early stages by an inflammatory alveolitis, which is responsive to corticosteroids, whereas in the later stages there may be irreversible lung fibrosis. Differential diagnosis At presentation, interstitial lung disease must be distinguished from a number of other diseases, such as infective pneumonia, pulmonary oedema, bronchiectasis and malignancy. The overall context of the disease is important and exclusion of other diseases may require further investigations. Once the clinical features suggest interstitial lung disease, a careful search for potential causes must be undertaken. Interstitial lung disease affects the alveoli and lung parenchyma and is characterised by progressive dyspnoea, crackles and a restriction of lung volumes. It is a serious disease, with about 50% of patients dying within 3 years of diagnosis. It is more common in men (male/female ratio 2: 1) and in the older age groups (mean age 70 years). The aetiology is unknown, but it appears to be the result of a failure of repair of lung tissue, whereby epithelial injury culminates in fibrosis rather than a controlled inflammatory and healing process. A small specimen of lung parenchyma can be obtained by passing a biopsy forceps through a flexible bronchoscope, usually under radiological guidance, into the lung periphery. A sample of lung tissue is obtained by biopsying between two limbs in a branching small bronchus. Combinations of prednisolone, azathioprine and N-acetyl cysteine have not proven effective. Pirfenidone is an immunosuppressant that is thought to have anti-inflammatory and antifibrotic effects. Lung transplantation is the main option for selected patients who meet the necessary criteria (see Chapter 19). He failed to respond to prednisolone and died 1 year later of respiratory failure. In cryptogenic organising pneumonia, histology shows intra-alveolar buds of organising fibrosis. Often the patient is thought to have infective pneumonia, but the differential diagnosis is widened when no pathogen is identified and the patient fails to respond to antibiotics. There is typically a dramatic response to corticosteroids, although relapse may occur as the dose is reduced. They have particular features of desquamation of alveolar macrophages or bronchiolitis on biopsy. Lymphoid interstitial pneumonia is characterised by the presence of lymphoid cells in the interstitium. Patients are often given a trial of prednisolone to assess whether any inflammatory component can be suppressed, but there is usually no clinical response and adverse 174 Interstitial lung disease the connective tissue disease or coincidental lung disease (see Table 6. The idiopathic interstitial pneumonias, therefore, are a complex array of inflammatory and fibrotic lung diseases. The lungs may respond to different insults with a similar pattern of inflammation and fibrosis; conversely, a single agent, such as amiodarone, may produce a range of reactions within the lung. The overall clinical management requires the integration of clinical, radiological and histological features in a multidisciplinary meeting. Systemic sclerosis (scleroderma) Diffuse lung fibrosis is the most common complication. Systemic lupus erythematosus Pleural effusions are common and may cause pleural thickening. Rheumatoid disease Involvement of the crico-arytenoid joint causes hoarseness and sometimes stridor. Pleural effusions are common, and analysis of the pleural fluid characteristically shows a high protein level (exudate), with a low glucose concentration and a high titre of rheumatoid factor. Rheumatoid nodules may develop in the lung parenchyma and show the same histological features as the rheumatoid subcutaneous nodules. In these circumstances, diffuse infiltrates on chest X-ray could be as a result of infection, a drug reaction, lung involvement by Hypersensitivity pneumonitis Hypersensitivity pneumonitis (extrinsic allergic alveolitis) is an immunologically mediated lung disease in which a hypersensitivity response occurs in an individual sensitised to an inhaled antigen. When hay is harvested and stored in damp conditions, it becomes mouldy and generates heat, which encourages the growth of fungi such as Thermoactinomyces vulgaris and Saccharoployspora rectivirgula. Likewise, people who participate in the sport of pigeon racing or who keep pet birds, such as budgerigars, can inhale avian antigens. Metalworking fluid alveolitis, for example, has been described in workers in car manufacturing, caused by contamination of fluid used to cool and lubricate metals. The inhalation of these antigens provokes a complex immune response in susceptible individuals, involving antibody reactions, immune-complex formation, complement activation and cellular responses, resulting in alveolitis. These diseases are less common in smokers, probably because of the immunosuppressive effects of cigarette smoke. During such an episode, lung function tests may show a reduction in lung volumes and gas diffusion, and chest X-ray may show diffuse shadowing. The chronic form is characterised by the insidious development of dyspnoea and lung fibrosis. Bronchoalveolar lavage typically shows evidence of a lymphocytic alveolitis, with a predominance of T-suppressor lymphocytes. Precipitating antibodies to avian or fungal antigens can be detected in serum but are also found in many asymptomatic individuals, so that they are not diagnostic. However, pigeon fanciers, for example, are very committed to their sport and will often wish to continue keeping pigeons. They can reduce antigen contact by wearing a mask, loft-coat and hat (so as to avoid carrying antigen on their clothing or hair). Serum immunoglobulin levels are usually elevated and immune complexes are often present in acute sarcoidosis. Sarcoidosis Sarcoidosis is a mysterious multisystem disease characterised by the occurrence in affected organs of noncaseating granulomatous lesions, which may progress to cause fibrosis. The frequent involvement of the lungs raises the possibility that such a putative antigen enters the body via that route. The disease resolved spontaneously, without the need for any medical intervention. There were no crackles on auscultation of her chest, but transfer factor for carbon monoxide and transfer coefficient were reduced to 60% of predicted values. Erythema nodosum this appears as round, red, raised nodules, typically over the shins. Chronic sarcoidosis the chronic form of sarcoidosis pursues a more indolent course, often in an older age group, with involvement of many tissues of the body.
Cheap sporanox online american express
Sertoli cells are tall fungus biology sporanox 100 mg mastercard, columnar, epithelial cells with basal membranes attached to the tunica propria and apical membranes facing the lumen of the tubule. The lateral and apical membranes of Sertoli cells envelop and nourish 30 to 50 germ cells at various stages of spermatogenesis and spermiogenesis. None of the other cells exhibit the distinctive nuclear morphology of Sertoli cells. These cells include early spermatids (arrow 2), late spermatids (arrow 3), primary spermatocytes (arrow 4), and spermatogonia (arrow 5). Junctional specializations of Sertoli cells in the seminiferous epithelium include tight junctions, gap junctions, desmosomes, and hemidesmosomes. Tight junctions create a permeability barrier between basal and adluminal compartments of the seminiferous tubules. These junctions provide ionic coupling in the seminiferous epithelium and help coordinate the cycle of spermatogenesis. Hemidesmosomes connect the basal membranes of Sertoli cells to their underlying basal lamina. The circle encloses a cluster of polygonal cells in the connective tissue between adjacent seminiferous tubules. Granulosa cells (choice B) nourish developing oocytes in the ovaries and secrete estrogen. The tunica propria of the seminiferous epithelium is composed of multiple layers of collagen fibrils and myoid cells. These contractile cells create peristaltic waves that propel sperm and fluid through the seminiferous tubules toward the excurrent genital duct system. In addition to their contractile property, peritubular myoid cells play a role in collagen biosynthesis. The nuclei of fibroblasts (choice B) appear nearly identical to those of myoid cells; however, myoid cells are much more abundant than fibroblasts in the tunica propria. Endothelial cells (choice A), fibroblasts (choice B), and plasma cells (choice D) are present within interstitial tissue of the testes. Spermatogonial stem cells are small, nondescript cells present within the basal compartment of the seminiferous epithelium. Keywords: Spermatogenesis, seminiferous tubules, myoid cells 17 the answer is D: Leydig cells. Leydig cell tumors are rare gonadal stromal/sex cord tumors composed of cells resembling interstitial (Leydig) cells of the testis. The androgenic effects of testicular Leydig cell tumors in prepubertal boys lead to precocious physical and sexual development. By contrast, feminization and 229 gynecomastia are observed in some adults with this tumor. Keywords: Leydig cells, Leydig cell tumor 18 the answer is E: Smooth endoplasmic reticulum. Enzymes involved in the synthesis of steroid hormones such as testosterone and estrogen are associated with membranes of the smooth endoplasmic reticulum. Elaborate smooth endoplasmic reticula are a characteristic ultrastructural finding in steroid-secreting cells. None of the other organelles organizes enzymes involved in testosterone biosynthesis. Spermatids undergo extensive nuclear and cytoplasmic remodeling as they differentiate into sperm. The release of sperm into the lumen of the seminiferous tubule is termed spermiation. Early and late spermatids are distinguished by their small size, condensed chromatin, and proximity to the lumen of the seminiferous tubule. Late spermatids have highly condensed chromatin, in which nuclear histones are replaced by small peptides termed protamines. Once late spermatids are released into the lumen of the seminiferous tubule, they are appropriately referred to as spermatozoa. None of the other cells exhibit the distinctive nuclear morphology of late spermatids. Keywords: Spermatogenesis, testes, spermatids 20 the answer is C: Intercellular bridges. Spermatogenesis is characterized by clonal cell divisions within the seminiferous epithelium. Daughter cells arising from a single type A (dark) spermatogonial stem cell remain intimately connected to one another through intercellular bridges. These open connections are the result of incomplete cytokinesis during mitotic and meiotic cell divisions. Sharing resources helps coordinate the progression of germ cells through the stages of spermatogenesis and spermiogenesis. Intercellular bridges are lost prior to the release of spermatozoa into the lumen of the seminiferous tubule. Keywords: Spermatogenesis, spermiogenesis 21 the answer is D: Intracellular lipid droplets. Like other steroid-secreting endocrine cells, Leydig cells are characterized by the presence of innumerable intracellular lipid droplets. As a result, Leydig cells appear to have a foamy cytoplasm when examined by light microscopy. Cells with a similar, vacuolated appearance are observed in the adrenal cortex (foam cells). Membrane-bound, dense core secretory granules (choice B) are a characteristic feature of neuroendocrine cells. None of the other cellular organelles are ultrastructural features of Leydig cells. The tail is divided into a short neck, middle piece, principal piece, and end piece. The middle piece of the spermatozoan contains mitochondria arranged in a helical fashion around outer dense fibers of the axonemal complex. Of clinical significance, is the observation that sperm-associated mitochondria do not survive fertilization. As a result, the mitochondria of the embryo and adult are derived from the ovum at fertilization. The neck of the spermatozoan contains a pair of centrioles that organize the 9 + 2 arrangement of microtubules in the sperm flagellum during spermiogenesis. Acrosome (choice A) is a membrane-bound vesicle in the head region of the spermatozoan. Karyosome (choice D) is a discrete region of heterochromatin that may be visible by electron microscopy in the nuclei of some cells. Keywords: Spermiogenesis, spermatozoa 24 the answer is D: Opening of membrane Ca2 + channels. Following posttesticular maturation in the epididymis, sperm must undergo capacitation in the female reproductive tract before they are competent to undergo fertilization. Capacitation results in hyperactivation of sperm motility and an increased ability of sperm to bind receptors on the zona pellucida. Biochemical changes associated with sperm capacitation include increased activity of adenylate cyclase, increased tyrosine phosphorylation, activation of membrane Ca2 + channels (correct answer), and other modifications of the sperm plasma membrane and glycocalyx. During spermiogenesis, small vesicles of the Golgi apparatus coalesce to form a large membrane-bound vesicle adjacent to the nucleus. In mature spermatozoa, this acrosomal cap covers the anterior two-thirds of the nucleus. It contains a variety of glycoprotein enzymes, including hyaluronidase, neuraminidase, acid phosphatase, and protease (acrosin). Binding of spermatozoa to receptors on the zona pellucida triggers the acrosome reaction. During this reaction, the sperm plasma membrane fuses with the membrane of the acrosomal cap, thereby liberating acrosomal enzymes.
Discount sporanox 100mg on line
Which of the curves in the graph describes the percentage of binding of a large dose of full agonist to its receptors as the concentration of a partial agonist is increased from low to very high levels Sugammadex interacts directly with rocuronium and not with the rocuronium receptor; therefore fungus gnats lifespan generic 100mg sporanox amex, it is a chemical antagonist. The binding of a full agonist decreases as the concentration of a partial agonist is increased to very high levels. As the partial agonist displaces more and more of the full agonist, the percentage of receptors that bind the full agonist drops to zero, that is, Curve 5. Curve 1 describes the response of the system when a full agonist is displaced by increasing concentrations of partial agonist. This is because the increasing percentage of receptors binding the partial agonist finally produce the maximal effect typical of the partial agonist. Partial agonists, like full agonists, bind 100% of their receptors when present in a high enough concentration. In contrast, pharmacologic antagonists bind to the agonist site and prevent access of the agonist. The difference can be detected experimentally by evaluating competition between the binding of radioisotopically labeled antagonist and the agonist. High concentrations of agonist displace or prevent the binding of a pharmacologic antagonist but not an allosteric antagonist. Predict the effect of a partial agonist in a patient in the presence and in the absence of Name the types of antagonists used in therapeutics. Describe the difference between an inverse agonist and a pharmacologic antagonist. Specify whether a pharmacologic antagonist is competitive or irreversible based on its effects on the dose-response curve and the dose-binding curve of an agonist in the presence of the antagonist. Give examples of competitive and irreversible pharmacologic antagonists and of Name 5 transmembrane signaling methods by which drug-receptor interactions exert Describe 2 mechanisms of receptor regulation. A drug may have high efficacy but low potency or vice versa the ability to activate (agonism) or inhibit (antagonism) a biologic system or effect. In addition, the binding of a drug may be at the site that an endogenous ligand binds that receptor, or at a different site Many drugs act on intracellular functions but reach their targets in the extracellular space. On reaching the target tissue, some drugs diffuse through the cell membrane and act on intracellular receptors. Most act on receptors on the extracellular face of the cell membrane and modify the intracellular function of those receptors by transmembrane signaling Receptors are in dynamic equilibrium, being synthesized in the interior of the cell, inserted into the cell membranes, sequestered out of the membranes, and degraded at various rates. These changes are noted as upregulation or downregulation of the receptor numbers and usually take days to accomplish. The major processes involved in pharmacokinetics are absorption, distribution, and elimination. Appropriate application of pharmacokinetic data and a few simple formulas makes it possible to calculate loading and maintenance doses. Units: liters the ratio of the rate of elimination of a drug to the concentration of the drug in the plasma or blood. Units: volume/time, eg, mL/min or L/h the time required for the amount of drug in the body or blood to fall by 50%. For drugs eliminated by first-order kinetics, this number is a constant regardless of the concentration. Units: time the fraction (or percentage) of the administered dose of drug that reaches the systemic circulation the graphic area under a plot of drug concentration versus time after a single dose or during a single dosing interval. The plasma concentration is a function of the rate of input of the drug (by absorption) into the plasma, the rate of distribution, and the rate of elimination. These parameters are unique for a particular drug and a particular patient but have average values in large populations that can be used to predict drug concentrations. Because the size of the compartments to which the drug may be distributed can vary with body size, Vd is sometimes expressed as Vd per kilogram of body weight (Vd/kg). Drug A diffuses freely between the 2 compartments and does not bind to macromolecules (heavy wavy lines) in the vascular or the extravascular compartments of the hypothetical organism in the diagram. With 20 units of the drug in the body, the steady-state distribution leaves a blood concentration of 2 units. At equilibrium, only 2 units of the total are present in the extravascular volume, leaving 18 units still in the blood. In each case, the total amount of drug in the body is the same (20 units), but the apparent volumes of distribution are very different. Drug C is avidly bound to molecules in peripheral tissues, so that a larger total dose (200 units) is required to achieve measurable plasma concentrations. At equilibrium, 198 units are found in the peripheral tissues and only 2 units in the plasma, so that the calculated volume of distribution is greater than the physical volume of the system. The Vd of drugs that are normally bound to plasma proteins such as albumin can be altered by liver disease (through reduced protein synthesis) and kidney disease (through urinary protein loss). For example, 50,000 liters is the average Vd for the drug quinacrine in persons whose average physical body volume is 70 liters. Thus, the clearance of a drug that is very effectively extracted by an organ (ie, the blood is completely cleared of the drug as it passes through the organ) is often flow-limited. For such a drug, the total clearance from the body is a function of blood flow through the eliminating organ and is limited by the blood flow to that organ. In this situation, other conditions-cardiac disease, or other drugs that change blood flow-may have more dramatic effects on clearance than disease of the organ of elimination. The magnitudes of clearance for different drugs range from a small percentage of the blood flow to a maximum of the total blood flow to the organs of elimination. Clearance depends on the drug, blood flow, and the condition of the organs of elimination in the patient. Like clearance, half-life is a constant for drugs that follow first-order kinetics. Disease, age, and other variables usually alter the clearance of a drug much more than they alter its Vd. Since elimination rate is equal to clearance times plasma concentration, the elimination rate will be rapid at first and slow as the concentration decreases. The bioavailability of a drug is the fraction (F) of the administered dose that reaches the systemic circulation. Bioavailability is defined as unity (or 100%) in the case of intravenous administration. The concentration rises smoothly with time and always reaches 50% of steady state after 1 half-life, 75% after 2 half-lives, 87. The decline in concentration after stopping drug administration follows the same type of curve: 50% is left after 1 half-life, 25% after 2 half-lives, and so on. The asymptotic approach to steady state on both increasing and decreasing limbs of the curve is characteristic of drugs that have first-order kinetics. Even for drugs with equal bioavailabilities, entry into the systemic circulation occurs over varying periods of time, depending on the drug formulation and other factors. After steady-state concentration in plasma has been achieved, the extraction ratio is one measure of the elimination of the drug by that organ. Drugs that have a high hepatic extraction ratio have a large first-pass effect and the bioavailability of these drugs after oral administration is low. An optimal dosage regimen results in the achievement of therapeutic levels of the drug in the blood without exceeding the minimum toxic concentration. To maintain the plasma concentration within a specified range over long periods of therapy, a schedule of maintenance doses is used. If it is necessary to achieve the target plasma level rapidly, a loading dose may be used to "load" the Vd with the drug. Loading Dosage If the therapeutic concentration must be achieved rapidly and the Vd is large, a large loading dose may be needed at the onset of therapy. If the loading dose is large (Vd much larger than blood volume), the dose should be given slowly to prevent toxicity due to excessively high plasma levels during the distribution phase. Part of the administered oral dose (blue) is lost in the gut in the feces or to metabolism, and lost to metabolism in the liver before it enters the systemic circulation: this is the first-pass effect.
100mg sporanox amex
None of the other structures are found in the lamina propria of the small intestine anti fungal infection tablets cheap 100 mg sporanox amex. Keywords: Small intestine, lacteals 5 the answer is E: Stratified squamous, nonkeratinized. The esophagus is a 25-cm tube that passes through the superior and inferior mediastinum. It enters the abdominal cavity at vertebral level T10 and delivers food to the stomach for mechanical and enzymatic digestion. This autopsy specimen was obtained from a patient with a history of chronic gastroesophageal (acid) reflux. The normal mucosa that lines the proximal portion of this esophagus (on the left) exhibits a nonkeratinized stratified squamous epithelium. None of the other types of lining epithelium describe histologic features of the esophagus. Keywords: Barrett esophagus, gastroesophageal reflux disease 6 the answer is E: Metaplasia. Adaptive responses to sublethal cell injury include atrophy, hypertrophy, hyperplasia, metaplasia, and dysplasia. In this autopsy specimen, the normal stratified squamous epithelium of the esophagus (on the left) has been replaced by columnar epithelium with goblet cells (on the right) as a result of chronic injury. Complete intestinal metaplasia with Paneth cells Gastrointestinal Tract and absorptive cells may also occur. Barrett esophagus is more resistant to peptic juice than normal squamous epithelium and appears to be an adaptive mechanism that serves to limit the harmful effects of acid reflux. None of the other cellular adaptations describe histopathologic findings in patients with Barrett esophagus. Keywords: Barrett esophagus, intestinal metaplasia 7 the correct answer is D: Muscularis mucosae. A myenteric nerve plexus is observed between inner circular and outer longitudinal layers of the muscularis externa (oval, shown in the image). These smooth muscle fibers run in a longitudinal direction that is parallel to the overlying epithelium. Contraction of the muscularis mucosae generates ripples in the mucosa that facilitate the movement of food during swallowing. Mucosa (choice B) is the layer that includes surface epithelium, lamina propria, and muscularis mucosae. Submucosa (choice E) is the layer of dense irregular connective tissue that is located between the muscularis mucosae and the muscularis externa. Keywords: Esophagus, muscularis mucosae 8 the answer is A: Ganglion cells in the Auerbach plexus. Absence of peristalsis and failure of the lower esophageal sphincter to relax upon swallowing are referred to as achalasia. Achalasia is associated with depletion or absence of ganglion cells in the myenteric (Auerbach) plexus. Lack of parasympathetic innervation prevents relaxation of smooth muscle in the lower esophageal sphincter during swallowing. A myenteric plexus is shown in the image provided for Question 7 (oval, shown in the image). These structures are composed of peripheral nerves and ganglion cells of postsynaptic parasympathetic neurons. Keywords: Achalasia, myenteric plexus 9 the answer is A: Esophagogastric junction. Examination of the image reveals an abrupt transition from a nonkeratinized stratified squamous epithelium (on the right) to a mucinous columnar epithelium with gastric pits (on the left). These lymphocytes are strategically located to detect and eliminate pathogens (immune surveillance). Fundus and pylorus of the stomach (choices B and E) feature gastric glands, but they do not reveal stratified squamous epithelium. The gastroduodenal junction (choice C) is characterized by the presence of submucosal Brunner glands. The ileocecal 183 junction (choice D) does not exhibit a stratified squamous epithelium. The muscularis externa in this distal portion of the esophagus is composed of smooth muscle; however, the muscularis externa in the upper third of the esophagus is composed of striated skeletal muscle. This image shows a thick layer of visible mucus (amorphous white debris) that is secreted by the surface mucous cells. These columnar epithelial cells are filled with mucinous granules that occupy most of the apical cytoplasm. The mucinous epithelium is interrupted by deep depressions, termed gastric pits (arrows, shown in the image). Visible mucus forms a gel-like coating that protects surface epithelial cells from the harmful effects of acidic gastric juice and mechanical abrasion. These glands produce a neutral pH mucus that is released into the bottom of the gastric pits. A small portion of the muscularis mucosae is visible on the lower right side of the image. The visible mucus that coats the gastric lumen is composed of heavily glycosylated proteins (mucins). In addition to mucins, surface mucous cells secrete bicarbonate ions and potassium. These molecules/minerals provide the mucus with an alkaline pH that serves to neutralize stomach acid near the lining epithelium. The other biomolecules are important components of gastric juice, but mucous cells do not produce them. They play an important role in maintaining bicarbonate secretion by surface mucous cells and increasing the thickness of the surface mucus layer. Pharmacologic agents (nonsteroidal antiinflammatory drugs) that inhibit the formation of prostaglandins can compromise the gastric mucosal barrier, 184 Chapter 13 leading to acute erosive gastritis. Loss of the protective alkaline mucus layer enables acidic gastric juice to injure the mucosa, leading to necrosis and hemorrhage. None of the other small molecules regulates the physiologic gastric mucosal barrier. Fundic glands (also called gastric glands) are composed of parietal cells, chief cells, mucous neck cells, enteroendocrine cells, and stem cells. Except for the cardiac and pyloric regions, these gastric glands are found throughout the stomach. Chief cells are typical protein-producing cells that feature an abundance of rough endoplasmic reticulum. These "protein factories" store pepsinogen (precursor enzyme) within intracellular zymogen secretory granules. Upon contact with gastric juice, pepsinogen is converted to pepsin-an aspartate protease. None of the other gastric cells store enzyme precursors in cytoplasmic zymogen granules. Keywords: Stomach, chief cells 15 the answer is C: Isthmus of glandular epithelium. Gastric glands are branched tubular glands that extend from the bottom of the gastric pit down to the muscularis mucosae. They are connected to gastric pits via a short segment that is referred to as the isthmus. A longer neck region (choice E) connects the isthmus to the fundus of the gland (choice A). Cells destined to become mucous cells migrate up toward the gastric pits (choice B), whereas the other secretory cells. Epithelial stem cells are not found in the lamina propria of the gastric mucosa (choice D).
