
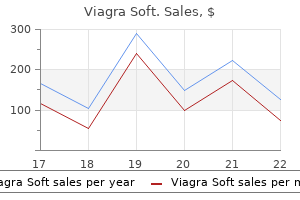
Cheap viagra soft uk
Treating patients with diaminopyridine erectile dysfunction icd 9 code wiki buy genuine viagra soft, a potassium channel blocker, is an effective therapeutic because it increases calcium ion influx by blocking repolarization of the action potential and thereby prolonging spike duration. Ensuring the proximity of these key active zone elements requires a number of proteins. Finally, a close association between synaptic vesicles and the plasma membrane is insufficient for triggered release. V oltage-gated calcium channels must also be in close proximity to the other two active zone elements. Within relatively inactive synaptic terminals that release only one or a few vesicles rarely, the number of docked vesicles is far less than the number in highly active synaptic terminals. Accordingly, the structure of the active zone varies to accommodate the docking of anywhere from a few to many vesicles. In a number of specialized sensory cells with high rates of neurotransmitter release, a proteinaceous "ribbon" extends into the cytosol, with synaptic vesicles docked on all sides of the ribbon. Ribbon-containing synapses are present in sound- and light-sensing cells, as well as in vestibular sensory cells that respond to accelerating forces. Because of their molecularly distant attachments, these proteins only overlap at their untethered ends. Thus, the association is loose initially and the complexed proteins are in the trans- conformation. Vesicle and plasma membranes would fuse if it were not for two interacting molecules, complexin and synaptotagmin. Recall that synaptotagmin is the calcium ion sensor that links release to calcium ion influx. In the absence of a high calcium ion concentration, complexin and synaptotagmin act together to prevent fusion of primed vesicles, thereby "clamping" down on spontaneous synaptic release. When zippering up is complete, even complexin and syntagmin cannot keep the membranes from fusing. Pore expansion initially results in the synaptic vesicle adopting an omega shape before eventually flattening out. Complexin lives up to its name because it is required for activity-triggered vesicle release as well as for clamping down on spontaneous vesicle release. Different parts of the complexin molecule partner with synaptotagmin to clamp down on spontaneous release or, alternatively, to tie triggered release to calcium ion influx. At the peak of the energetic mountain, the synaptic vesicle is docked and primed, held close to but remaining distinct from the plasma membrane. The synaptic delay, the time between a presynaptic action potential and a postsynaptic response, is less than a millisecond. The vast majority of the synaptic delay involves the time needed within the presynaptic terminal, time for an incoming signal to trigger calcium ion influx and then membrane fusion. Diffusion of neurotransmitter across the synaptic cleft and activation of postsynaptic receptors require far less time. For example, the synaptotagmin isoform present in sound-localizing neurons is extremely fast, whereas the isoform in limbic neurons is slow. Clostridial bacteria can only survive in an anaerobic environment and are killed by exposure to oxygen. Fundamentally, the two clostridial toxins work very similarly, but they arrive at their destinations through different routes. Since it is preferentially taken up by motoneurons that utilize acetylcholine as their transmitter, botulinum toxin kills people by preventing the acetylcholine release necessary for breathing. There is no treatment save for placing patients on a ventilator and waiting the weeks or months-depending on the strain involved-that it takes to break down and clear the toxin. Kerner predicted that botulinum toxin could be used as a therapeutic and even experimented on himself to that end. Despite its powerful lethality, botulinum toxin is now used at very low doses and with highly localized application as a treatment for a variety of medical conditions including strabismus or crossed eyes, blepharospasm or excessive blinking, laryngeal dystonia or spasm of the vocal cords, and even for certain types of incontinence. This latter use works because wrinkles are sustained by motoneuron-produced muscle contractions. Therefore, injection of modified botulinum into and near wrinkles blocks release of acetylcholine from motoneurons and therefore blocks activation of the facial muscles involved. The pharmaceutical relaxation of wrinkles lasts for months, as long as it takes to clear the injected toxin, typically strain A. The "safety" of injecting one of the most threatening agents of biological warfare into healthy people requires the usage of extremely low doses in restricted locales. Unlike botulinum toxin, tetanus toxin does not act on the synaptic terminals into which it is originally endocytosed. The toxin is then further transported, again retrogradely but now trans-synaptically. This means that the toxin leaves the dendrites and soma of a motoneuron and travels "backward" across the synaptic cleft to presynaptic terminals. Thus, tetanus toxin ends up in the synaptic terminals of inhibitory interneurons that contact motoneurons, and it is here that tetanus toxin exerts its pathogenic effects. The mechanisms targeting tetanus toxin specifically to the presynaptic terminals of inhibitory interneurons are not known. Within the inhibitory interneuron terminals, tetanus toxin prevents neurotransmitter release. Muscle contractions due to tetanus are sufficiently severe that they cause severe pain and can even break bones. Luckily, tetanus vaccine is effective and widespread, rendering tetanus a disease largely of the past. Physiological extensor muscles (see Section 5) are most affected, resulting in hyperextension. Photograph kindly provided by the Royal College of Scottish Surgeons of Edinburgh. Synchrony is critical for presynaptic cells to speak in a loud and coherent "voice. On average, each presynaptic terminal may spontaneously release a vesicle about once every couple of minutes. Yet, under certain conditions, for example in the presence of certain modulators, the rate of spontaneous release can increase to as much as every other second. Since typical neurons receive thousands of synapses, one or more vesicles may be released onto a neuron during any given millisecond. While this low level of spontaneous release is unlikely to elicit an action potential, it may change the membrane potential or alter excitability. In essence, untriggered, spontaneous vesicle fusion can produce a significant background hum in the neuronal conversations of the brain. The molecules, membrane region, and mechanisms of spontaneous release appear to partially, but not fully, overlap with those of triggered synchronous release. For example, spontaneous release is not dependent on a high concentration of calcium ions throughout the active zone, as is required for activity-triggered release. Thus, at rest, single vesicles of neurotransmitter are released intermittently, perhaps in association with stochastic openings of single calcium channels. Then, when an action potential triggers sufficient calcium ion influx, fusion pores are formed at multiple terminals and neurotransmitter spills simultaneously into multiple synaptic clefts. Now, consider the consequences of losing voltage-gated calcium channels, as occurs in Lambert-Eaton syndrome. More action potentials are required for a triggering concentration of calcium ions to enter through fewer voltage-gated calcium channels. Well, spontaneous release does not depend on a high calcium ion concentration throughout the active zone and therefore it is normal in Lambert-Eaton syndrome. Exciting recent findings suggest that spontaneous release is critical to formation and stabilization of synapses during development. In adults, spontaneous release appears to be an important signal that is used in maintaining synapses at a roughly constant strength across time, a homeostatic process called synaptic scaling. For example, if spontaneous release from a presynaptic terminal plummets, perhaps due to injury or disease, a compensatory boost in synaptic efficacy will result.
Generic 100 mg viagra soft with mastercard
Younger patients tend to have more waxing and waning symptoms erectile dysfunction remedies diabetics purchase 100 mg viagra soft free shipping, while those older than age 50 might have a more abrupt onset, with severe and constant symptoms. There are some clues that might be helpful in differentiation of these conditions. For example, akathisia is a motor restlessness that is usually caused by an inner sense of restlessness, rather than an unpleasant sensation in the limbs, and does not improve with movement nor worsen at nighttime. Therefore, making this diagnosis becomes challenging in children or in individuals who are cognitively impaired. Both sexes and all ethnicities are affected; however, incidence is much higher in Caucasians and women. Neurological examination is essential to rule out other neurological disorders. Among these are blood loss, chronic proton pump inhibitors use, chronic blood Table 9. However, serum iron levels are variable and can be impacted by a variety of dietary and lifestyle factors. In addition, tests for vitamin B12 and folate may be beneficial because their malabsorption can occur in the same medical conditions. A kidney function test and a pregnancy test, in appropriate patients, should be performed as well. Treatment of patients with ferritin levels even less than 75 mg/ml can improve symptoms. Oral iron supplementation along with ascorbic acid, to enhance absorption, could be considered. Among them are sleep deprivation, use of caffeine and/or nicotine, and both lack of exercise and excessive strenuous exercise. It is important to inquire about current and past medications, including asking if any medications were recently stopped. They are not as effective if taken after symptoms have already started, so it is recommended to take these medications about 90 to 120 minutes prior to the typical time of symptom onset. In the smaller dosages, they are less likely to cause the side effects that are typical for this class of medication. Nevertheless, even in these doses, side effects can be seen, and patients should be advised of the possibility of excessive daytime sleepiness, impulse control disorders, nausea, or swelling of the legs. The most troubling side effects of dopaminergic treatment are rebound and augmentation. It can occur during treatment with either dopamine agonists or levodopa, but is much more common with levodopa. Levodopa has the highest rate of augmentation, occurring in close to 70% of patients. Therefore levodopa is not recommended for everyday treatment, but it can be used for patients with sporadic symptoms or as a "rescue" medication for anticipated period of inactivity, such as a prolonged airplane or a car ride. The longer acting dopamine agonists may show a lower rate of augmentation and a high efficacy of symptoms control in some patients. Gabapentin and its derivatives have also been well studied and have demonstrated efficacy comparable with dopamine agonists. In fact, pregabalin (Lyrica) showed equal or superior efficacy compared to pramipexole, without causing typical dopamine agonists side effects. These medications can be especially beneficial in patients with coexisting neuropathic pain or other pain syndromes. Concerns regarding longterm opioid use, such as addiction, tolerance, and sleep apnea, limit their utility. When more regular treatment with opioids is needed, longacting options such as methadone should be considered. Benzodiazepines are also helpful, especially in patients who have severe sleep disturbances. Clonazepam has been studied the most and demonstrated efficacy and safety, even in older patients. However, due to a long duration of action, it can result in side effects of morning drowsiness, cognitive impairment, and unsteadiness. Nonpharmacological management should be tried first and iron deficiency should be treated. Some evidence suggests that folate, magnesium, and B12 might be helpful in pregnancy. Restless legs syndrome: diagnostic criteria, special considerations, and epidemiology. A report from the restless legs syndrome diagnosis and epidemiology workshop at the National Institutes of Health. Prevalence and disease burden of primary restless legs syndrome: results of a general population survey in the United States. Globus pallidus deep brain stimulation for refractory idiopathic restless legs syndrome. Treatment of restless legs syndrome: an evidence based review and implications for clinical practice. This, in turn, causes chronic sleep deprivation, impairment in cognitive function, depression, decrease in work performance, and many other problems. Strong correlation between severity of symptoms and loss of work productivity was observed. The prevalence in Asian populations appears to be higher than that in the Caucasian population for reasons that are not well understood. The spasms are usually very brief, but can occur in runs and are often brought on when the patient voluntarily and forcefully contracts the facial muscles (Video 10. Facial spasms may persist during sleep, and are frequently exacerbated by stress, fatigue, and anxiety. In a study of 115 patients undergoing microvascular decompression surgery, the anterior inferior cerebellar artery was mostly involved (43%), followed by the posterior inferior cerebellar artery (31%), vertebral artery (23%), and a large vein (3%). According to the nerve origin hypothesis, the region of the compressed and demyelinated nerve produces abnormal discharges that precipitate spasms. The demyelinated nerve can produce spontaneous discharges, referred to as ectopic discharges. Additionally, there can be lateral transmission of activity between demyelinated nerve axons, which is referred to as ephaptic transmission. Ephaptic transmission is believed to account for subsequent involvement of the rest of the facial muscles. Rapid amelioration of symptoms following decompression surgery strongly argues for the nerve origin hypothesis. The facial nucleus hypothesis proposes that peripheral facial nerve lesions lead to hyperexcitability of the facial nucleus and the discharges arise from this nucleus. Spontaneous dyskinesias in the elderly and dyskinesias seen in edentulous individuals or those with poorly fitting dentures should also be considered in the differential diagnosis. Transient side effects such as facial weakness, ecchymosis, diplopia, ptosis, lid edema, dry eye, and lacrimation are minimal in experienced hands. This procedure can be curative in about 90% of patients, but it is associated with some risk of complications. Other surgical options such as sectioning of the peripheral nerve trunk or its branches, unilateral removal of the orbicularis oculi and corrugator superciliaris muscles, injection of alcohol or phenol into the facial nerve, and percutaneous puncture of the facial nerve at the stylomastoid foramen have all been used with varying success in the past, but these procedures are rarely used today. A causative vessel was found at the root exit zone of the facial nerve in 81/83 (97. Blepharospasm may occur in isolation with no associated etiology, which is termed primary, benign, essential, or idiopathic blepharospasm. Blepharospasm can also occur in association with other disease entities, such as Parkinson disease and atypical parkinsonian disorders like progressive supranuclear palsy. It can occur in conjunction with dystonic movements of lower facial, oral, jaw, or cervical muscles, as seen in Meige syndrome.
Purchase cheap viagra soft on line
Weeks later erectile dysfunction pump for sale purchase viagra soft in united states online, the comb-over portion of the still-expanding telencephalon surrounds the underlying diencephalon on three sides without connecting to it. The adult brain differs from the early embryonic brain in several important and prominent ways. In fact, the human hindbrain is oriented just off the vertical, and most of the forebrain is oriented in the horizontal plane. The other prominent differences between early embryonic and adult brains are two major fiber tracts in the forebrain. Moreover, these white matter structures contain axons and glia but are neuron-free. Although growth of both tracts begins during gestation, myelination of these tracts, and of axons throughout the nervous system, is not complete until years after birth. The corpus callosum is the major commissural tract that carries axons linking the two cerebral hemispheres and the internal capsule forms a physical join between each cerebral hemisphere and the thalamus. The internal capsule runs between the lateral edge of the diencephalon and the medial edge of each cerebral hemisphere. From the top-down perspective, the axons of the internal capsule run in and out of the page and are therefore depicted as transversely cut. C: A coronal cartoon through the brain (at the level indicated by the dotted arrow) shows that the velum interpositum (vi) is situated between the corpus callosum and the roof of the diencephalon. The internal capsule runs through the subcortical portion of the telencephalon (stippled area) and outlines the lateral edge of the diencephalon. The remaining axons in the internal capsule travel from the thalamus to the cerebral cortex. Fibers of the internal capsule travel along a course that passes between the medial edge of the ventral telencephalon and the lateral edge of the diencephalon. In fact, beyond the small attachments surrounding the foramina of Monro, the internal capsules are the only connection between the telencephalon and diencephalon. Thus, cutting the internal capsule on either side allows the telencephalic cap to be removed from the underlying diencephalon and brainstem. Thus, neurons in frontal cortex send axons through anterior portions of the corpus callosum (genu, rostrum) to the frontal cortex in the contralateral, or opposite, frontal cortex, whereas the axons of neurons in the occipital cortex traverse the most posterior portion of the corpus callosum (splenium). In sum, the corpus callosum allows the two cerebral hemispheres to share information and to seamlessly function with an apparent common purpose. The corpus callosum is the major conduit for interhemispheric communication but not the only one. The hippocampal and anterior commissures connect the hippocampus and other parts of the temporal lobe, respectively. Additional commissures that connect subcortical regions include the diencephalic optic chiasm, the posterior commissure in the midbrain, and the anterior white commissure of the spinal cord. Others receive a callosotomy at the hands of a neurosurgeon in order to treat intractable generalized epileptic seizures. Interestingly, cutting the corpus callosum does not simply reduce the bilateral spread of seizures but actually reduces the incidence of seizure activity, suggesting a role for callosal fibers in facilitating activity in both hemispheres. According to this idea, callosal fibers excite neurons in the two hemispheres, taking them above threshold for epileptiform discharge at the same moment. Recent recordings support the finding that seizures begin simultaneously in both cortices. Cutting the corpus callosum would then block the facilitatory input, which may be just enough to take the excitatory input below threshold and thereby reduce the incidence of seizures. Split-brain patients appear normal upon casual observation and even upon examination. Yet, functional deficits readily become apparent using tests that restrict input and output to opposite hemispheres. For example, if you ask a split-brain patient to view an object located in his left visual field. This is because the left visual scene is represented in the right occipital cortex, which, without the corpus callosum, has no access to the left hemisphere needed for verbal language. Despite being unable to say the name of the object, the patient can correctly pick out the object with the left hand (controlled by the right cortex). Moreover, the patient can only pick out an object from the left visual field with the left hand that is controlled by the right hemisphere. The left hemisphere, which controls the right hand, has no clue that anything happened in the left visual world. When asked to point to the picture that best matched what he had just seen, the patient preformed perfectly: with his left hand, he pointed to a chicken and with his right hand to a snow shovel. Moreover, neither this nor similarly challenged patients say, "I have no idea why I did that," which would be the truth. Making up a sensible explanation or justification for our actions, telling a plausible story for why we do what we do, arises out of the left hemisphere playing the role of interpreter. The left hemisphere interpreter is not bound by truth and, in fact, is often responsible for confabulation. Critical to understanding ourselves is understanding that the interpreter works its confabulatory magic in all of us, not just in split-brain patients. In a classic experiment by the American psychologist Norman Maier, people were asked to tie two hanging cords together. After subjects struggled with the task for a while, Maier nonchalantly set another cord into pendulum motion. Immediately thereafter, the subjects swung one cord as they would a pendulum and were able to grab both cords and accomplish the task. One subject who was a psychology professor reported an elaborate image of monkeys swinging across a river that appeared to him out-of-the-blue as his motivation. Even when specifically told about the cue, subjects averred that they could see that others may have used the clue but were sure that they had not. We may report reasons for our actions, but, more often than not, these reasons have a sketchy relationship to actuality. But, if the left hemisphere is needed for fully understanding and expertly producing verbal language-which it is (see Chapter 16)- how was the split-brain patient able to use verbal instructions to point to the snow shovel with his left hand to begin with The simple answer is that the right hemisphere has some capacity for language comprehension and is able to understand syntactically simple instructions and to even produce simple words nonverbally by, for example, arranging letter blocks with the left hand. Because the right hemisphere can understand simple instructions, it has been possible to test each hemisphere independently in split-brain patients. The picture that has emerged is that the hemispheres are not duplicates, with identical abilities and only differing with respect to the side involved. Instead, the left and right cerebral hemispheres each have particular propensities or talents that are not fully shared by the other. The left hemisphere, beyond housing critical regions involved in language, is particularly well suited to logical, mathematical, and sequential thoughts. In contrast, the right hemisphere possesses a more global perspective and is particularly good for nonsequential image-derived reasoning independent of language. For example, when asked to put blocks together to match a pattern, the right hemisphere controlling the left hand succeeds quickly, and the left hemisphere fails miserably in directing the right hand to accomplish the same task. Both hemispheres may be able to accomplish similar endpoints but will do so differently. In the embryonic cord, the central lumen has a bilateral inflection point or indentation. Thus, primary sensory afferents enter the spinal cord from the dorsal side, bringing information to the dorsal part of the spinal gray matter. Motoneurons innervating skeletal muscles have somata in the ventral portion of the spinal gray and send an axon out from the ventral spinal surface. In the hindbrain (B), the sulcus limitans (arrowhead) again separates cells destined for a sensory role from those destined to become motor-related.
Cheap viagra soft 100 mg mastercard
Vitus dance" to describe chorea seen in what is now his eponymous disease natural treatment erectile dysfunction exercise buy discount viagra soft 50mg on-line, although this is unrelated to the original use of the term. Chorea is defined as involuntary, irregular, arrhythmic, nonpatterned, purposeless movements that flow randomly from one body part to another. It is the hallmark movement disorder present in Huntington disease but can also be seen in several other inherited neurodegenerative disorders, as well as in acquired disorders from a myriad of causes, whether structural, immunemediated, or metabolic. When chorea affects the proximal extremities, choreic movements assume a higher amplitude, violent look, and are termed ballism. Nonpatterned, writhing movements generally affecting the distal extremities are called athetosis. Ballism can occur secondary to stroke or from damage to pallido subthalamic pathways from other causes. Athetosis is commonly seen in cerebral palsy, but can be seen in the setting of primary dystonia as well as in combination with choreic disorders. Chorea Definition the term "chorea" is used to describe involuntary movements that are irregular and unpredictable in temporal and anatomic distribution. Patients with chorea commonly demonstrate other features including motor impersistence (the inability to sustain voluntary muscle contraction), exaggerated gestures that are caused by superimposition of chorea onto voluntary movements, and an irregular, dancelike gait. Patients can usually temporarily and partially consciously suppress chorea, and choreic movements in one body part can be brought out by asking the patient to perform complex motor tasks elsewhere in the body. Tendon jerks may assume a "hung up" characteristic (prolonged relaxation of the limb to neutral position after reflex testing). There are considerable geographical differences in prevalence, with a much lower prevalence in Japan and among South African blacks and a much higher prevalence in the Lake Maracaibo region in Venezuela. The N terminal of mutant huntingtin can bind to transcription factors and lead to a reduction in acetylated histones and decreased gene expression, which may adversely affect neuronal survival. People often try to blend their chorea into purposeful movements, which is termed "parakinesis. Mild dystonia, in addition to chorea, gives rise to choreoathetosis, and use of anti dopaminergic drugs may increase the likelihood of dystonia. Eye movement abnormalities are among the earliest motor signs, with slow, uncoordinated voluntary initiation of saccades, disrupted smooth pursuit and impersistence. Initiation of internally generated saccades is harder than that of externally triggered ones, suggesting relative sparing of parietal lobesuperior collicular pathways in the setting of extensive frontostriatal circuit dysfunction. Optokinetic nystagmus is impaired in both vertical and horizontal directions, with vertical movements impaired earlier in the course. Dysphagia tends to be prominent in the terminal stages and aspiration is a common cause of death. Cognitive impairment occurs in all patients, but the rate of progression varies considerably. Aggregates of n-htt disrupt axonal transport through huntingtin interacting proteins Translocation of N Terminal 8. Wildtype huntingtin protein (htt) is predominantly cytoplasmic and probably subserves multiple functions including vesicle transport, cytoskeletal anchoring, endocytosis mediated by clathrin, and axonal transport. Htt may be transported into the nucleus and have a role in transcriptional regulation. Ultimately, toxicity may be caused by mutant fulllength htt or by cleaved Nterminal fragments, which may form soluble monomers, oligomers, or large insoluble aggregates. Cognitive inflexibility and loss of executive function may be related to frontostriatal circuit dysfunction. Insight and central language function may remain preserved, even in the advanced stages. Aggression and irritability are the common behavioral changes seen, along with anxiety and apathy. Diagnostic suspicion is increased by the presence of behavioral and psychiatric disturbances, which may be subtle at onset, and may need to be elicited by direct questioning (see Box 6. Patients may be unaware of these symptoms and information should be corroborated by interviewing family members if possible. A psychiatric family history, including history of psychotic disorder, dementia, and suicide should also be obtained. The testing can identify gene carriers before or after the onset of clinically manifest disease. Presymptomatic gene testing should only be carried out in association with genetic counseling, preferably also in combination with a psychologist and a neurologist with supportive care and counseling before and after testing. A valid reason for presymptomatic testing includes family planning, but testing merely out of curiosity should not be done casually. Presymptomatic and atrisk individuals should be given the opportunity to discuss the risks and benefits of testing and be provided psychological and social support in the context of genetic testing. Hence, in general, it is not recommended to treat chorea unless it is causing disabling functional and social impairment. Tetrabenazine reversibly binds to type2 vesicular monoamine transporter and causes central monoamine depletion. Commonly reported adverse effects include sedation, depression, anxiety, insomnia and akathisia. Neuroleptics are used frequently: atypical antipsychotics may reduce chorea with fewer extrapyramidal side effects than typical antipsychotics. It is advisable to use the lowest effective doses of tetrabenazine or antipsychotics for chorea management. Periodically reassess (and if necessary, reduce) therapy with these agents, since parkinsonism, dysphagia, and gait impairment may evolve and become prominent with advancing disease, with less chorea, and tetrabenazine may worsen these symptoms. Psychosis is uncommon but disabling, and newer antipsychotics are the mainstay of treatment, with clozapine, quetiapine, and olanzapine thought to have the fewest neurological side effects. The potential targets for neuroprotection are summarized in the Science Revisited box. Other inherited choreas Chorea may result from several other inherited neurodegenerative disorders. Chorea may infrequently be seen in Wilson disease; therefore anyone younger than 50 presenting with chorea, tremor, or dystonia should be screened using urine copper, serum ceruloplasmin, and slitlamp examination, since copper chelation may halt the progression and even improve motor function in this otherwise devastating disorder. Trend to improved maximal chorea, verbal learning and Stroop color naming Remacemide Not discussed - - 1 Study Table 6. Chorea, Athetosis, and Ballism 53 seen on microscopic exam) and neurological dysfunction. In addition, both of these disorders have neuromuscular involvement and might have hepatosplenomegaly, which can help narrow the differential. In ChAc, the motor phenotype includes limb and orolingual dystonia including the characteristic "feeding dystonia," where the tongue protrudes and pushes food out of the mouth. In addition, there may be prominent selfmutilation in the form of tongue biting and lipbiting. Seizures may be the first manifestation of the disease, and psychiatric manifestations including psychosis and obsessivecompulsive behaviors are also common. Psychosis, obsessivecompulsive disorder, and depression are common, and may predate the movement abnormalities. There is prominent myopathy with muscle atrophy, and cardiomyopathy with conduction abnormalities and life threatening arrhythmias can occur. Onset of neurological symptoms is in the first decade, with orofacial and limb dystonia, spasticity, and chorea. Lingual dystonias, including the feeding dystonia seen with ChAc, may respond to some degree to botulinum toxin injections in the genioglossus. Anticonvulsants, such as valproate, used to treat seizures may help the involuntary movements as well. Supportive care, including speech therapy, to help with dysphagia and physical/ occupational therapies to improve gait impairment are generally required. Acquired choreas Chorea may also present as a symptom of metabolic and endocrine disorders, vascular disorders (including inflammatory vasculitides), infectious or parainfectious processes, and toxicity related to medications or other agents (Table 6. For many acquired choreas, removal of the inciting cause may help alleviate chorea. When the cause is a structural lesion, the abnormal movements generally improve with time, although symptomatic treatment may be helpful in the acute stages or with disabling movements. Behavioral and psychiatric abnormalities 54 Non-Parkinsonian Movement Disorders Box 6. Other features of acute rheumatic fever, such as carditis and arthritis, may also be present.

Quality 100 mg viagra soft
At the base of the fluid-filled cochlea is the oval window upon which the stapes presses erectile dysfunction trials buy generic viagra soft 50mg line. The stapes moves the oval window toward and away from a U-shaped, perilymph-filled cochlear compartment composed of two different regions joined by a narrow canal. The region adjoining the oval window is the scala vestibuli or the vestibular canal. The scala vestibuli runs from the oval window at the base of the cochlea to the tip of the cochlear spiral, where it connects through the helicotrema to the scala tympani or the tympanic canal. At the basal end of the scala tympani is the round window, a membranous structure similar to the oval window. Because of the connection at the helicotrema, there is no actual divider between the perilymph-filled scala vestibuli and scala tympani. The scala vestibuli, cochlear duct, and scala tympani are all fluid-filled compartments within the cochlea. The helicotrema is a narrow channel that connects the scala vestibuli and scala tympani at the apex of the cochlea. The pressure wave crosses through the cochlear duct and then moves down the scala tympani to impact the round window. B: A rough outline of the tonotopy in the cochlea is illustrated on a cartoon of the bony cochlea viewed from the apex (asterisk). C: Compression at the oval window results in rarefaction at the round window (red arcs). Conversely, rarefaction at the oval window results in compression at the round window (dim brown arcs). Pressure waves of different frequencies pass through the cochlear duct at different locations along the base-to-apex axis. Note that the bony cochlea is wide at its base and narrow at the apex but that the orientation of the cochlear duct is reversed, narrow at the base and wide at the apex. Between the scala vestibuli and scala tympani runs the cochlear duct, the sensory region of the cochlea. The cochlear duct separates the scala vestibuli and scala tympani for most of their lengths, ending just short of the cochlear apex, where the helicotrema joins the two canals. The cochlear duct shares one wall with the scala vestibuli and one wall with the scala tympani. Like the scala vestibuli and scala tympani, the cochlear duct is filled with fluid but the fluid in the cochlear duct is endolymph rather than perilymph (see more later). Importantly, the cochlear duct is flexible, so that pressure waves move the cochlear duct up and down. Because the cochlea is surrounded by unyielding bone, two pressure valves are needed to support any movement of the fluid within. Just as liquid does not come out of a single pinhole in a soda can, movement of the oval window only produces a pressure wave because a second compressible portal, the round window, exists. Compression at the oval window results in rarefaction at the round window, and rarefaction at the oval window produces compression of the round window. Airborne sounds that arrive at different frequencies set up movements of the oval window at corresponding frequencies. The movement of the oval window in turn sets up a pressure wave at a given frequency that travels through the cochlea. Thus, pressure waves at the highest frequency represented in the human cochlea (20,000 Hz) move the cochlear duct at the base of the spiral; pressure waves with low frequencies (less than 200 Hz) move the cochlear duct closest to the helicotrema. An important mechanism of tonotopy is the flexibility of the stiffest part of the cochlear duct, the basilar membrane. Recall that the basilar membrane forms the border between the cochlear duct and the scala tympani. The narrow basilar membrane at the base of the cochlea is stiffest and therefore moves maximally in response to high-frequency pressure waves. In contrast, at the apex of the cochlea, the wide basilar membrane is relatively loose and bends maximally in response to low-frequency pressure waves. Consequently, the basilar membrane moves maximally in response to sounds of progressively lower frequencies as one moves from the base of the cochlea to its apex. This topographic arrangement of maximal pressure wave excursion along the length of the cochlea follows a tonotopic organization. The tonotopy of the basilar membrane dictates a tonotopic neural response to sound so that the apical cochlea responds best to low-frequency sounds and the basal cochlea responds best to sounds of high frequency. The frequency that produces the greatest movement of the basilar membrane, and consequently the greatest hair cell response at any one point within the cochlea, is termed the characteristic frequency. Dividing the organ of Corti from the rest of the cochlear duct is the tectorial membrane, which emanates outward from the modiolus, the central pillar of the cochlear spiral. Sensory hair cells sit atop the basilar membrane and extend cellular extensions termed stereocilia into the scala media, the fluid chamber of the organ of Corti. At the outer edge of the cochlear duct is a specialized tissue, the stria vascularis, which pumps potassium ions into the scala media to form endolymph. Endolymph is a potassium ion-rich fluid that fills the scala media, the fluid-filled portion of the cochlear duct. The organ of Corti contains two types of hair cells, inner and outer, and the tectorial membrane (tm). Spiral ganglion cells (blue) innervate a single row of inner hair cells (blue) and carry afferent input from the inner ear to the cochlear nuclei in the hindbrain. Efferents arising from cells in the pons (maroon) innervate three rows of outer hair cells (maroon). B: the stereocilia of outer hair cells (ohc) are embedded in the tectorial membrane. When a sound elicits a pressure wave in the cochlea, the basilar membrane moves up and down at the frequency of the incident sound. If the frequency of basilar membrane movement matches the characteristic frequency of the hair cells at the cochlear location, the outer hair cells themselves will move up and down. The movement of outer hair cells serves as an independent resonator, which amplifies the movement of the basilar membrane. The stereocilia of inner hair cells (ihc) float within the endolymph and respond to pressure waves produced by basilar membrane movement and the movement of endolymph. The responses of inner hair cells are conveyed to spiral ganglion cells through a synapse. Hair cells are mechanosensitive sensory cells present in both the cochlea and vestibulum. These stereocilia are in fact neither cilia nor "hairs" but instead are long extensions from the cell body that contain an inner actin skeleton. Stereocilia are arranged from short to tall, with thin proteinaceous tip-links linking shorter stereocilia to their taller neighbors. The direction of hair bundle deflection that causes cell depolarization-toward the tallest stereocilia-is the preferred direction. When the stereocilia are bent away from the tallest stereocilia (the nonpreferred direction), the probability that the mechanoelectrical transduction channel will close increases, thus hyperpolarizing the cell. Cochlear hair cells are aligned so that all the hair cells in a patch of cochlea share a response to hair bundle stimulation. A: A colorized scanning electron micrograph showing a top view of outer (left three rows) and inner (right row) hair cells. B: All cochlear hair cells have three rows of stereocilia, but they are arranged as an arrowhead in the outer hair cells and in a straight line in the inner hair cells. The preferred direction, defined as the direction of hair bundle movement that leads to hair cell depolarization, is deflection toward the tallest stereocilia (brown arrow). D: Outer hair cells alter the basilar membrane displacement in response to incoming pressure waves. In this way, they serve as the cochlear amplifier to both amplify and narrow the tuning of the stimulus delivered to the inner hair cells. The inner hair cells synapse onto spiral ganglion cells that in turn provide sensory input to hindbrain cochlear nuclear neurons.
Cheap viagra soft on line
Mild recurrent abdominal pain is a less urgent problem and may be assessed in an hour or two if you have other patients with higher priority problems erectile dysfunction in diabetes mellitus ppt generic viagra soft 100mg line. Perforated or ruptured viscus Ascending cholangitis o Necrosis of a viscus o Exsanguinating hemorrhage A perforated or ruptured viscus may result in hypovolemic shock (from third-space losses), septic shock (from bacterial peritonitis), or both. Necrosis of a viscus, as in severe pancreatitis, intussusception, volvulus, strangulated hernia, or ischemic colitis, may cause hypovolemic or septic shock and electrolyte and acid-base disturbances. Exsanguinating hemorrhage with hypovolemic shock may result from a leaking abdominal aortic aneurysm, a ruptured ectopic pregnancy, or a splenic rupture; the cause is occasionally iatrogenic, such as a liver or renal biopsy or a misdirected thoracentesis. Patients with myocardial infarction and aortic dissection occasionally present with abdominal pain. These cardiovascular diagnoses should be considered, especially if no local abdominal signs can be identified. Patient-Related Problems: the Common calls Appearances are often deceptive in acuk abdominal disease. If the patient 1w recently received narcotic analgesics or high-dose steroid~, he or she may appear well despite a serious underlying problem. Patients with severe colic are often restless; those with peritonitis, in contrast. With peritonitis, patients may have their knees drawn up to reduce abdominal tension. Hypotension associated wi1:h abdominal pain is an ominous sign suggestive of impending hypovolemic, hemorrhagic, or septic shock. Abdominal Pain Does the patient have postural changes (lying and standing) in the blood pressure and heart rate If the supine blood pressure is normal, recheck the blood pressure and heart rate with the patient standing. A drop in blood pressure that is associated with an increased heart rate (>15 beats/minute) is suggestive of volume depletion. Fever associated with abdominal pain is suggestive of intraabdominal infection or inflammation. However, lack of fever in an elderly patient or in a patient receiving an antipyretic or immunosuppressive drug does not rule out infection. Selective History and Chart Review Diagnosis is often dependent on a careful history that addresses the following issues: 1. Remember that a patient may complain of diffuse abdominal pain, but on careful examination, the pain may be found to be localized. Right lower quadrant: A, appendix (appendicitis,* abscess); 0, ovary (torsion, ruptured cyst. Generalized abdominal pain: (1 See conditions marked with an asterisk(*, (2 peritonitis (any cause), (3) diabetic ketoacidosis, (4 sickle cell crisis, (5) acute intermittent porphyria, and (6) acute adrenocortical insufficiency resulting from steroid withdrawal. Patient-Related Problems: the Common Calls Does the patient characterize the pain as severe or mild, burning or knifelike, or constant or waxing-and-waning, as in colic The pain of a peptic ulcer tends to be burning, whereas that of a perforated ulcer is sudden, constant, and severe. An acute onset with fainting is suggestive of perforation of a viscus, ruptured ectopic pregnancy, torsion of an ovarian cyst, or a leaking abdominal aortic aneurysm. A ruptured viscus may be initially associated with localized pain that subsequently shifts or becomes generalized, with the development of chemical or bacterial peritonitis. Thus, in biliary colic, pain is frequently referred to the inferior angle of the right scapula. Pain that increases with meals, decreases with passage of bowel movements, or does both is suggestive of a hollow gut origin. An exception is pain from a duodenal ulcer, which is often relieved by the ingestion of food. The pain of pancreatitis is often worse after eating and may be relieved by sitting up or leaning forward. Pain that increases with inspiration is suggestive of pleuritis or peritonitis, and pain that is aggravated by micturition is suggestive of a urogenital cause. Vomiting that occurs with the onset of pain frequently accompanies both acute peritoneal irritation and perforation of a viscus. It is also commonly associated with acute pancreatitis and with obstruction of any muscular hollow viscus. Vomiting many hours after the onset of abdominal pain may be a clue to intestinal obstruction or ileus. Brown, feculent emesis is pathognomonic of bowel obstruction, either paralytic or mechanical. Vomiting food after fasting is consistent with gastric stasis or gastric outlet obstruction. Diarrhea and abdominal pain are observed in infectious gastroenteritis, ischemic colitis, appendicitis, and partial small bowel obstruction. Diarrhea alternating with constipation is a common symptom of diverticular disease. Fever and chills that accompany abdominal pain are suggestive of an intra-abdominal infection. Also check the medication sheet for antipyretic or steroid use; remember that fever may be masked by the administration of these medications. Past History and Chart Review Does the patient have a history of peptic ulcer disease or antacid ingestion If the patient has a history of peptic ulcer, check for the presence of a new one. Patient-Related Problems: the Common Calls Does the patient have a history of blunt or penetrating trauma to the abdomen Has there been a liver or kidney biopsy or has thoracentesis been performed since admission A subcapsular hemorrhage of the spleen, liver, or kidney may result in hemorrhagic shock 1 to 3 days later. Spontaneous bacterial peritonitis must always be considered in an alcoholic patient with ascites and fever. Atherosclerosis is a diffuse process and may affect the vascular supply to several body systems. In addition to the possibility ofa myocardial infarction that manifests with abdominal pain, you should consider a leaking abdominal aortic aneurysm, aortic dissection, and ischemic colitis caused by atherosclerosis ofthe mesenteric arteries. If the patient is a premenopausal woman, what was the date of her last normal menstrual period Abdominal pain associated with a missed period raises the possibility of an ectopic pregnancy. Hypotension in this situation is suggestive of a ruptured fallopian tube as the result of an ectopic pregnancy, which is a life-threatening situation. Intra-abdominal hemorrhage may occur in the anticoagulated patient, especially ifthe patient has a history of peptic ulcer disease. Does the patient have a history of use of aspirin or nonsteroidal anti-inflammatory drugs, alcoho~ or other ulcerogenic drug Peptic ulcer should be a consideration in a patient who has been taking one or more of these agents. Note that the bulge of the inguinal hernia begins superiorly to the inguinal ligament whereas the bulge of the femoral hernia originates inferiorly to the inguinal ligament. Sh0t:k For either hypovolemic or septic shoc:k, the initial treatment is the aame and is aimed at immediate expansion of the iDtraY&scular volume: 1. A psoas sign is manifested by abdominal pain in response to passive hip extension. An obturator sign Is manifested by abdominal pain In response to passive Internal rotation of the right hip from the 9Cklegree hi,H<nee flexion position when the patient is supine. In extreme circwnstances, 0-negative blood may be used during the wait for the crossmatched supply. When shock occurs in the setting of a disorder causing abdominal pain, urgent surgical consultation is almost always required.
Buy 50 mg viagra soft with amex
Otoacoustic emissions may be low in amplitude impotence grounds for annulment buy generic viagra soft online, but they can be picked up by a microphone placed into the ear canal. Otoacoustic emissions can occur spontaneously but can also be elicited by playing a tone into the ear. Tone-evoked otoacoustic emissions start with the activation of outer hair cells by the incoming tone. Then, the rest of the reverse pathway just described ensues, and the result is an emission of the same frequency as the tone that was originally played into the ear. Since otoacoustic emissions depend on healthy outer hair cells, the presence of evoked otoacoustic emissions can be used as an early test for cochlear health. This test is particularly useful for testing the hearing of babies, young children, and nonverbal individuals. In fact, the highest frequency sound that mammals such as bats can hear is more than 100 kHz. To place the challenge of high-frequency responses in context, first consider the relatively easy job of responding to sinusoidal stimulus at 10 Hz. A 10 Hz stimulus moves the hair cell stereocilia bundle in one direction for 50 ms, an ionotropic ion channel "eternity. In that 25 s time period, the hair cell stereocilia must physically move and an ion channel in the hair cell membrane must open for a hair cell to respond. Musical instruments produce sounds as low as 8 Hz, the lowest note produced by an organ, or 65 Hz, the lowest note produced by a cello. At the high end, the highest note sung by a soprano is more than 1 kHz, the highest note of a flute more than 2 kHz, and the highest note of a violin more than 4 kHz. When we are born, we can hear frequencies up to 20 kHz or so, but we lose the ability to hear the highest frequencies as we age. By the time we are in our twenties, most of us only hear frequencies up to 16 kHz or so. Young people use ringtones at frequencies above 16 kHz to allow them to receive cell phone calls unnoticed by their teachers, who are typically unable to hear the high-frequency sounds. Conversely, business owners have employed devices that emit a high-pitched sound, at about 17 kHz, designed to discourage young people from hanging around outside stores. Particularly fast potassium channels, present in the membrane of the hair cell soma, are activated by depolarization and are responsible for repolarizing hair cells quickly. For example, vibration of the basilar membrane at 1 kHz alternately moves the basilar membrane sinusoidally up and down every millisecond. Because of the fast repolarization mechanisms in hair cells, hair cells show a sinusoidal response of alternating depolarization and hyperpolarization with a period as short as 1 ms. However, hair cells cannot follow the sinusoidal movements at frequencies greater than 3 kHz or so. Sounds above frequencies of 3 kHz produce a sustained depolarization of hair cells at the corresponding tonotopic location. When a sound occurs and a pressure wave moves the basilar membrane up and down (gray), the stereocilia of the hair cell are bent. When the stereocilia bend toward the tallest stereocilium (middle), the preferred direction, the hair cell depolarizes; when the stereocilia bend away from the tallest stereocilium, the hair cell hyperpolarizes. When the membrane potential is depolarized above the resting potential, release of neurotransmitter is increased. The release of more glutamate (glu) vesicles increases the probability of an action potential in the postsynaptic spiral ganglion cell. B: In response to a pressure wave of 3 kHz or less (stimulus), a spiral ganglion cell fires one or more action potentials in response to each cycle. The number of action potentials fired per cycle is greater as the amplitude of the stimulus increases. Genetic causes of deafness stem from mutations in genes for connexins, the gap junction building blocks; channels and transporters found in the stria vascularis; and several transmembrane proteins with as of yet undiscovered functions. In fact, mutations in genes coding for connexins are the most common genetic cause of deafness. These forms of hearing loss or deafness are termed nonsyndromic (syndrome derives from Greek for "to run together") in that they do not run with symptoms in vestibular or other functions. The inner hair cells are the conduit for sensory information from the cochlea bound for the brain. Regardless of their indirect or direct roles, both outer and inner hair cells are needed for normal hearing. Aminoglycoside antibiotics and the chemotherapeutic agents cisplatin and carboplatin can kill hair cells. Ototoxic drugs may have a predilection to kill either cochlear or vestibular hair cells or may be toxic to hair cells in both parts of the inner ear. The antineoplastic agents neomycin, kanamycin, and amikacin act primarily in the cochlea and primarily on outer hair cells. In the case of ototoxic antibiotics, affected cells die through caspase-dependent apoptosis. The cochlear hair cells most at risk for ototoxicity are outer hair cells in the basal turns of the cochlea. Loss of basal outer hair cells leads to a loss of hearing in the high-frequency range and an accompanying tinnitus. Although the proportion of patients suffering ototoxic hearing loss is relatively small, the consequences for affected patients can be devastating. Often, the patient taking an antibiotic or chemotherapeutic is an older individual who, upon losing hearing, lacks the resources to compensate by learning sign language or lip-reading or using a cochlear implant. Fortunately, the prescription of some ototoxic compounds can be avoided when alternative therapeutic approaches exist. When prescription of a potentially ototoxic compound is warranted, close monitoring of serum levels should be used to prevent audiologic or vestibular damage. Since genetic factors may predispose some to ototoxic damage, patients with a family history should be particularly carefully managed. Close to the apex of the cochlea, the basilar membrane will resonate at 500 Hz, and the inner hair cells there will respond with alternating depolarizations and hyperpolarizations every 2 ms (equal to the period of a 500 Hz stimulus). The location of the hair cell and the identity of the auditory afferent brand the stimulus as having a characteristic frequency of 500 Hz. In addition, the afferent fires action potentials that occur with a frequency of 500 Hz. Hair cell location, afferent identity and firing pattern all combine to effectively code sound frequencies up to 3 kHz. However, above 3 kHz, auditory afferents cannot follow the stimulus by firing an action potential once per period of stimulation. Therefore, auditory afferents coding for sounds at frequencies above 3 kHz employ a labeled-line mechanism rather than discharge pattern for coding. Because of their elevated resting potential, hair cells can signal pressure waves in either the preferred or nonpreferred direction. This fits with the fact that it is the frequency of pressure waves rather than the direction of hair bundle deflection that carries meaning in the auditory system. The elevated resting potential in hair cells leads to ongoing release of glutamate and therefore a resting discharge in the spiral ganglion cells, even in conditions without sound. Thus, the hair cell-to-spiral ganglion cell is a much-trafficked synapse with, as it turns out, its own version of synaptotagmin called otoferlin. Otoferlin serves as the calcium ion sensor that triggers neurotransmitter release from hair cells. In people with otoferlin mutations, pressure waves are transduced normally but no sound-related activity occurs in the auditory nerve fibers, causing nonsyndromic deafness. Because of this architecture, auditory pathway neurons that are third-order or more carry information about sound arriving at both ears. Neurons in the inferior colliculus and in the medial geniculate nucleus carry bilateral auditory information, as do auditory cortex cells.
Buy viagra soft canada
Its duration of action is relatively short; therefore erectile dysfunction specialist doctor order viagra soft 50mg with visa, overdose cases must be monitored for resedation. Confusion/Decreased Level of Consciousness Dementia Dementia is a diagnosis of exclusion. Aggressive treatment of the kidney failure (dialysis, if necessary or liver failure lactulose, neomycin) should be undertaken when indicated. Hyponatremia or Hypernatremia For the management of hyponatremia or hypernatremia, refer to Chapter 35. Mania, DepreS$ion, or Schizophrenia For suspected mania, depression, or schizophrenia, psychiatric consultation is necessary for confirmation of diagnosis. Fat Embolism the rate of mortality from fat embolism syndrome can be as high as 8%. Decreased Urine Output Decreased urine output is a problem frequently seen in both medical and surgical services. Proper management of affected patients depends on your skills in assessing volume status. Absence of urine (anuria) is suggestive of a mechanical obstruction of the bladder outlet or a blocked Foley catheter. Abdominal pain is a clue to the possible presence of a distended bladder, as may be seen with bladder outlet obstruction. If the patient has a Foley catheter in place, the assessment of urine output can usually be assumed to be accurate. If not, you must ensure that the total volume of voided urine has been collected and measured. If a Foley catheter is in place and the patient is anuric, ask the nurse to flush the catheter with 20 to 30 mL of normal saline to ensure patency. Clogging of Foley catheters with sediment is a common problem, and it is solved easily before a more detailed investigation for decreased urine output is necessary. Elevations in serum urea and creatinine levels can be used as guidelines to assess the degree of renal insufficiency present. Renal artery thrombosis Patient-Related Problems: the Common Calls Postrenal Causes 1. Of the complications of renal failure, hyperkalemia is the most immediately life-threatening because it can lead to potentially fatal cardiac dysrhythmias. A patient who is sick or looks critically ill may have advanced renal insufficiency. However, both these conditions can be present in a patient who deceptively appears well. Caution: A resting tachycardia alone may be indicative of decreased intravascular volume. Selective Physical Examination Examine for prerenal (volume status), rena~ or postrenal (obstructive) causes of decreased urine output. Management I Your job becomes simpler when you can find a prerenal or postrenal cause for decreased urine output Prerenal Cause First ensure that the intravascular volume is normal. Patient-Related Problems: the Common Calls If the patient has volume depletion, replenish the intravascular volume with normal saline. Postrenal Cause Obstruction in the lower urinary tract can be adequately ruled out by passage of a Foley catheter into the bladder. If the bladder outlet has been obstructed, the initial urine volume on catheterization is usually more than 400 mL, and the patient experiences immediate relief. After catheterization, watch for the development of postobstructive diuresis by monitoring urine volume status carefully for the next few days. If a Foley catheter is already in place, ensure that flushing the catheter with 20 to 30 mL of normal saline allows free flow of fluid from the bladder. This maneuver helps rule out an intraluminal blockage of the Foley catheter as a cause of postrenal obstruction. The presence of a Foley catheter in the bladder rules out obstruction of only the lower urinary tract. If the preceding two steps fail to restore urine output, a renal ultrasound examination should be ordered first thing in the morning to search for obstruction of the upper urinary tract. Although bilateral ureteric obstruction is rare, additional useful information, such as documentation of the presence of both kidneys and an estimate of renal size, may be obtained. Renal Cause If prerenal and postrenal factors are not responsible for the decrease in urine output, you must investigate renal causes. Are any of the following five life-threatening complications of decreased urine output present Uremic encephalopathy: manifested by confusion, stupor, or seizures and managed by dialysis. If seizures occur, they should be managed as outlined in Chapter 23 until dialysis can be initiated. Uremic pericarditis: suggested by the presence of pleuritic chest pain, pericardia! Potassium-sparing diuretics (eplerenone, spironolactone, triamterene, amlloride) c. If arninoglycosides are required, doses will need to be adjusted on the basis of serum levels. Although the mortality rate in this condition is higher than that in nonoliguric renal failure, there is little evidence to support efforts to convert oliguric to nonoliguric renal failure through the aggressive use of diuretics. If the patient does not pass urine despite high doses of diuretics, the indications for urgent dialysis are as follows: i. If the patient is in renal failure and if one or more of these conditions are present, request an urgent nephrology consultation about dialysis for the patient. Uremic encephalopathy: keep the patient calm and on bed rest until dialysis can be initiated. Once the questions have been addressed, you can consider possible renal causes of decreased urine output. The majority of renal causes are diagnosed from the history, physical examination, and laboratory findings. Urine Dipstick Test for Blood and Protein Urine dipsticks are a rapid and relatively sensitive (>80%) method for detecting hematuria. Microscopic examination of the urine will differentiate between hematuria and hemoglobinuria. White blood cell casts, particularly eosinophil casts, may be observed in cases of acute interstitial nephritis. Urine for Eosinophils Ask for this test if acute interstitial nephritis is suspected. In most cases, beyond these simple tests, no further investigation is required during the night. For any suspected renal cause of decreased urine output, however, ensure that prerenal and postrenal factors are not additional contributors to the poor urine output All medications that the oliguric or anuric patient is receiving should be reviewed, and any potential nephrotoxins should be discontinued the actions of many drugs depend on renal excretion, and dosage adjustment may be required If you are uncertain about the route of excretion of a drug that has been ordered for a patient, it may be safest to withhold the drug until you find out. Diarrhea is always a symptom of another underlying disorder and seldom warrants nonspecific antimotility therapy. During the night, when testing services are not always available, your job is to determine the likely cause of the diarrhea, whether additional investigations should be perfunned, and whether complications have arisen that necessitate treatment. Bloody stools with pus or mucus are suggestive of inftammation, as may be present with infection, inflammatory bowel disease, or ischemic colitis. Moderate or severe abdominal pain is suggestive of ischemic colitis, diverticulitis, or inflammatory bowel disease. If the 84 Diarrhea diarrhea is frequent, severe, or bloody, the patient should be evaluated at the bedside as soon as possible. If the patient is hypotensive, tachycardic, or febrile, he or she should be assessed immediately. Yersinia enterocolitica Vibrioparahaemolyticus(in uncooked shellfish) Plesiomonas shigelloides (in uncooked shellfish) Aeromonas hyrJrophila Iin untreated well water, brackish water) Mycobacterium avium-intracellulare" Mycobacterium tuberculosis" Chlamydia spp. Diarrhea Intravascular volume depletion; electrolyte imbalance Systemic infection Volume depletion and electrolyte disturbances are the reasons that many children in underdeveloped countries die from diarrhea.
